
Abstract
A schwannoma is a benign tumor that arises from the myelin-producing Schwann cells that surround nerves. We herein report a case involving a 55-year-old man who first presented to our clinic with a schwannoma of the posterior tibial nerve and 5 years later with a schwannoma of the ulnar nerve. This is the first report of schwannomatosis of the ulnar and posterior tibial nerves.
Introduction
A schwannoma is a benign tumor that arises from the myelin-producing Schwann cells that surround nerves. Approximately 45% of schwannomas are located in the head and neck region, 1 , 2 3% to 19% are located in the upper extremities, and only about 1% to 10% are found in the lower extremities. 3 , 4 Most commonly, a schwannoma occurs as a solitary idiopathic lesion. The presence of multiple lesions suggests a genetic disorder, such as neurofibromatosis (NF). This can present in three distinct forms: NF type 1 (NF1), NF type 2 (NF2), and schwannomatosis. 2 This is the first report of schwannomatosis of the ulnar and posterior tibial nerves.
Case report
A 55-year-old man presented to our clinic with pain along the left posterior tibial nerve. The pain had begun 2 years earlier and had progressively increased since then. He had no history of trauma. Tinel’s sign was positive along the left posterior tibial nerve. Palpation revealed no sign of a tumor. Soft tissue ultrasound revealed a tumor-like mass on the proximal third of the left posterior tibial nerve. The tumor was excised with the patient under general anesthesia, and full remission of the symptoms was achieved after surgery. Microsurgical loupes with 4× magnification were used. The tumor was completely removed without damaging any nerve fascicles. Macroscopically, the tumor had an “onion bulb-like” appearance and measured 2.0 × 1.3 × 1.0 cm (Figure 1). Microscopic examination revealed Antoni A and B areas, which are distinctive for schwannoma.
“Onion bulb-like” appearance of the tumor.
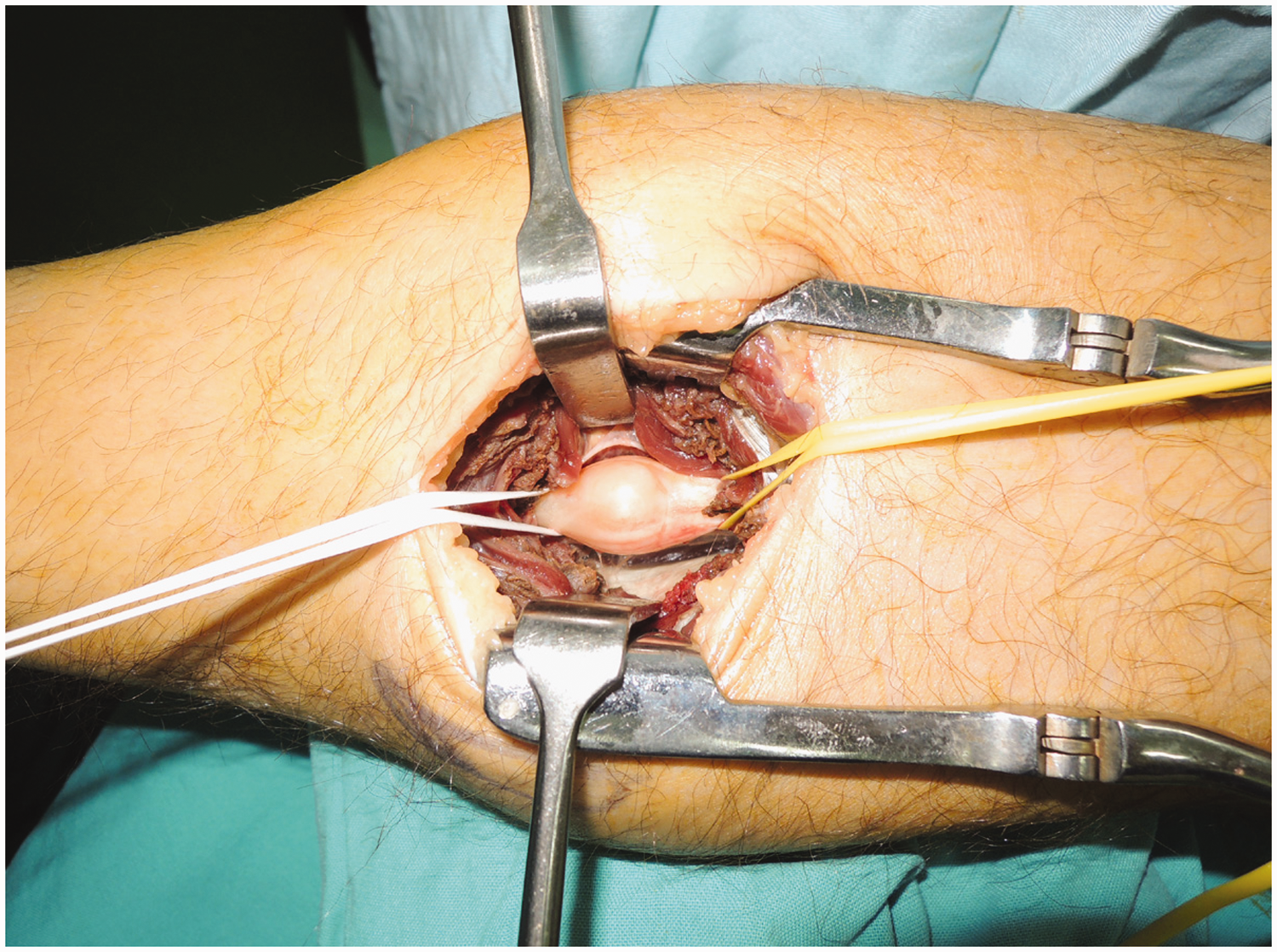
Five years later, the patient presented to our clinic again with pain in the right arm along the ulnar nerve. Palpation revealed a painful, firm, nodular tumor of approximately 2.1 cm located in the proximal one-third of the arm. Tinel’s sign was positive on the ulnar nerve trajectory. Ultrasound examination confirmed the presence of a hypoechogenic, round, well-delimited nerve tumor (Figure 2). After removing the tumor using the same technique described earlier, pathologic examination confirmed the diagnosis of a schwannoma of the ulnar nerve (Figure 3). The tumor measured 1.7 × 1.3 × 1.3 cm. A tumoral syndrome of schwannomatosis or NF2 was suspected. The patient had no family history of schwannomatosis or NF. These two entities were differentiated by ruling out the presence of a bilateral lesion on the acoustic nerve, which is a characteristic of NF2. Magnetic resonance imaging (MRI) was negative for an acoustic nerve tumor. Consequently, we established the final diagnosis of sporadic schwannomatosis. No complications occurred during the 6-month follow-up period after the second procedure.

Ultrasound appearance of the schwannoma.

Histopathologic appearance of the ulnar nerve tumor. Antoni A and B areas are distinctive for schwannoma.
Discussion
Schwannoma is the most common tumor of the nerve sheath and originates from Schwann cells. 5 This tumor can appear either as a unique lesion, which is considered to be an idiopathic schwannoma, or as multiple lesions, suggesting a genetic tumor predisposition syndrome. The most common genetic condition in such patients is NF2, the landmark feature of which is bilateral acoustic nerve schwannomas. 6 , 7
In 1997, Jacoby et al. 8 suggested the first diagnostic criteria for schwannomatosis, a different entity than NF2, based on several cases of multiple schwannomas without the landmark feature of NF2. Over the following years, the criteria were modified to exclude patients with NF2 characteristics, such as bilateral acoustic schwannomas on high-quality MRI, a first-degree relative with NF2, or a known constitutional NF2 mutation. 6 , 9
Later, several schwannomatosis-specific genetic mutations were identified. Thus, according to Plotkin et al. 10 and Ostrow et al., 11 the diagnosis of schwannomatosis can either be based on clinical criteria or the combination of clinical and molecular data. The clinical criteria are (i) the presence of at least two non-intradermal schwannomas and the absence of a vestibular nerve tumor based on MRI examination or (ii) confirmation of schwannomatosis in one first-degree family member and the presence of either a schwannoma, including a unilateral vestibular schwannoma, or an intracranial meningioma. The genes that predispose to schwannomatosis are SMARCB1 and LZTR1. 7 Germline mutations of these tumor suppressor genes are associated with one of the two types of schwannomatosis: sporadic or familial. 7 , 12 The NF2 gene mutation is frequently present in patients with schwannomatosis, but this abnormality appears as a somatic mutation that affects both alleles. Only 15% to 25% of cases present as a familial form, and the SMARCB1 abnormality is found in 40% to 50% of these cases. 7 , 13 De novo mutation of the LZTR1 gene is found in 30% of sporadic cases of schwannomatosis. A correlation exists between clinical and molecular abnormalities. Meningiomas have been reported only in patients with the SMARCB1 mutation, and rhabdoid tumors have been found in SMARCB1-familial forms of schwannomatosis with germline truncated variants. 12 The tumors are most frequently found on the peripheral nerves (89%), followed by localization along the spinal nerves (74%). 7 One in three patients presents with limited disease called segmental schwannomatosis, which means that the tumors are located on one limb, on one side of the body, or in one region of the spine. 12
In a large retrospective analysis of 87 patients with schwannomatosis, the most common locations were on the arm (46%) or the leg (47%). 9 Other patients with schwannomatosis described in the literature presented with multiple lesions on one nerve or on one limb. Lewis et al. 14 and Shank et al. 15 reported cases of schwannoma in which the tumors were located on the ulnar or median nerves. Ogose et al. 16 reported four cases of schwannomatosis in which multiple tumors were located on one limb.
Other soft tissue tumors of the extremities (e.g., lipomas, lymph node tumors, epidermoid cysts, neurofibromas, and malignant peripheral nerve tumors) must be included as differential diagnoses of schwannoma. The differentiation between schwannomatosis and NF1/NF2 is based on clinical and histological features. NF1 is characterized by the presence of a neurofibroma, a histologically distinct tumor with a high risk of malignant degeneration, as well as clinical presentation of “café au lait” cutaneous spots. Patients with NF2 develop multiple peripheral nerve tumors (e.g., schwannoma or meningioma) at a young age in association with other features that help to distinguish NF2 from schwannomatosis (e.g., bilateral vestibular schwannomas, ependymomas, cutaneous schwannoma, or cataract).12,13
A neurofibroma has the potential to undergo malignant degeneration. This risk is lower for a schwannoma because of the genetic mutations that involve tumor suppressor genes. However, this risk remains uncertain, and specific factors such as rapid growth or refractory pain can suggest malignancy.12,17
The management of a schwannoma depends on the severity of the clinical manifestations. Surgery is the only totally curative treatment. Surgical intervention follows a simple principle: enucleation of the tumor without damage to the nerve. For infiltrating tumors, partial excision only is possible. Because of its capsule, the tumor can be successfully and entirely removed with no nerve damage or with minimal nerve lesions. This contributes to a very low recurrence rate.2,12
Our case of schwannomatosis is unique in the English-language literature because the tumors were located in both the upper and lower extremities. In other cases of schwannomatosis reported in the literature, the patients’ lesions were limited to one limb (e.g., ulnar, median, or sciatic nerve) or one side of the body (e.g., right ulnar nerve or right superficial fibular nerve). 2 , 13 Another particularity of our case is the long-term follow-up necessary to establish the correct diagnosis. Unlike other reported cases of multiple schwannomas, our case required 5 years of follow-up to confirm the correct diagnosis.
In conclusion, a long-term follow-up, family history, and additional investigations were necessary to establish the diagnosis of schwannomatosis in this case. A microsurgical approach is necessary to prevent damage to nerve fascicles and to completely remove the tumor.
Footnotes
Ethics and consent
Ethics committee approval was not required for this case report. Patient consent was also not required because the patient’s identify has been protected.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.