
Abstract
Meckel’s diverticulum (MD) is a relatively common true congenital diverticulum on the ileum. Bleeding caused by polypoid hyperplasia of ectopic gastric mucosa in MD is rare. A 14-year-old Chinese boy presented with intermittent melena and haematochezia for 1 month. Laboratory data showed normocytic anaemia. Gastroscopic findings were normal. The patient underwent exploratory laparotomy without bowel preparation on day 2 because of sudden haematochezia and decreased haemoglobin. Intraoperative colonoscopy revealed inflammatory changes in the terminal ileal mucosa with diffuse haemorrhage. Melena with decreased haemoglobin recurred 20 days after the first operation. Computed tomography (CT) and angiography revealed a tubular lesion that was localised in the right lower abdominal quadrant. Single-photon emission computed tomography/computed tomography (SPECT/CT) fusion imaging with 99m-technetium pertechnetate confirmed moderately increased uptake in the distal ileum. Retrograde double-balloon enteroscopy (DBE) showed a diverticulum with prominent mucosal polypoid hyperplasia at an insertion depth of 100 cm from the anastomotic stoma. Diverticulectomy and end-to-end anastomosis were performed, and MD was confirmed by a histopathological examination. The patient’s postoperative recovery was uneventful during the 2-month follow-up. MD with polypoid hyperplasia of ectopic gastric mucosa is rare. Complementary use of DBE and SPECT/CT can accurately diagnose MD by providing anatomical and functional information.
Keywords
Background
Meckel’s diverticulum (MD) is a common congenital malformation of the gastrointestinal tract that occurs in 0.14% to 4.5% of the population. 1 MD is caused by faulty involution of the vitelline duct, which is located 60 to 100 cm from the ileocaecal valve, during the fifth week of gestation. 2 MD is most often asymptomatic, but approximately 4.2% to 6.4% of cases are diagnosed on the basis of complications. 3 Life-threatening complications include bleeding, obstruction, and inflammation. The most common clinical presentation is bleeding because of the existence of ectopic gastric mucosa, which occurs in 25% to 50% of patients.4,5 A preoperative diagnosis of MD is challenging because of a non-specific array of symptoms. Conventional imaging methods, including X-ray, ultrasonography, computed tomography (CT), and angiography, are seldom beneficial for a preoperative diagnosis.6–11 99m-Technetium pertechnetate scintigraphy is a useful non-invasive technique because 99m-technetium pertechnetate is taken up by ectopic gastric tissue in MD. This method has a higher specificity (95%) and sensitivity (80% to 90%) in children than in adults.12,13 Single-photon emission computed tomography/computed tomography (SPECT/CT) can precisely locate the lesion. 14 With improvements in the double-balloon endoscopy (DBE) technique, DBE is considered to be a safe and dependable procedure for diagnosing MD in children as well as adults because MD can be directly observed.15–18 In this report, we describe a rare case of MD with polypoid hyperplasia of ectopic gastric mucosa that was diagnosed using a combination of DBE and 99m-technetium pertechnetate with SPECT/CT.
Case presentation
A 14-year-old Chinese boy attended our hospital with chief complaints of intermittent melena and haematochezia for 1 month. His medical history was unremarkable. Laboratory data showed normocytic anaemia, with haemoglobin 7.5 g/L, and positive stool occult blood 1 month previously. Other biochemical analyses, including tumour marker tests, urinalysis, coagulation function, and liver and renal function, showed normal results. His vital signs were stable, and physical examination revealed a soft abdomen without tenderness. Gastroscopy revealed no abnormality. Because of sudden haematochezia and decreased haemoglobin, the patient underwent exploratory laparotomy without bowel preparation on the secondary day in the hospital. Intraoperative colonoscopy revealed inflammatory changes in terminal ileal mucosa with diffuse haemorrhage. Ileocecectomy with anastomosis of the terminal ileum and ascending colon was performed. Melena with decreased haemoglobin (6.9 g/L) recurred 20 days after the first operation. The patient was managed with fasting, intravenous fluids, and transfusion. Small bowel bleeding was suspected. Capsule colonoscopy was performed, but no definite bleeding was identified. Contrast abdominal CT revealed a contrast-enhanced tubule that was localised in the right lower abdominal quadrant (Figure 1a, b). Angiography showed tortuous vessels and vascular death originating from the ileocolic artery, which arises from distal branches of the superior mesenteric artery (Figure 1c). 99m-Technetium pertechnetate scintigraphy revealed a faint focal area of uptake that appeared simultaneously with the stomach in the right lower abdominal quadrant (Figure 2a, b). SPECT/CT fusion imaging confirmed moderately increased uptake in the distal ileum (Figure 2c, d, e). Two months later, retrograde DBE was performed and showed a diverticulum with prominent mucosal polypoid hyperplasia at an insertion depth of 100 cm from the anastomotic stoma (Figure 3a, b). Based on these imaging findings, MD (4.0 × 5.0 cm) was located in the ileum and a 100-cm anastomotic stoma was found using laparoscopy (Figure 3c). Diverticulectomy and end-to-end anastomosis were applied. Histology revealed polypoid hyperplasia of ectopic gastric mucosa in MD (Figure 3d). The patient’s postoperative recovery was uneventful during the 2-month follow-up. This case report was approved by the Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University. Written informed consent for publication was obtained from the patient, and the patient’s data were anonymised. We followed the CARE guidelines.
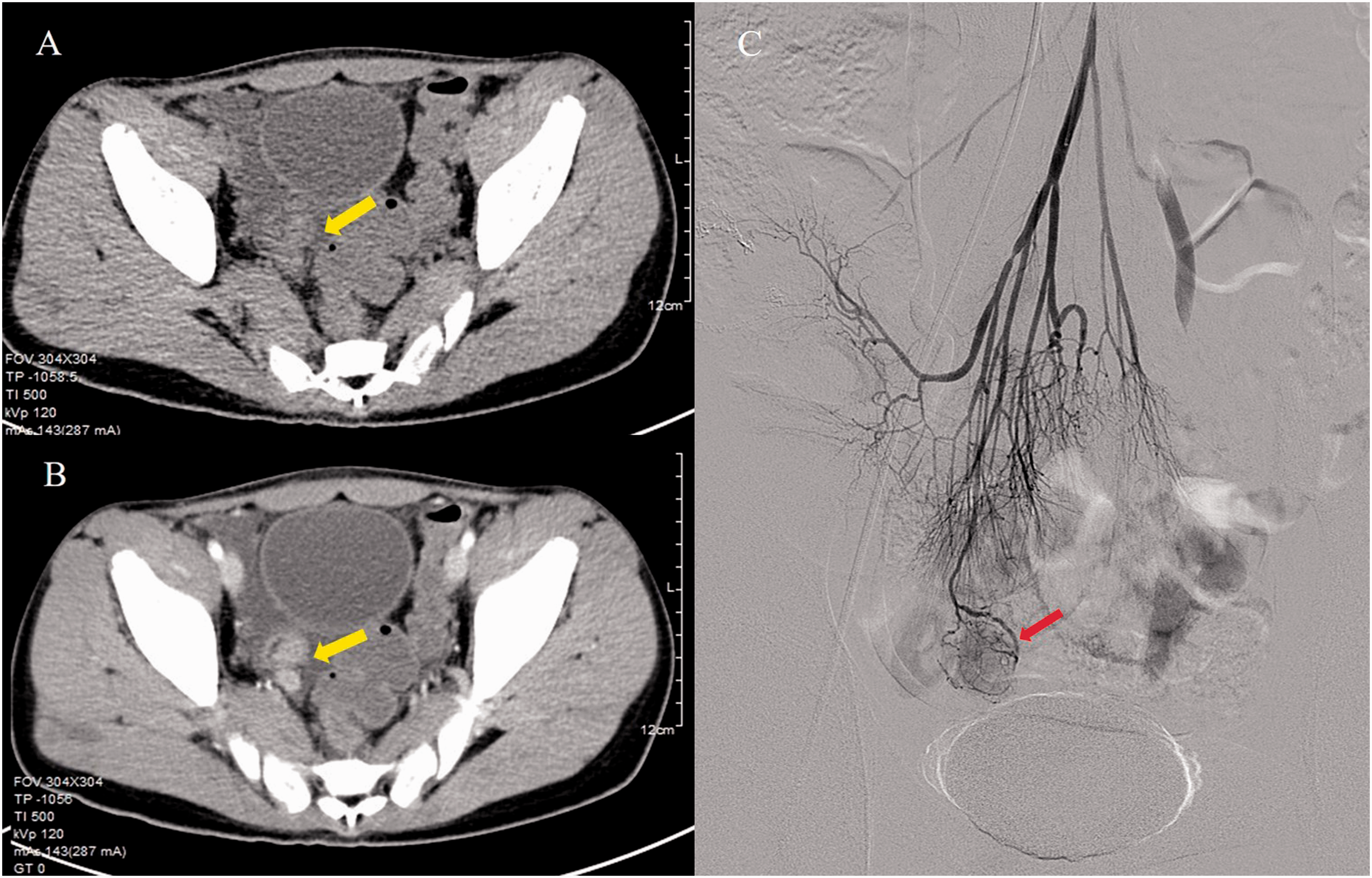
Contrast-enhanced computed tomography (CT) showing abnormal thickening (a) and a contrast-enhanced lesion (b) in the distal ileum with mild ascites. Superior mesenteric arteriography (c) showing tortuous vessels and vascular staining the terminal branch of the ileocolic artery.
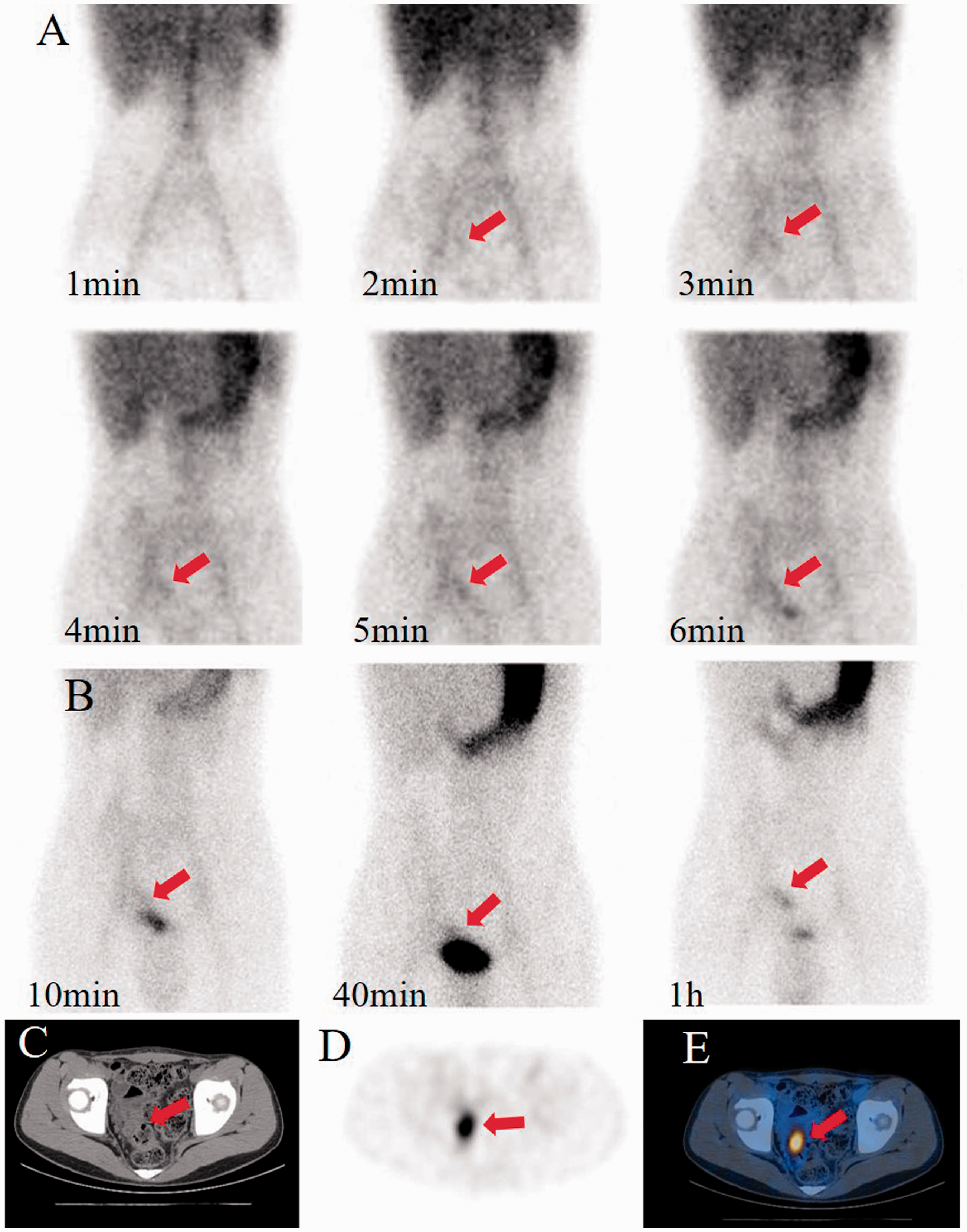
99m-Technetium pertechnetate scintigraphy showing a subtle focus of activity within the lower abdominal quadrant in dynamic (a) and delayed (b) images that increases simultaneously with that in the stomach. SPECT/CT infusion imaging (c, CT; d, SPECT; d, fused SPECT/CT) showing a focal concentration localised anatomically to the tubular structure in the right abdomen.
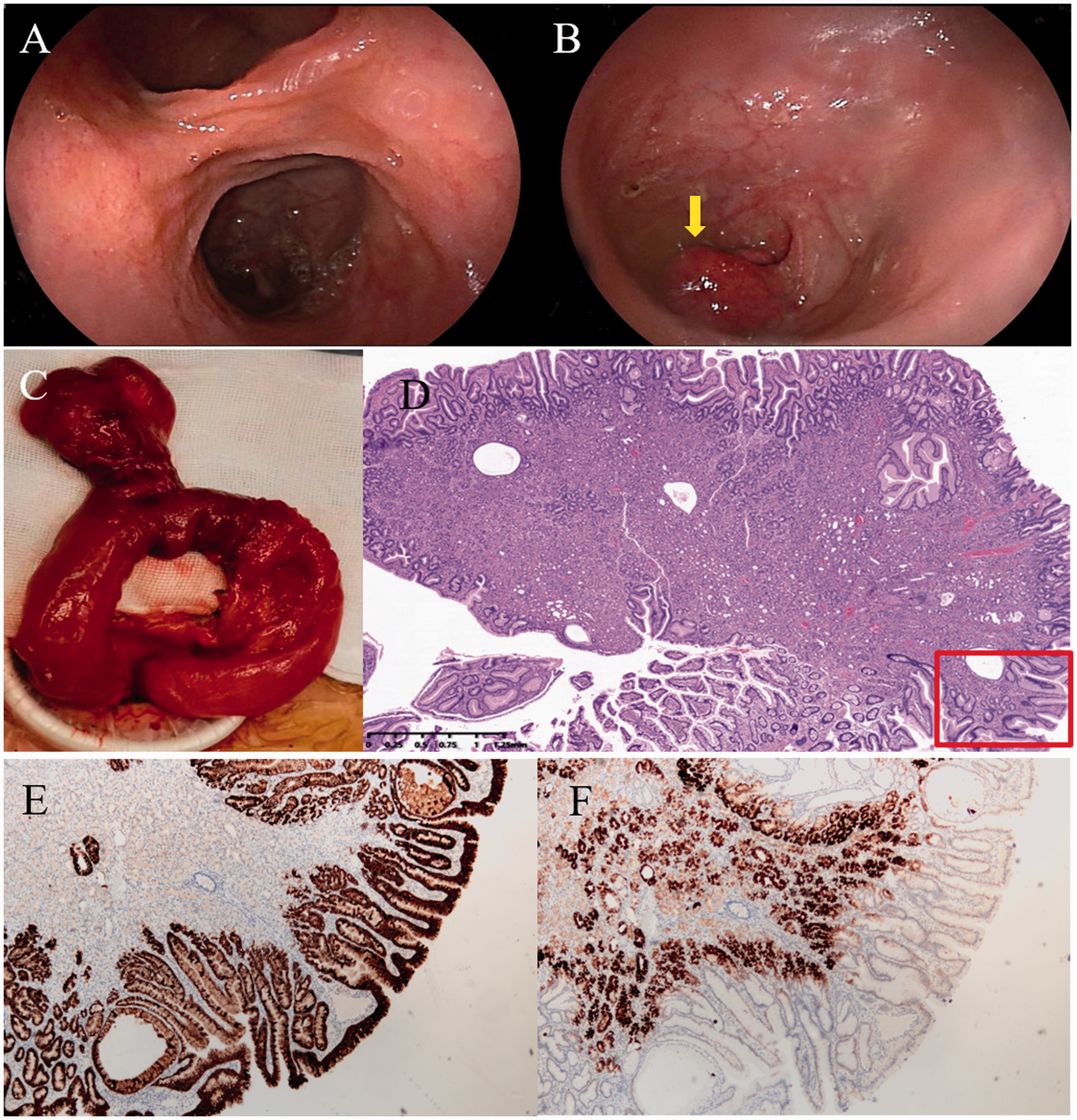
Retrograde DBE showing a double lumen sign within 1 m proximal to the anastomotic stoma; the upper lumen contains a diverticulum (a). A protruding poly-like lesion was noted in the diverticulum (b); Operative findings showing a diverticulum located on the antimesenteric border of the ileum within 100 cm of the anastomotic stoma (c). Pathological (d, HE-stained magnification ×20) findings showing the polypoid lesion with ectopic gastric mucosa located adjacent to the intestinal mucosa. Immunohistochemical staining for mucin-5AC (e, magnification ×50) and mucin-6 (f, magnification ×50) was positive.
Discussion and conclusions
This is a rare case report in which we describe the complementarity of DBE and SPECT/CT with 99m-technetium pertechnetate in a child, which revealed polypoid hyperplasia of ectopic gastric mucosa within MD. MD was first illustrated as the embryological origin of a true diverticulum in 1809. 19 The prevalence of MD is 0.14% to 4.5%, with a male-to-female ratio of 1.7 to 2.4:1, and is most often asymptomatic throughout the patient’s lifetime.1,3,20 Zani et al. 21 estimated that 4% of patients with MD had symptoms, and 3% would require surgery. MD diagnosis is challenging because symptoms are mainly caused by bleeding, obstruction, or diverticulitis, and they are usually non-specific.
Conventional imaging modalities, such as X-ray, ultrasonography, CT, and angiography, are not accurate. Chatterjee et al. 22 reported that only 5.7% of MD cases are diagnosed preoperatively. In our case, the conventional imaging modalities and laparotomy did not reveal MD. Physicians’ knowledge of MD (i.e., anatomy, embryology, clinical presentation, and complications) is crucial. Our patient was diagnosed by performing 99m-technetium pertechnetate SPECT/CT and DBE. Ectopic gastric mucosa is considered to be the major cause of bleeding because acidic secretion from gastric tissues causes ulceration of the adjacent normal ileal mucosa. 99m-Technetium pertechnetate scintigraphy is a specific imaging tool that can be used to detect MD-containing ectopic gastric mucosa. Ectopic gastric tissue can take up 99m-technetium pertechnetate, and it is present in 24.2% to 71% of symptomatic MD cases. 23 A sensitivity of 80% to 90% and a specificity of 90% are reported in paediatric patients.12,13 In adults, the sensitivity is only 62.5% because ectopic gastric mucosa decreases in older patients. 23 The sensitivity of 99m-technetium pertechnetate scintigraphy can be increased by imaging with SPECT/CT and administering glucagon and H2 antagonists. 24 False-positive results may be caused by bowel inflammation, vascular lesions, carcinoma, or an anomaly of the urinary system. Negative scan results may occur in some patients with no/insufficient gastric mucosa or diluted radioactivity due to haemorrhage. 25 99m-Technetium pertechnetate with SPECT/CT revealed a positive result in the ileum of this patient. We also performed DBE because it is an excellent diagnostic modality and a safe and reliable procedure. DBE can be used to directly observe an MD. After identifying ectopic gastric mucosa, ulceration and a ring-like scar appearance can improve diagnostic confidence in cases of haemorrhagic MD. 18 A diagnosis of MD was made in our case because DBE showed a double lumen and polypoid hyperplasia of ectopic gastric mucosa in the diverticulum. When MD is inverted into the ileum, it may present as an intraluminal polypoid lesion. Polypoid hyperplasia of ectopic gastric mucosa in MD is rare. To the best of our knowledge, only three cases have been reported.26–28 The development of polypoid hyperplasia of ectopic gastric mucosa in MD has not yet been elucidated. It is speculated that abnormal peristaltic movements from MD and chronic inflammation may play important roles in the development of polypoid hyperplasia.
Surgical management should be decided on the basis of patient-specific factors. Complicated MD needs to be treated by resection. In this report, we described a rare case of MD with polypoid hyperplasia of ectopic gastric mucosa. DBE and SPECT/CT with 99m-technetium pertechnetate can be used in a complimentary manner to prompt the recognition and accurate diagnosis of MD because they provide anatomical and functional information.
Footnotes
Acknowledgements
This study was supported by the Science and Technology Panning Project of Zhejiang Province, China (2017KY061). The authors would like to thank Dr. Hao Chen and Dr. Jian-guo Zhong for their good comments on this work.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.