
Abstract
Objective
Several recent studies have shown that the aldosterone synthase gene (CYP11B2) −344C/T polymorphism is related to cardiovascular diseases. However, whether the −344C allele influences the incidence of cardiovascular diseases in Chinese patients with hypertension is unclear.
Methods
Chinese patients with essential hypertension were genotyped for the −344C/T polymorphism in CYP11B2 (n = 755; CC, n = 112; CT, n = 361; TT, n = 282) and followed for 11 years for major adverse cardiovascular events (MACEs), including stroke, onset of coronary artery disease (CAD), and CAD-related death. Established cardiovascular risk factors were used to adjust the multivariate Cox analysis.
Results
After a mean follow-up period of 7.60 ± 1.12 years, a significantly higher incidence of MACEs was seen in patients with the CC genotype than in those with the CT and TT genotypes. The CC variant was significantly and independently predictive of MACEs (hazard ratio = 2.049), CAD (hazard ratio = 1.754), and stroke (hazard ratio = 2.588), but not CAD-related stroke or death.
Conclusion
The CYP11B2 −344 CC genotype is a risk factor for CAD and stroke, independent of other established cardiovascular risk factors in Chinese patients with hypertension.
Introduction
Essential hypertension (EH) is a complicated, chronic, noncommunicable disease that is a major risk factor for cardiovascular disease and mortality, including ischemic heart disease 1 and stroke. 2 Annually, approximately 9.4 million deaths are attributed to high blood pressure, which is one of three leading risk factors for global disease burden.3,4 Predicting the development of cardiovascular diseases in patients with hypertension is important.
The human aldosterone synthase (CYP11B2) gene is located at chromosome 8q22. 5 It encodes a key enzyme involved in the terminal steps of aldosterone biosynthesis. 6 One study from Egypt suggests that CYP11B2 genotypes and baseline serum K are predictors of spironolactone response in heart failure with reduced ejection fraction, which suggests that it may be correlated with cardiovascular disease. 7 In the 30 years since it was first sequenced, numerous common CYP11B2 polymorphisms have been identified. The most studied is the rs1799998 C/T single nucleotide polymorphism (SNP), also referred to as “−344” because of its base position relative to the gene transcription start site.8,9 At the molecular level, the role of the CYP11B2 locus has been extensively evaluated in cardiovascular disease, with particular attention to the −344C/T SNP. Previous studies also identified variants of CYP11B2 associated with increased risk of EH.10,11 We found that the −344C allele is strongly associated with increased left ventricular size and decreased baroreflex sensitivity in healthy individuals; these physiological parameters are cardiovascular risk factors.8,12 Nevertheless, one report suggested that rs1799998 is not associated with hypertension or other cardiovascular indicators in a population in Thailand. 13
Recent population-based studies established the association of the −344C/T CYP11B2 polymorphism with the risk of cardiovascular diseases.14,15 Because of differences in −344C/T allele frequencies and incidences of cardiovascular disorders in different ethnicities, these results may not be applicable to the Chinese population. Moreover, most of these studies were conducted in healthy populations and, at least in part, were unable to demonstrate a genetic association for patients with hypertension. Therefore, whether the allele at −344C/T influences the incidence of cardiovascular disease in patients with hypertension needs to be confirmed in hypertensive cohort-based studies. Here, we conducted a prospective study to investigate the association between the −344C/T SNP and the risk of cardiovascular diseases in a cohort of Chinese individuals with hypertension.
Methods
Ethical approval
The protocol was approved by the Institutional Ethics Committee of Hebei General Hospital and Beijing Xuanwu Hospital, China. Written informed consent was obtained from each study participant.
Study subjects
In this study, 820 outpatients diagnosed as having EH without cardiovascular disease were recruited sequentially between June 2004 and May 2006 at Hebei General Hospital and Beijing Xuanwu hospital. A clinical survey and genotyping were conducted for each patient. Sixty-five patients were excluded because of lack of follow-up. The remaining 755 patients were included (CC, n = 112; CT, n = 361; TT, n = 282; Table 1). Diagnosis of EH was based on the 8th report of the Joint National Committee. Exclusion criteria were present or past ischemia (patients underwent exercise electrocardiography, stress myocardial perfusion imaging, or coronary artery angiography, and showed no evidence of myocardial ischemia), congenital or valvular heart disease, dilated or hypertrophic cardiomyopathy, myocarditis, heart failure, stroke, and other cardiovascular or cerebrovascular diseases.
Study participant characteristics.

HDL, high-density lipoprotein; LDL, low-density lipoprotein; ACEI/ARB, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker.
Measurements of cardiovascular disease risk factors
At study entry, blood pressure was taken at two office visits at least 1 week apart by the same trained nurse using a standard mercury sphygmomanometer with the patient in the sitting position. The measurement was taken using the right arm with an appropriate cuff size and after the subject had rested for at least 5 minutes. Systolic and diastolic blood pressures were based on the first and fifth Korotkoff phases, respectively. Three measurements were made at 2-minute intervals and the mean was used in the analysis.
Body mass index (BMI, kg/m2) was calculated from standardized measurements of height and weight. Current smoking was defined as having smoked at least 100 cigarettes in the patient’s lifetime and currently smoking on all or some days during the past year. Diabetes was defined as fasting plasma glucose ≥7.0 mmol/L (126 mg/dL) or glycated hemoglobin (HbA1c) ≥6.5% according to the American Diabetes Association criteria or reported use of diabetic medications.
All blood biochemical markers were derived from the existing medical record or, where this was unavailable for the preceding 12 months, by measurement during the screening phase of the study. Disease status, personal history of cardiovascular diseases, and antihypertensive or other medication use were reported by the usual treating physician.
Genotyping
Venous blood was collected in 5-mL EDTA tubes. Genomic DNA was isolated with the QIAamp DNA Blood Mini Kit (Qiagen, Hamburg, Germany) and stored at −20°C. The CYP11B2 −344C/T polymorphism was determined by PCR-restriction fragment length polymorphism (RFLP). The primers used were 5′-CAGGGCTGAGAGTAAAA-3′ (forward) and 5′-CAGGGGGTACGTGGACATTT-3′ (reverse) as previously reported. 16 The PCR amplification was performed in a 20-µL reaction mixture (PCR master mix, TaKaRa Bio, Tokyo, Japan) with 2 µL of template DNA. The thermal cycling conditions included initial denaturation for 5 minutes at 95°C, followed by 35 cycles of denaturation at 94°C for 30 s, annealing at 53°C for 30 s, extension at 72°C for 30 s, and final extension for 10 minutes at 72°C. The amplicon was digested with HaeIII (2.5 units) overnight and subjected to 3% agarose gel electrophoresis. The digestion of the 153-bp PCR product resulted in the production of 97- and 56-bp bands in the presence of the C allele, whereas the product remained uncut in presence of the T allele. In addition to RFLP analysis, the selected PCR products were clone into pGEM-T Easy Vector Systems (Promega, Madison, WI, USA), and gene sequencing was performed to confirm the polymorphisms.
Clinical follow-up
Clinical follow-up was conducted by face-to-face interview in the consulting room, telephone contacts, or clinical visits (electronic medical record) every September. The questionnaire included events related to hypertensive complications and occurrence of death. We confirmed the responses by comparing them against patients’ medical records. The primary endpoint of this study was occurrence of major adverse cardiovascular events (MACEs), which included stroke (defined as rapidly developing signs of focal or global disturbance of cerebral function lasting >24 hours or leading to death, with no apparent cause other than that of vascular origin and diagnosis with computed tomography and/or magnetic resource imaging), the onset of coronary artery disease (CAD, including angina pectoris, myocardial infarction, and cardiovascular death). The follow-up duration was considered to encompass the interval from initial evaluation to the time of event onset or June 2018. The average follow-up period was 7.60 ± 1.12 years.
Statistical analyses
Categorical variables are reported as counts and percentages; continuous variables are presented as means ± standard deviations. Differences in proportions were statistically evaluated using the Chi-square test. Continuous variables were compared using ANOVA for parametrically distributed variables or Kruskal–Wallis statistics for nonparametrically distributed variables. The genotype and allelic frequencies of the C344T CYP11B2 were assessed by Hardy-Weinberg equilibrium (HWE) and compared by Chi-square test and Fisher’s exact test using the online calculator tool (http://www.oege.org/software/hardy-weinberg.html). Multivariable Cox proportional hazard regression was used to estimate adjusted hazard ratios (HRs) and the corresponding 95% confidence intervals with respect to CYP11B2 genotypes for the time to occurrence of the primary endpoint. We conducted a Cox proportional hazard model adjusted for age, male sex, family history of cardiovascular diseases, BMI, diabetes mellitus, dyslipidemia, and current smoking. 17 Kaplan–Meier curve estimation and log-rank tests were performed using SPSS software (version 17.0; SPSS Inc., Chicago, IL, USA). A p-value < 0.05 was considered significant.
Results
Baseline characteristics of participants
Baseline characteristics of the cohort in terms of CYP11B2 status are presented in Table 1. Among the 755 EH patients studied, 282 (37.4%) were homozygous for the T allele (TT genotype), 361 (47.8%) were heterozygous (CT genotype), and 112 (14.8%) were homozygous for the C allele (CC genotype). These frequencies were in agreement with those predicted by HWE (p = 0.435). No statistical differences in age or sex ratio were observed among the groups. No further significant associations with CYP11B2 genotypes could be detected.
Primary endpoint
As shown in Table 2, after a mean follow-up period of 7.60 ±1.12 years, 27 MACEs were observed in the CC genotype group, 32 in the TT genotype group, and 56 in the CT genotype group (26.2% vs.12.4% vs. 17.1%; p = 0.006). CAD occurred in 19 patients of the CC genotype group, 25 of the TT genotype group, and 46 of the CT group genotype group (18.4% vs. 9.7% vs. 14.1%; p = 0.064). Stroke was recorded in 10 patients in the CC genotype group, 9 in the TT genotype group, and 19 in the CT genotype group (9.7% vs. 3.5% vs. 5.8%; p = 0.061). Two patients of the CC genotype group, one patient of the TT genotype group, and nine patients of the CT genotype group had both CAD and stroke. Three patients of the CC genotype group, one patient of the TT genotype group, and three patients of the CT genotype group died (Table 2).
Major adverse clinical events over 11 years of follow-up according to CYP11B2 genotype.

MACEs, major adverse cardiovascular events; CAD, coronary artery disease.
As shown in Figure 1a and 1b, the time-to-event analysis using the Kaplan–Meier method showed a significantly higher rate of MACEs in the CC genotype group than in patients with the other genotypes (log rank p = 0.006 and p = 0.003 for differences among the three genotypes and between CC vs. TT+CT genotypes, respectively).

Kaplan–Meier curves for MACEs of subjects stratified according to genotype of the CYP11B2 gene −344C/T polymorphism (a), and according to the CC genotype or the CT+TT genotypes (b). Differences among and between the groups were assessed using log-rank tests. A p-value < 0.05 was considered significant. The cumulative (Cum) incidence of MACEs for the CC genotype was significantly higher than that for the other genotypes. MACEs, major adverse cardiovascular events.
Further investigation using a Cox proportional hazard model was done to study whether the CYP11B2 gene CC variant could predict the onset of cardiovascular diseases or mortality, independent of other risk factors. As shown in Table 3, CYP11B2 gene CC variant was significantly and independently predictive of MACEs (HR = 2.049; p = 0.001) and CAD (HR = 1.754; p = 0.032), but not stroke, CAD plus stroke, or death.
Cox proportional hazard models adjusted for traditional risk factors.
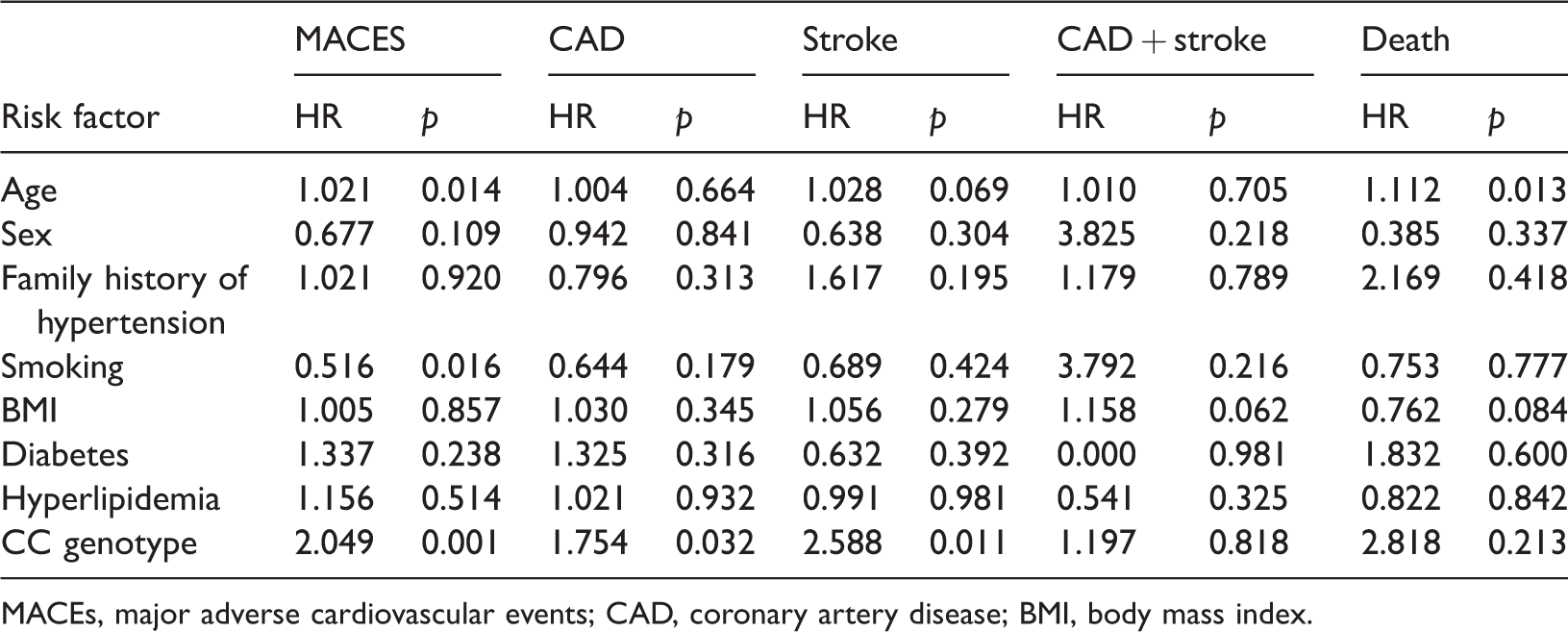
MACEs, major adverse cardiovascular events; CAD, coronary artery disease; BMI, body mass index.
Discussion
The present analysis is an 11-year longitudinal cohort study of Chinese EH individuals. The data demonstrated that the CC genotype of the −344C/T CYP11B2 polymorphism was associated with higher risk of incident cardiovascular diseases in patients with EH. This association was independent of other established cardiovascular diseases risk factors, such as age, male sex, family history of CAD and stroke, BMI, diabetes mellitus, dyslipidemia, and current smoking. Chi-square test revealed that new cases of MACEs were more frequent in the CC group than in the CT and TT groups. Kaplan–Meier curves also indicated that the CC group had an average shorter survival period.
In addition to regulating renal sodium resorption and intravascular volume, aldosterone may have direct effects on the cardiovascular system.18,19 A cytosine/thymidine (C/T) exchange at position −344 in the promoter of CYP11B2 affects binding of the SF-1 transcription factor,20,21 and thus might influence gene expression. This is currently the best explanation of the association between the −344C/T polymorphism in CYP11B2 and MACEs.
Many studies have shown a correlation between −344C/T and MACEs in different ethnicities. 22 The polymorphism was positively correlated with left ventricular mass and thickness in EH;23,24 left ventricular hypertrophy is an important predictor of cardiovascular morbidity and mortality in patients with hypertension. 25 In a meta-analysis, Yin et al. indicated that −344C/T polymorphism might be associated with CAD in Caucasian and Asian populations. 8 However, Mishra et al. 26 indicated that the −344C/T polymorphism in CYP11B2 is not correlated with CAD or left ventricular hypertrophy in an Indian population, although that study did not involve stratification by sex. In addition, a prospective study of healthy British men discovered that the −344C/T variant is not associated with cardiovascular risk. 27 Our current study included nearly 800 patients and showed that the −344C/T polymorphism in the CYP11B2 gene was associated with CAD in China.
Because of genetic and environmental differences in different populations, any results cannot simply be extrapolated to a Chinese patient with hypertension. This study based on Chinese patients with EH adds to the current knowledge and reveals an association of this polymorphism with the incidence of MACEs. This polymorphism potentially influences gene expression and aldosterone levels. 5 In an in vitro study, the −344C/T polymorphism in the CYP11B2 promoters was shown to affect binding of the SF-1 transcription factor and thus might influence gene expression; binding was 4 times stronger with the C allele than with the T allele. 21 Two studies22,23 indicated that increased aldosterone production was associated with the C allele. Our results also demonstrated that presence of the C allele increased the risk of MACE in this Chinese EH population. Indeed, compared with traditional risk factors, such as age, sex, family history of hypertension, smoking, BMI, diabetes, hyperlipidemia, only the CC genotype significantly increased the hazard risk for MACE. Other studies have reported that the CYP11B2 −344CC genotype was over-represented in patients with dilated cardiomyopathy or cardiovascular diseases with extreme elevations of aldosterone.28,29 In a study in a Tunisian Arab population, risk of CAD was associated with the −344C/T polymorphism, with interactions with age and smoking status. 30 Further studies are needed to clarify the nature and pathways of this association.
Stroke is a multifactorial and polygenic disease with major clinical manifestations and multiple etiologies. It is a significant cause of disability and death in developed countries.31,32 The association between the aldosterone synthase −344C/T gene polymorphism and ischemic stroke remains controversial and ambiguous. A meta-analysis of 7,710 subjects reported a lack of an association between the polymorphism and ischemic stroke.8,17 In 2015, another meta-analysis indicated that the −344C/T variant was significantly associated with ischemic stroke, and subgroup analysis showed that it was significantly associated with ischemic stroke in East Asian and South Asian populations, but not in a Caucasian population. 30 Presently, the CYP11B2 −344C/T polymorphism could influence susceptibility to ischemic stroke. Studies have demonstrated that the frequencies of alleles are different in different ethnic populations; consequently, ischemic stroke might be affected by genetic background. Furthermore, a report indicated that this polymorphism is associated with higher aldosterone synthase activity and increased aldosterone production, 33 which in turn induces sodium and water retention, increases systemic peripheral resistance, and can lead to adverse vascular remodeling, vasoconstriction, thrombosis, and vessel wall damage, ultimately increasing the odds of stroke development.34–36 Compared with traditional risk factors, such as sex, family history of hypertension, smoking, BMI, diabetes, hyperlipidemia, only the presence of the CC genotype had a significantly higher hazard risk.
Conclusions
In conclusion, we demonstrated that the CC variant at the −344C/T polymorphism in CYP11B2 was significantly and independently predictive of MACEs, CAD, and stroke in this Chinese population. The −344CC genotype is implicated as a risk factor for CAD and stroke independently of other established cardiovascular risk factors in Chinese patients with EH.
Footnotes
Author contributions
XQ defined the research theme. LW and ZZ designed methods and carried out the laboratory experiments. DL and KY analyzed the data, interpreted the results. LW and GZ collected the clinical data from Hebei General Hospital and Beijing Xuanwu Hospital, respectively. All authors contributed to, reviewed, and approved the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
Financial support from Key R&D Projects in Hebei Province (19277743D) is greatly appreciated.