
Abstract
Primary thyroid hemangioma is an extremely rare clinical disease. Only 31 cases have been reported to date according to a PubMed search, and most were postoperatively diagnosed by pathologic examination. Ultrasonography is the first-line imaging modality for thyroid disease screening. However, preoperative ultrasonic diagnosis of thyroid hemangioma has been rarely reported. We herein describe a 24-year-old woman with a painless mass in the left thyroid lobe. Routine ultrasound (US) and contrast-enhanced US (CEUS) were performed. Routine US revealed an anechoic tumor with linear echogenic septal lines and compressibility. CEUS showed a characteristic “slow in and slow out” pattern of contrast filling and perfusion. Based on the combined findings of routine US and CEUS, the initial diagnosis was thyroid venous hemangioma. Postoperative pathological examination demonstrated multiple irregular dilated vessel lumens filled with red blood cells and multiple hemorrhagic zones. Immunohistochemical staining showed positivity for CD31 and smooth muscle actin.. Overall, this case showed US characteristics of a rare case of thyroid hemangioma, which is of importance for preoperative planning to avoid a large amount of blood loss during surgery. This case together with our literature review will help radiologists to bridge the knowledge gap of thyroid hemangioma, especially at the initial US screening.
Keywords
Introduction
A hemangioma is a commonly observed benign vascular neoplasm characterized by a relatively irregular proliferation of tiny vessels. It has a predilection for the head and neck as well as the liver and other visceral organs 1 , 2 ; however, it is extremely rare in the thyroid. Pickleman et al. 3 reported the first case of a thyroid hemangioma in 1975, and only 31 case reports of this condition have since been published worldwide. 2 Ultrasonography is the first-line imaging modality for thyroid disease screening. However, preoperative ultrasonic diagnosis of thyroid hemangioma has been rarely reported, and most cases were postoperatively diagnosed according to the pathology results. We herein report a case of a thyroid hemangioma diagnosed by conventional ultrasound (US) combined with contrast-enhanced US (CEUS) and review the associated literature to help radiologists increase their knowledge of thyroid hemangioma.
Case presentation
A 24-year-old woman presented with a palpable painless mass in the left thyroid lobe. The mass had initially appeared 2 months previously. The patient had no swallowing discomfort, hoarseness, palpitation, shortness of breath, or other clinical manifestations. Her physical examination findings and laboratory test results were normal.
Conventional US examination revealed an anechoic tumor with numerous linear echogenic septal lines in the ventral left thyroid lobe. The tumor had a three-dimensional size of 36 × 12 ×15 mm (Figure 1(a)). Unusual internal flow was captured by color Doppler flow imaging (CDFI) of the tumor, which presented a vein-like velocity curve with blood flowing into the left inferior thyroid vein. The tumor significantly shrank when compressed with the ultrasound probe (positive compression test), but no significant increase in blood flow was observed by CDFI (Figure 1(b)). No other abnormalities were detected in the bilateral neck. No lymph node enlargement was found.

Ultrasound images of the thyroid hemangioma. (a) Two-dimensional ultrasound showed a mixed tumor in the left thyroid lobe. (b) Color Doppler flow imaging showed unusual internal flow of the tumor. (c) Contrast-enhanced ultrasound showed high uneven enhancement of the tumor. (d) The tumor significantly shrank after pressure was applied with the ultrasound probe (positive compression test). (e) Rapid refilling with contrast agent occurred in the tumor when the probe was released, together with obvious inhomogeneous enhancement. (f) Contrast enhancement had almost subsided in the surrounding thyroid tissue at 5 minutes 14 seconds after injection, while the tumor still exhibited enhancement. (g) The time intensity curve showed a typical “slow in and slow out” pattern.
CEUS showed obvious enhancement of the thyroid at 11 s with subsequent perfusion of the tumor at 13 s after intravenous administration of a contrast agent (SonoVue; Bracco, Milan, Italy). The tumor exhibited slightly inhomogeneous enhancement compared with the surrounding thyroid tissues, and twisted vessels were detectable within the tumor (Figure 1(c)). The tumor significantly shrank when compressed by the US probe (Figure 1(d)). Once the probe was released, the tumor showed rapid filling of contrast agent and high enhancement (Figure 1(e)). Contrast enhancement had almost subsided in the surrounding thyroid tissue at 5 minutes 14 s after injection, while the tumor still exhibited enhancement (Figure 1(f)). The time intensity curve showed the typical “slow in and slow out” enhancement pattern (Figure 1(g)). Based on the combined findings of routine US and CEUS, our initial diagnosis was thyroid venous hemangioma.
A computed tomography examination was performed to validate our initial diagnosis. Unenhanced images showed left thyroid lobe enlargement and uneven low-density lesions within the gland. The lesions measured about 16 × 15 mm in the axial image and had an unclear boundary with the surrounding thyroid tissue (Figure 2(a)). In the arterial phase after intravenous administration of contrast agent, the lesions exhibited moderately inhomogeneous enhancement that was inferior to the enhancement of the surrounding thyroid tissues (Figure 2(b)).

Computed tomography images of the thyroid hemangioma. (a) Neck computed tomography showed a low-density lesion in the left thyroid lobe. (b) Contrast-enhanced axial images showed uneven enhancement with linear strengthening of the tumor.
Postoperative pathologic examination showed numerous proliferative vessels within the lesion; multiple irregular, dilated vessel lumens filled with red blood cells; and multiple hemorrhagic zones (Figure 3(a)). Immunohistochemistry showed CD31 positivity for proliferative vessels (representative staining images are shown in Figure 3(b)); D240 negativity, fli-1 positivity, CD34 positivity, and smooth muscle actin positivity (representative staining images are shown in Figure 3(c)); and Ki67 positivity. These pathological results finally confirmed the initial diagnosis of thyroid vein hemangioma.
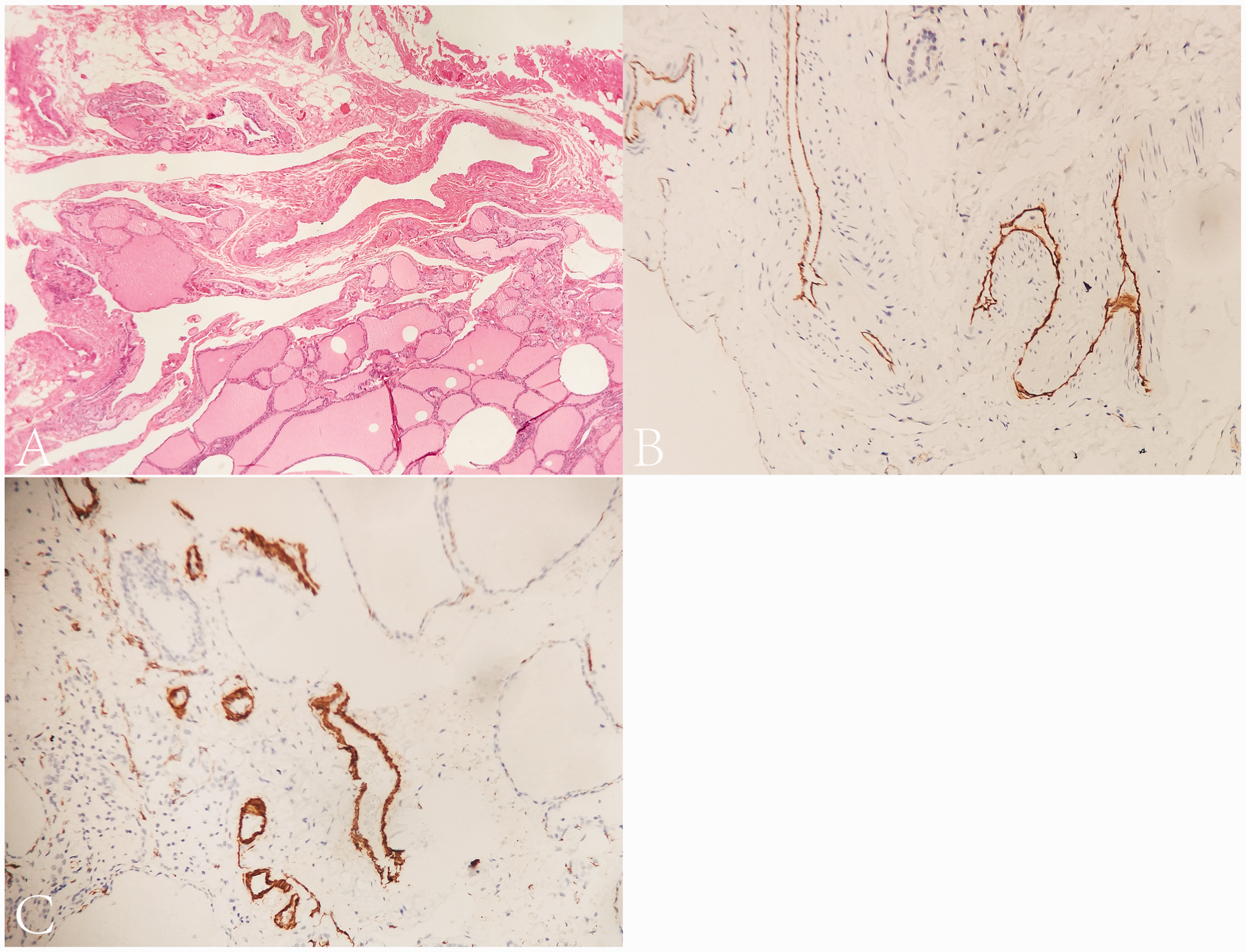
Microscopic view of the thyroid hemangioma. (a) The lesion consisted of multiple irregular, dilated vessel lumens filled with red blood cells and hemorrhagic zones (hematoxylin and eosin, ×50). (b, c) Immunohistochemical staining showed that the hemangioma was strongly positive for CD31 and smooth muscle actin (streptavidin–peroxidase, ×200).
Discussion and literature review
A hemangioma is a benign tumor caused by vascular endothelial cell proliferation or vascular malformation and is histologically classified as synovial, cavernous, capillary, venous, racemose, or arteriovenous. 1 , 2 Hemangiomas most commonly occur in the skin, mouth, and liver, while those in the thyroid are extremely rare. To date, only 31 cases of thyroid hemangioma have been reported; of these, 23 were cavernous hemangiomas, 3 were capillary hemangiomas, 2 were venous hemangiomas, and 3 had an unknown pathology. 2 Most thyroid hemangiomas are secondary conditions associated with previous fine needle aspiration (FNA) procedures or thyroid injury. 4 Soft tissue edema and organization of hematomas lead to proliferation of blood vessels and fibrosis, similar to the generation of a cavernous hemangioma. 5 However, our patient had no history of FNA or other procedures involving her thyroid; therefore, our initial suspicion was a primary thyroid hemangioma.
Preoperative imaging diagnosis is important for patients with thyroid hemangiomas because the abundant rete vasculosum within the tumor may lead to severe intraoperative hemorrhage. For example, more than 2 L of blood loss was reported during surgical treatment of a thyroid hemangioma. 3 Another report emphasized the importance of ensuring that the integrity of a thyroid hemangioma is maintained to minimize blood loss during surgery. 6 Therefore, initial imaging diagnosis is crucial for both surgical planning and ensuring a good prognosis.
Magnetic resonance imaging, digital subtraction angiography, and single-photon emission computed tomography can be used to diagnose hemangioma by a pattern of heterogeneous enhancement or twisted enhancement. 7 , 8 The emergence of a Tc-99m-labeled pool of red blood cells may also be a sign of hemangioma. 7 Among all imaging modalities, US is the most preferable for initial screening of thyroid diseases. In the present case, routine US showed an anechoic tumor with linear echogenic septal lines and compressibility, while CEUS showed a “slow in and slow out” enhancement pattern. These findings confirmed our initial diagnosis of thyroid hemangioma. Although FNA is essential for the diagnosis of thyroid tumors in most cases, 9 the value of FNA for thyroid hemangioma remains controversial. FNA may pick up only blood components rather than thyroid follicular cellular components, 4 , 7 , 9 , 10 which are not sufficient for a diagnosis of hemangioma. It is difficult to differentiate a hematic puncture with vascular malformation from a traumatic puncture. 4
To further understand the US characteristics of thyroid hemangioma, we searched the literature in PubMed and found eight reports describing the US diagnosis of thyroid hemangioma.2,6,9–14 The sonographic characteristic of thyroid hemangiomas included heterogeneous and hypoechoic tumors with clear boundaries and different shapes. The tumors usually had internal multiple linear septations due to the presence of multiple vascular channels. 11 Additionally, the slow blood flow and dilated vascular channels of these tumors predispose to thrombosis and phlebolith formation; thus, the tumors also show heterogeneous echo and calcification. 14 , 15 Another sonographic characteristic of a superficial hemangioma is compressibility of the blood-filled lesion unless it is fully thrombosed. 11 In our case, the sonographic characteristics were an anechoic tumor with linear echogenic septal lines and a positive compression test, which were very similar to previous reports. However, the internal flow of the tumor together with the lack of a significant increase of blood flow on CDFI after compression may have been due to the venous blood supply causing relatively slow blood flow. 16 We performed CEUS to further clarify the perfusion pattern. CEUS confirmed extremely slow blood flow in the anechoic area, and the characteristic “slow in and slow out” enhancement pattern was clearly shown. The regression occurred significantly later in the tumor than in the surrounding thyroid tissue, which was consistent with the angiographic findings of venous hemangiomas in other tissues. 17 , 18 The presence of characteristic linear echogenic septal lines on US, as shown in our case, may be related to multiple irregular and dilated vessel lumens. Immunohistochemical staining finally showed positive expression of proliferative vessels (CD31) and a marker of vascular smooth muscle (smooth muscle actin), and the diagnosis of hemangioma was finally confirmed.
Overall, this case showed the US characteristics of a rare case of thyroid hemangioma, which is of importance for preoperative planning to avoid a large amount of blood loss during surgery. Moreover, this case together with our literature review will help radiologists to bridge the knowledge gap of thyroid hemangioma, especially at the initial US screening.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement and informed consent
This study was approved by the Ethics Committee of Jiading District Central Hospital Affiliated Shanghai University of Medicine & Health Science (No. JDKW-2016-W12). This study was conducted in accordance with the Declaration of Helsinki. The patient signed an informed consent form for the operation (Supplemental Figure 1).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Key Medical Discipline of Jiading District, Shanghai (No. 2017ZD04).
Supplemental material
Supplemental material for this article is available online.