
Abstract
Postpancreatectomy haemorrhage (PPH) is a rare and life-threatening complication that can occur after pancreaticoduodenectomy (PD). Recently, radiological intervention has become a first-line approach for the diagnosis and treatment of late PPH in haemodynamically stable patients. Surgical intervention should be performed in haemodynamically unstable patients. We report the case of a 54-year-old man who underwent PD for ampullary carcinoma. On postoperative day (POD) 20, he developed a late PPH in the context of pancreatic fistula that was accompanied by hypotension and tachycardia. Therefore, emergency relaparotomy was performed, but the bleeding site was not detected due to severe adhesions in the surgical field. Thus, urgent angiography was performed immediately, and active bleeding was detected from the distal part of the proper hepatic artery. Coil embolisation of the proper hepatic artery trunk was successfully performed. No intrahepatic abscess or liver failure was subsequently observed, and the patient left our hospital on POD 27. This case shows that radiological intervention is a first choice for the diagnosis and treatment of haemodynamically stable late PPH and that it also might still be a first choice and also be safer and more effective than surgical intervention even with unstable haemodynamics.
Keywords
Introduction
Pancreaticoduodenectomy (PD) is the standard procedure that is used for resectable ampullary carcinoma, 1 and its complexity leads to an increase in the morbidity rates of postoperative complications, such as intra-abdominal haemorrhage, pancreatic fistula, and delayed gastric emptying. 2
Postpancreatectomy haemorrhage (PPH) is a rare and life-threatening complication after PD, and it is usually caused by arterial bleeding in the context of pancreatic fistula or intraabdominal abscess. In accordance with the International Study Group of Pancreatic Surgery (ISGPS), a late PPH is defined as PPH that occurs more than 24 hours after PD. 3 The morbidity rate of late PPH was reported to be between 6% and 10%, 4 and the mortality rate can be up to 11% to 60%. 5 Urgent reoperation or interventional radiology can both be performed as first-line approaches, but there is no appropriate treatment for PPH.
This paper presents the diagnosis and treatment of a patient with late haemorrhage after PD due to proper hepatic artery rupture.
Case presentation
A 54-year-old man was admitted to the Department of General surgery at the first affiliated Hospital of Chengdu University for jaundice and abdominal pain. The relevant examinations including abdominal computed tomography (CT), magnetic resonance imaging (MRI), and magnetic resonance cholangiopancreatography (MRCP) all suggested the diagnosis of ampullary carcinoma and cholecystolithiasis. In July 2019, the patient underwent laparoscopic cholecystectomy and an exploration of the common bile duct, and a T tube was placed in the duct. After surgery, the patient was admitted to the Liver Surgery Department at our hospital for further treatment.
Laboratory examination revealed the abnormalities that are presented below. Biochemical test results showed the following results: total/direct bilirubin serum level, 56.6/55.0 µmol/L; gamma-glutamyl transpeptidase (GGT) serum level, 716 IU/L; aspartate aminotransferase (AST) serum level, 192 IU/L; and alanine aminotransferase (ALT) serum level, 453 IU/L. Tumour marker test results were as follows: CA199, 52.96 U/mL; and CEA, 4.77 ng/mL. Additionally, abdominal ultrasound (US), contrast-enhanced CT, contrast-enhanced MRI, and upper gastrointestinal (GI) endoscopy suggested a diagnosis of ampullary carcinoma.
Therefore, PD in accordance with Whipple’s procedure with child reconstruction was performed without any significant intraoperative events in August 2019. On POD 2, the patient developed a fever and was treated with broad-spectrum antibiotics. The next day, the patient developed a pancreatic fistula, and the amylase and lipase levels in the drainage fluid were 976 IU/L and >6000 IU/L, respectively. Pancreatic fistula was well tolerated, with effective drainage at the pancreaticojejunostomy and the Winslow foramen, which did not affect the patient’s clinical status. The patient’s subsequent postoperative course was uneventful. Abdominal CT that was performed on POD 11 indicated the presence of a slight fluid collection containing a small amount of gas around the operative field in the abdominal cavity, but there were no signs of abscesses or infected necrosis (Figure 1). Therefore, the patient was discharged at POD 13.
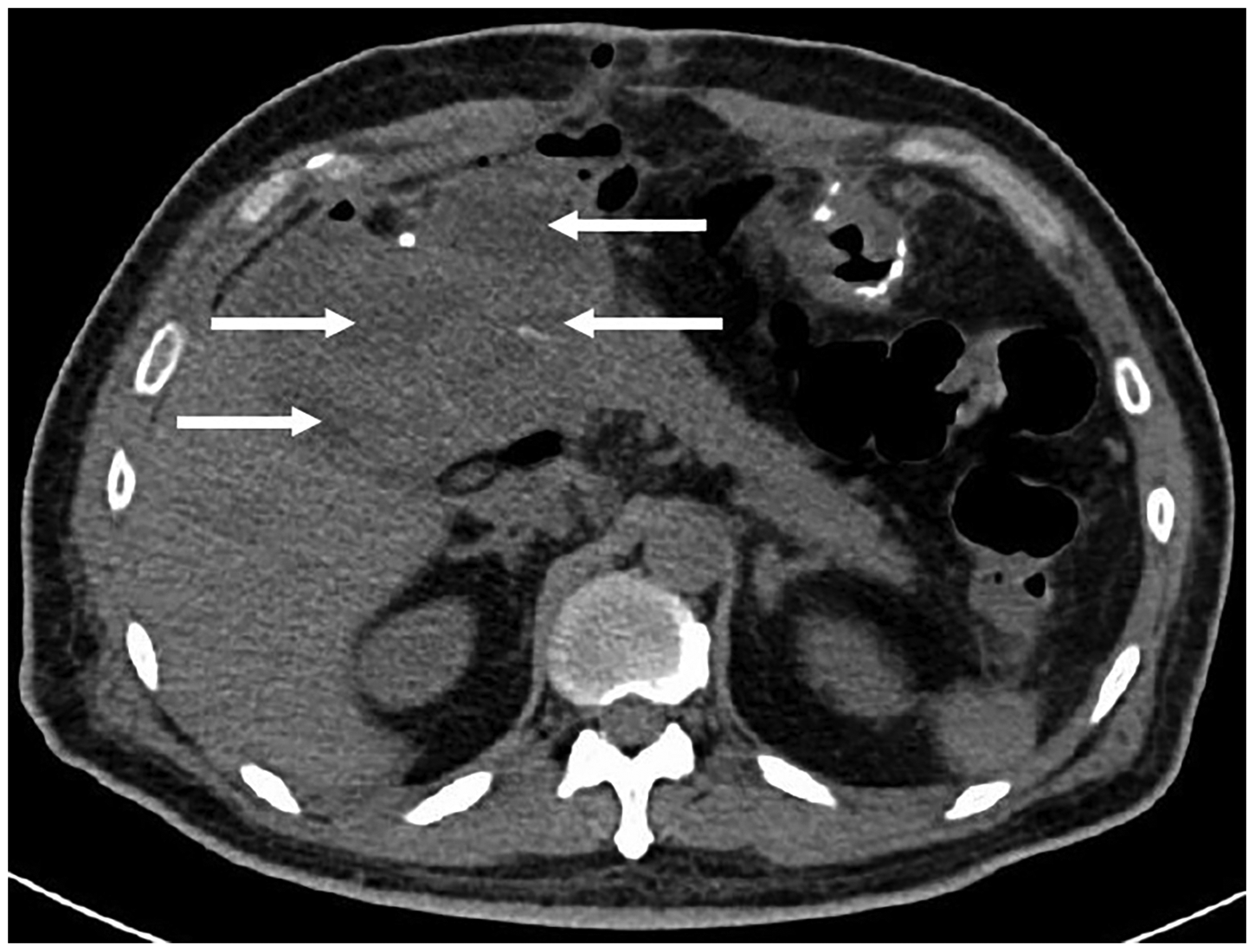
Abdominal computed tomography that was performed on POD 11 indicated the presence of slight fluid collection containing a small amount of gas around the operative field in the abdominal cavity (white arrow) but no signs of abscesses or infected necrosis.
The histopathologic outcome of the operative specimen revealed a 1.5 × 1.0 × 0.5 cm-sized, moderately well-differentiated ampullary carcinoma with perineural, but without microvascular, invasion. No positive lymph nodes were observed.
On POD 17, 500 mL of dark red bloody fluid suddenly drained from the patient’s abdominal drainage tube during forced defecation, so the patient was readmitted to the Liver Surgery Department. The emergency blood routine examination showed that his haemoglobin level was 77 g/L, but the patient’s haemodynamic parameters were stable, and the results of abdominal contrast-enhanced CT were similar to previous findings from POD 11. The other laboratory examination and physical examination showed no significant abnormalities. After haemostasis therapy and transfusions, the patient’s haemoglobin level improved steadily, with no signs of subsequent bleeding. However, at POD 20, the patient’s abdominal drainage suddenly reappeared (approximately 1000 mL of bright red bloody fluid) when his abdominal drainage tube was pulled out by 1 cm. The patient presented severe clinical symptoms, such as hypotension and tachycardia. Emergency exploratory laparotomy was performed because of unstable haemodynamics. Intraoperatively, we found that serious adhesions were present around the surgical area, which might lead to more severe bleeding if they were forced to separate. Thus, the operation was stopped, and we immediately communicated with family members about the patient’s condition and obtained consent for angiography. Angiography showed that the source of bleeding was in the distal part of the proper hepatic artery (Figure 2), so several pushable coils were successfully implanted with no bleeding and no complications (Figure 3).

Angiogram results showed that the source of bleeding (black arrow) was in the distal part of the proper hepatic artery.

Angiogram results showed that the pushable coils (black arrow) were placed in the distal part of the proper hepatic artery, with no extravasations of contrast agent.
No rehaemorrhage occurred after coil embolisation. The abdominal contrast-enhanced CT before discharge showed no active bleeding and uneven decreased density of the left lobe of the liver; there were no obvious signs of ischaemic necrosis. Moreover, the artery phase showed high-density striped blood vessels in the liver (Figure 4). After interventional embolisation, the hepatic functions of the patient were not markedly abnormal, and he was discharged on POD 27. At the 1-month follow-up, the patient’s liver function had returned to normal, and there were no signs of ischaemic necrosis in the liver.

(a) Abdominal contrast-enhanced computed tomography after embolisation showed the presence of metal artefacts (black arrow) that were created by coils and the density of the left lobe of the liver decreased unevenly (white arrow). (b) The artery phase showed high-density striped blood vessels (black arrow) in the liver.
Discussion
PPH is a rare and life-threatening postpancreatectomy complication, and its occurrence leads to a high mortality rate. 3 Late PPH is usually related to pancreatic fistula, bile leak, or intraabdominal abscess. The pathogenesis of late PPH includes enzymatic digestion, local infection with secondary vascular wall erosion, or vascular injury at the time of resection. 6 In our case, the pathogenesis of the late PPH was more likely enzymatic or infectious erosion of the proper hepatic artery wall secondary to postoperative pancreatic fistula. Therefore, proper ligation of bleeding vessels and abdominal drainage is necessary to prevent late PPH.
Ansari et al. 7 reported that approximately 70% of patients with late PPH have experienced sentinel bleeding, which is defined as a minor loss of blood via a surgical drainage tube or gastrointestinal tract, with asymptomatic intervals of at least 12 hours until haemorrhagic shock. Tien et al. 8 suggested performing angiography for sentinel bleeding after every PD, and the embolisation of any detectable bleeding point can significantly reduce bleeding-related mortality without serious angiography-related complications. Sometimes, sentinel bleeding is the only clinical symptom before a severe PPH, which was observed in the patient who is described in this case report. At that time, we advised the patient to undergo further angiography, but the patient and his family refused this invasive examination because the patient’s vital signs were stable and no abnormal abdominal CT was performed. Thus, this case once again suggested that early detection, diagnosis, and treatment of sentinel bleeding are necessary to prevent late PPH.
Recently, some studies have shown that surgical intervention should be performed in haemodynamically unstable patients with late PPH, and radiological intervention should be performed in haemodynamically stable patients with late PPH. However, it is unclear which emergent intervention provides the optimal strategy for late PPH.9–11 In our case, we initially chose emergency relaparotomy because of the large amount of bleeding and relative haemodynamic instability. Several authors have shown that surgical intervention can stop bleeding by ligation, repair, or reconstruction of blood vessels.12–14 However, the severe adhesions surrounding the operating field prevented us from locating the bleeding site. Thus, emergency angiography was performed immediately, and the bleeding point was detected at the distal part of the proper hepatic artery. Radiological intervention includes coil embolisation and stent implantation, both of which can effectively manage late PPH. 15 Asai et al. 16 reported that stent implantation might be preferable to coil embolisation because stent implantation was more likely to ensure blood perfusion and reduced related complications. However, because we did not have a suitable arterial stent at that time and the patient was in critical condition, we performed urgent coil embolisation and successfully stopped the bleeding. Some studies have shown that the success rate of radiological intervention was 80% after one procedure, which could be repeated if there is repeated bleeding. Additionally, radiological intervention could reduce the mortality of late PPH compared with surgical intervention.17–19 Complete obstruction of the proper hepatic artery trunk might lead to liver infarction, intrahepatic abscess, biliary ischaemia, or liver failure, and the incidence and mortality for these complications is 45% and 30%, respectively. 20 Fortunately, the results of the postoperative follow-up showed that there was no obvious ischaemic necrosis or abnormal liver function, which may be because there are at least 26 possible routes of collateral artery circulation that can supply the liver. The decrease in the density of the left lobe of the liver may be caused by cutting off the part of collateral circulation that supplies the left lobe of the liver during PD.21,22
In conclusion, this case illustrates that radiological intervention is a first choice for the diagnosis and treatment of haemodynamically stable late PPH, and it might still be a first choice along with being safer and more effective than surgical intervention even when the patient’s haemodynamic parameters are unstable. Surgical intervention might be risky and reoperation might encounter fragile tissue and severe adhesions in the surgical area, which could result in the inability to find the bleeding site, especially in the case of a pancreatic fistula. Surgical intervention might be used as an alternative treatment when radiation intervention is negative or if it fails.
Footnotes
Author contributions
All authors made substantial contributions to conception and design, data acquisition, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics and informed consent
The West China Hospital Ethics Committee approved this report, and this work was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patient for publication of this case report.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.