
Abstract
Seminoma accounting for approximately 98% of malignant testicular tumours and it typically presents as a painless, palpable solid mass in the testis. Seminomas presenting only as a solitary neck mass are very rare. This case report describes a previously healthy 35-year-old male that presented with a 3-month history of the incidental discovery of a mass in his right neck. He had no testicular symptoms. He underwent neck ultrasound, contrast-enhanced ultrasound, computed tomography and positron emission tomography. Serum human chorionic gonadotropin (3.90 mIU/ml) was raised and alpha-fetoprotein (3.79 ng/ml) was within normal limits. Clinical examination and imaging examinations did not find any suspicious signs of testicular cancer. Biopsy from the neck mass confirmed the diagnosis of metastatic seminoma. The case report presents the ultrasound and contrast-enhanced ultrasound characteristics of seminoma and provides an update of the literature regarding this very rare metastatic site for seminomas.
Introduction
Testicular germ cell tumours comprise only 1–2% of all male cancers but represent the commonest solid malignancy in 15–35 year olds.1–3 According to 2016 World Health Organization classification of Tumours of the Urinary System and Male Genital Organs, 4 germ cell tumours fell mainly into two classifications: derived from germ cell tumours in situ (GCNIS) and not related to GCNIS. Seminoma is a tumour derived from GCNIS. The highest incidence of seminoma is in those aged 34–45 years old. 5 Seminoma accounts for approximately 98% of malignant testicular tumours and the proportion of cervical metastasis is approximately 15%. 6 An asymptomatic mass in the neck is the initial manifestation in 5% of patients. 6 Seminoma typically presents as a painless and palpable mass in the testes. 7 Fewer patients with seminoma demonstrate epididymal orchitis with testicular swelling and mild discomfort. 8
Contrast-enhanced ultrasound (CEUS) is considered to be a revolutionary breakthrough in the history of ultrasound. The ultrasound contrast agents are microbubbles similar to red blood cells, which cannot enter the tissue space through the vascular endothelium, thus providing good vascular tracers. 9 CEUS can evaluate tumour microvascular perfusion, provide complementary information for conventional ultrasound and be helpful for qualitative diagnosis.10,11
The differential diagnosis of neck masses is a routine clinical situation in ears, nose and throat clinics; and the causes can include infections, inflammatory conditions, congenital and neoplastic disease. Cases of germ cell tumours initially presenting as cervical masses are rare. 12 Among testicular cancer patients, the incidence of cervical lymph node metastasis is between 4.5% and 15%, of which only 5% of patients have a neck mass as the initial symptom. 12 This current case report describes a patient with a metastatic seminoma that presented as a solitary neck mass and the use of CEUS in the diagnosis.
Case report
In November 2021, a previously healthy 35-year-old male presented to the Department of Head and Neck Surgery, Sichuan Cancer Hospital Institute, Sichuan Cancer Centre, School of Medicine, University of Electronic Science and Technology of China, Chengdu, Sichuan Province, China with a 3-month history of the incidental discovery of a mass in his right neck. He had an isolated, firm, soft lump in his right neck without fever, cough, tingling, itching and other symptoms. He had no symptoms of upper respiratory malignancy. The patient did not have any testicular symptoms and clinical examination did not reveal any suspicious signs of testicular cancer.
Contrast computed tomography (CT) imaging of the neck demonstrated a 50 × 29 mm soft tissue mass in the right upper neck surrounding the right internal jugular vein (Figure 1). The head and neck surgeon arranged a neck ultrasound and ultrasound-guided core needle biopsy. The neck ultrasound showed that the hypoechoic mass (approximately 68 × 18 ×50 mm) was on the deep surface of the right sternocleidomastoid muscle, the lateral side of the common carotid artery and internal jugular vein (Figure 2). It had a clear boundary and irregular shape, appeared as an aggregation of small multi-nodules and the boundary between the mass and the right internal jugular vein was unclear. The colour-coded Doppler ultrasound showed no obvious blood flow signal in the mass.

Transverse contrast-enhanced computed tomography (CT) scan image (a) and coronal contrast-enhanced CT scan image (b) of a 35-year-old male that presented with a 3-month history of the incidental discovery of a mass in his right neck shows that the right upper neck mass (yellow arrows). The colour version of this figure is available at: http://imr.sagepub.com.

Ultrasound images of a 35-year-old male that presented with a 3-month history of the incidental discovery of a mass in his right neck show a hypoechoic mass (yellow arrows) on the deep surface of the right sternocleidomastoid muscle (a and b). The colour version of this figure is available at: http://imr.sagepub.com.
The CEUS imaging of the right neck mass was performed using an Aplio i800 scanner (Canon Medical Systems [China], Beijing, China) equipped with an ultra-wideband linear i18LX5 transducer (Canon Medical Systems [China]). A single bolus injection of 2.4 ml of SonoVue® (Bracco SpA, Milan, Italy) was injected into the forearm vein followed by 5 ml of normal saline. The CEUS showed unhomogeneous hyperenhancement during the arterial phase and hypoenhancement in the venous phase (Figure 3). The pathological examination of the right neck mass showed evidence of a germ cell tumour, in particular a seminoma (Figure 4). Further immunohistochemical staining showed that the tumour cells were positive for Spalt Like Transcription Factor 4 (SALL4). The cells were negative for human chorionic gonadotropin (hCG), CD30, S100, alpha-fetoprotein (AFP), Epstein-Barr encoding region in situ hybridization and p63. The final diagnosis was metastatic seminoma.
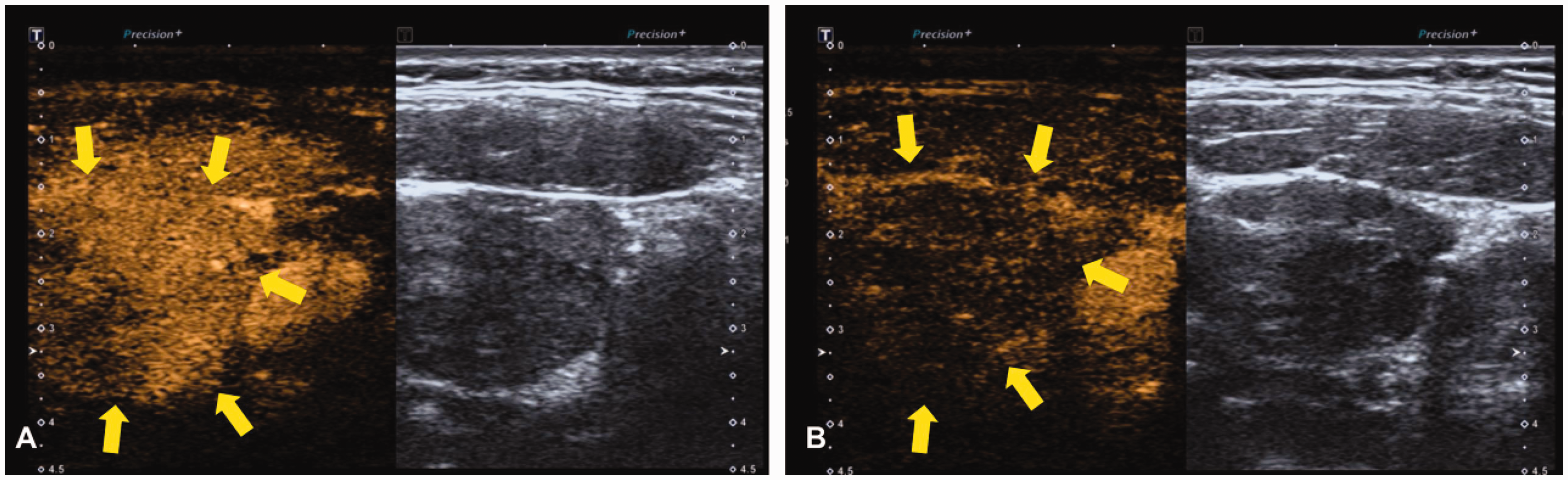
Contrast-enhanced ultrasound images of a 35-year-old male that presented with a 3-month history of the incidental discovery of a mass in his right neck show that the neck mass (yellow arrows) presented with unhomogeneous hyperenhancement during the arterial phase (A) and hypoenhancement during the venous phase (B). The colour version of this figure is available at: http://imr.sagepub.com.

Representative photomicrographs showing the histological features of a sample of the mass removed from a 35-year-old male that presented with a 3-month history of the incidental discovery of a mass in his right neck. The histological features confirmed the diagnosis of metastatic seminoma. The tumour cells were consistent in shape and arranged in a diffuse sheet shape. The tumour cells were large in volume, with transparent cell membranes, pale to bright cytoplasm, large and central nuclei, round or polygonal and massive chromatin (haematoxylin and eosin, scale bar 10 µm). The colour version of this figure is available at: http://imr.sagepub.com.
Positron emission tomography-CT imaging was performed and showed positive hypermetabolic activity in one right upper cervical lymph node, consistent with metastatic lymphadenopathy (Figure 5). No primary site of the malignant tumour was found. Laryngoscopy showed that the local mucosa of the nasopharynx was slightly elevated and biopsy showed chronic inflammation of the mucosa. Colonoscopy showed that the local mucosa of the transverse colon was rough and reddish. Biopsy pathology showed chronic inflammatory cell infiltration with papillary hyperplasia. Serum hCG (3.90 mIU/ml; reference range 0–2 mIU/ml) was raised and AFP (3.79 ng/ml; reference range 0–7.0 ng/ml) was within normal limits. Full blood count, renal function, liver function and other routine blood tests were normal. Testicular examination showed that both testicles had descended, but no mass was palpated. Ultrasound also showed no definite mass in either testis.
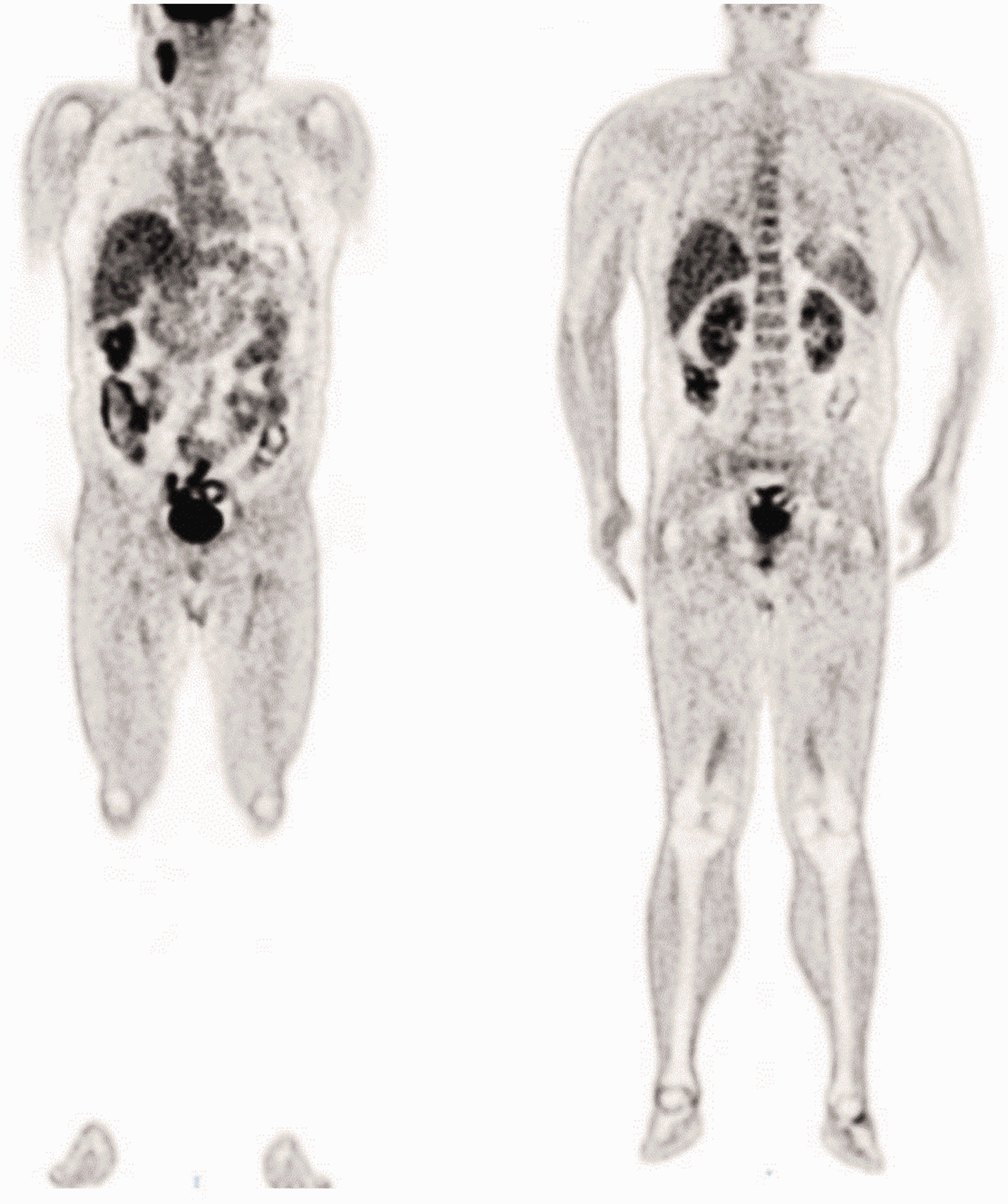
Positron emission tomography-computed tomography imaging of a 35-year-old male with a metastatic seminoma tumour in his right neck showed positive hypermetabolic activity in one right upper cervical lymph node but the primary site of the malignant tumour was not found.
Oncology consultation recommended a chemotherapy regimen, including four cycles of etoposide and cisplatin (100 mg etoposide, once daily, intravenously on days 1–5, 40 mg cisplatin, once daily, intravenously on days 1–3) and intensity-modulated radiotherapy. The size of the neck mass decreased significantly after receiving the treatment.
This study was approved by the Ethics Committee of Sichuan Cancer Hospital Institute, Sichuan Cancer Centre, School of Medicine, University of Electronic Science and Technology of China, Chengdu, Sichuan Province, China (no. SCCHEC-03-2019-030) for publication. Written informed consent was obtained from the patient for his treatment and publication of this report. The reporting of this study conforms to the CARE guidelines. 13
Discussion
Testicular tumours account for approximately 1% of male cancers and are the most common malignant tumours in men aged 29–30 years. 5 Primary testicular malignancies are usually classified as seminomas and non-seminomatous germ cell tumours. A patient having a personal history of testicular germ cell tumours is the most important risk factor for testicular cancer and will increase the risk of secondary testicular tumours by 12-times, which occurs in 2–3% of patients.14,15
Seminoma classically presents with a painless, palpable, solid mass in the testicle. A few patients present with epididymal-orchitis with testicular swelling and mild discomfort. 7 Approximately 75% of seminomas are confined to the testis; 16 and metastasis to nonregional lymph nodes or disseminated disease is much less frequent (14%).5,16 The current patient presented with a single neck mass instead of a testicular mass or testicular discomfort, which is rare. Seminoma metastases via the lymphatic route and presents a sequential pattern, involving the abdominal lymph nodes first, then the chest and neck lymph nodes. 17 A previous study demonstrated that 4% of patients with seminoma also had neck metastasis and only 5% of patients had a neck mass as the initial symptom of the disease. 18
Ultrasound examination of testicular seminomas show unilateral and homogeneous hypoechoic masses that are lobulated or multinodular. 19 Calcification and cystic degeneration are relatively rare, accounting for only 30% and 10%, respectively. 20 Compared with adjacent normal testis, seminoma demonstrates increased vascularity on Doppler ultrasound. 20 CEUS can show low-speed blood flow and sensitivity to microcirculation perfusion in tissues.21,22 A previous study showed that seminomas presented with heterogeneous enhancement, rapid wash-in and wash-out, and peripheral rim hyperenhancement signs. 23 The current patient presented with inhomogeneous hyperenhancement during the arterial phase and hypoenhancement during the venous phase, similar to the CEUS pattern for seminomas. Infarctions or epidermoid cysts are types of nonneoplastic lesions that lack blood vessels. Although it can occasionally be challenging to identify these two types of lesions from testicular cancers on ultrasound, CEUS can be valuable. Testicular lymphoma is the most commonly occurring testicular malignancy in older men. 24 Hypervascularity is typical of testicular lymphoma. 24 Nonbranching linear vessels, rapid wash-in and slow wash-out patterns of the particular vascular pattern of lymphomas distinguish them from other types of cancer. 24
In conclusion, case reports of seminomas presenting only as a neck mass are very rare, so they can easily go undiagnosed or be misdiagnosed, particularly in young men. Therefore, for a single neck mass, it is best to obtain sufficient clinical information and multimodal imaging findings, which are helpful to make a precise diagnosis.
Research Data
sj-jpg-1-imr-10.1177_03000605221135482 - Research Data for Contrast-enhanced ultrasound in the diagnosis of a solitary neck mass: a case report of metastatic seminoma
Research Data, sj-jpg-1-imr-10.1177_03000605221135482 for Contrast-enhanced ultrasound in the diagnosis of a solitary neck mass: a case report of metastatic seminoma by Ziyue Hu, Xiang Yan, Jiulong Dai, Yanjie Li and Man Lu in Journal of International Medical Research
Footnotes
Author contributions
Ziyue Hu and Man Lu contributed to the project and wrote the main body of the manuscript. Xiang Yan and Jiulong Dai designed the manuscript. Yanjie Li participated in the clinical study.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.