
Abstract
Objective
To investigate the associations between β1-adrenergic receptor (ADRB1) and cytochrome P450 2D6 (CYP2D6) gene polymorphisms and β-blocker treatment outcomes in patients with hypertension.
Methods
Chinese patients with essential hypertension were treated with the β-blocker metoprolol and followed up for 12 weeks. xTAG® liquid-chip technology was used for CYP2D6 100 C > T and ADRB1 1165G > C genotyping. Associations between gene polymorphisms and antihypertensive therapy outcomes were assessed by generalized linear model fitting. A decrease of ≥ 10 mmHg in systolic blood pressure indicated an effective treatment outcome.
Results
A total of 93 patients were included in the study. Mutant allele frequencies of 61.29% and 58.60% were obtained for ADRB1 and CYP2D6, respectively. There was no significant interaction between the effects of ADRB1 and CYP2D6 gene polymorphisms on treatment outcome. Patients homozygous for the mutant ADRB1 genotype (CC) had better treatment outcomes than those heterozygous for the mutation (GC). Interestingly, β-blocker treatment duration was an independent factor associated with treatment outcome.
Conclusions
The ADRB1 1165G > C gene polymorphism and β-blocker treatment duration are independent factors associated with β-blocker treatment outcome. These findings suggest that the selection of antihypertensive therapy should take into consideration the patient’s genotype.
Introduction
Essential hypertension is a multifactorial disorder, with interactions between many genetic and environmental risk factors underlying its pathogenesis.1,2 It is a major public health problem throughout the world; 3 in China, there are around 200 million patients with hypertension, giving a prevalence of ∼20% in adults.4,5 Many candidate genes have been recognized as potential contributors to the pathogenesis of hypertension. 6 Polymorphisms of the β1-adrenoceptor 7 and of cytochrome P450 2D6 (CYP2D6) 8 have been reported to be involved in the pathogenesis of high blood pressure and related cardiovascular events.
The β1-adrenoceptor is encoded by the ADRB1 gene, which has two single nucleotide polymorphisms: Ser49Gly and Arg389Gly. The Gly49 allele of the Ser49Gly polymorphism is associated with greater agonist-promoted downregulation and altered glycosylation of the receptor, 9 while the Arg389 variant has been reported to have basal and isoprenaline-activated adenylyl cyclase activity that is three- to four-fold higher than the Gly389 variant. 10 These factors may explain the observed cardiovascular differences and varying responses to β-blockers between those with different ADRB1 genotypes. For example, Chinese men homozygous for the Arg389 variant have been reported to show heightened responses to metoprolol, in terms of resting heart rate as well as resting and exercise blood pressure. 11 Furthermore, in patients with essential hypertension, both the Ser49Gly and Arg389Gly polymorphisms have been found to be associated with the response to metoprolol treatment: patients with Ser49Arg389/Ser49Arg389 were the best responders, while little or no response was observed in patients with Gly49Arg389/Ser49Gly389.12,13 However, there is an ongoing debate concerning the importance of this effect, with one study reporting no major effect of these polymorphisms on the response to atenolol treatment. 14
The enzyme CYP2D6 accounts for only a small percentage (<2%) of all hepatic cytochromes, but is responsible for the metabolism of ∼25% of all drugs in current clinical use.15–17 Several studies have examined the effects of CYP2D6 phenotype in relation to the cardiovascular system. 18 Polymorphisms of the CYP2D6 gene are associated with a wide variety in CYP2D6 enzyme activity, ranging from complete deficiency to ultrafast metabolism. 19 1′-Hydroxylation of the β-blocker bufuralol by CYP2D6 was markedly decreased with the CYP2D6 variant Ser34 compared with the Pro34 variant, indicating that CYP2D6 Pro34Ser polymorphism is significantly associated with CYP2D6 enzyme activity. 20 Although several studies have identified an influence of CYP2D6 polymorphisms on metoprolol metabolism rate,16,21 inconsistent data have been reported with regard to response to metoprolol therapy, 22 with some studies reporting an association 23 and others showing little or no effect. 24
Although there is some evidence that ADRB1 and CYP2D6 gene polymorphisms influence the response to antihypertensive therapy with β-blockers, there is ongoing debate concerning the clinical importance of these effects. Furthermore, it is not known whether an interaction exists between the effects resulting from polymorphisms of these two genes. The aim of the present study was to investigate the association between the ADRB1 1165G > C (Arg389Gly) and the CYP2D6 100 C > T (Pro34Ser) polymorphisms, and outcomes in patients with hypertension treated with the β-blocker metoprolol.
Patients and methods
Patients
Chinese patients attending the Department of Cardiovascular Medicine, First Affiliated Hospital of Fujian Medical University, Longyan, China, aged 40–65 years, with grade I–II essential hypertension (systolic blood pressure 140–179 mmHg and/or diastolic blood pressure 90–109 mmHg), diagnosed according to the 1999 World Health Organization/International Society of Hypertension guidelines, 25 with no previous exposure to β-blockers, were recruited to the study between June 2012 and December 2012. Exclusion criteria included severe cardiac, liver or renal disease, patient withdrawal from the study or incomplete clinical data.
Written informed consent was obtained from all patients. The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Fujian Medical University, Longyan, China.
Fasting blood samples were collected at ∼06.00 h from all patients on admission to the study for the measurement of fasting blood glucose, triglyceride and uric acid. Blood glucose samples were collected using potassium oxalate as an anticoagulant. All samples were sent for immediate analysis.
All patients received 25 mg metoprolol twice a day or 40.5 mg sustained release metoprolol tartrate once a day. No other antihypertensive therapy was given. Blood pressure was measured every 4 weeks, and patients were followed up for 12 weeks. A decrease of ≥10 mmHg in the systolic blood pressure was considered to indicate an effective treatment outcome.
Genotyping and xTAG liquid-chip technology
Before commencing antihypertensive treatment, a 2 ml peripheral blood sample, anticoagulated with 15 mg/ml ethylenediamine tetra-acetic acid, was collected from each patient for genotyping. Samples were shaken gently approximately eight times to ensure the anticoagulant was well mixed, then stored at –20℃ until analysis. A DNA extraction kit (SurExam Biotech, Guangzhou, China) was used, according to the manufacturer’s instructions, to separate genomic DNA. Genotyping for ADRB1 1165G > C and CYP2D6 100 C > T was performed using xTAG® liquid-chip technology (Luminex, Austin, TX, USA). The xTAG protocol begins with a multiplex polymerase chain reaction (PCR), which is used to amplify regions of the target genes containing the mutation site. The resulting PCR products are treated with exonuclease I and shrimp alkaline phosphatase to remove excess nucleotides and primers, and cleaned using Exo-SAP® (Affymetrix, Santa Clara, CA, USA). They are then subjected to an allele-specific primer extension (ASPE) step using specific primer sequences complementary to the given genes of interest that are tagged with an xTAG universal tag sequence. These primer sequences were 5′-CCGCAAGGCCTTCCAGG-3′ for the wild type and 5′-CGCAAGGCCTTCCAGC-3′ for the mutation for the ADRB1 1165G > C polymorphism, and 5′-GGGCTGCACGCTACC-3′ for the wild type and 5′-GGGCTGCACGCTACT-3′ for the mutation for the CYP2D6 100 C > T) polymorphism. The ASPE products were then hybridized to specific antitag probes precoated onto polystyrene microspheres, and streptavidin phycoerythrin was added for fluorescent detection using a Luminex 200 Analyzer (Luminex).
Statistical analyses
Data were reported as mean ± SD. Associations between the gene polymorphisms ADRB1 1165G > C and CYP2D6 100 C > T and treatment outcomes of β-blocker antihypertensive therapy were assessed using two-factor repeated measures analysis of variance
(ANOVA). Comparisons between ADRB1 1165G > C and CYP2D6 100 C > T were assessed by ANOVA using the following generalized linear model:

A P-value <0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS® software, version 13 (SPSS Inc., Chicago, IL, USA).
Results
Patients
Baseline characteristics of 93 patients with grade I–II essential hypertension.
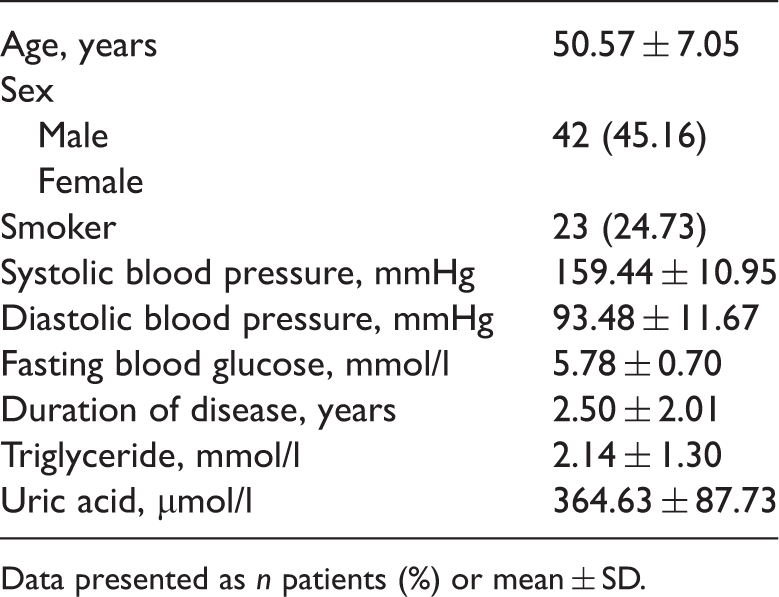
Data presented as n patients (%) or mean ± SD.
Demographic and clinical characteristics of 93 patients with grade I–II essential hypertension according to age group.

Data presented as n patients.
Genotyping
Genotyping of ADRB1 1165G > C and CYP2D6 100 C > T polymorphisms in 93 patients with essential hypertension.

Data presented as n patients or alleles (%).
ADRB1 1165G > C and CYP2D6 100 C > T polymorphisms according to sex, smoker status and age in 93 patients with essential hypertension.
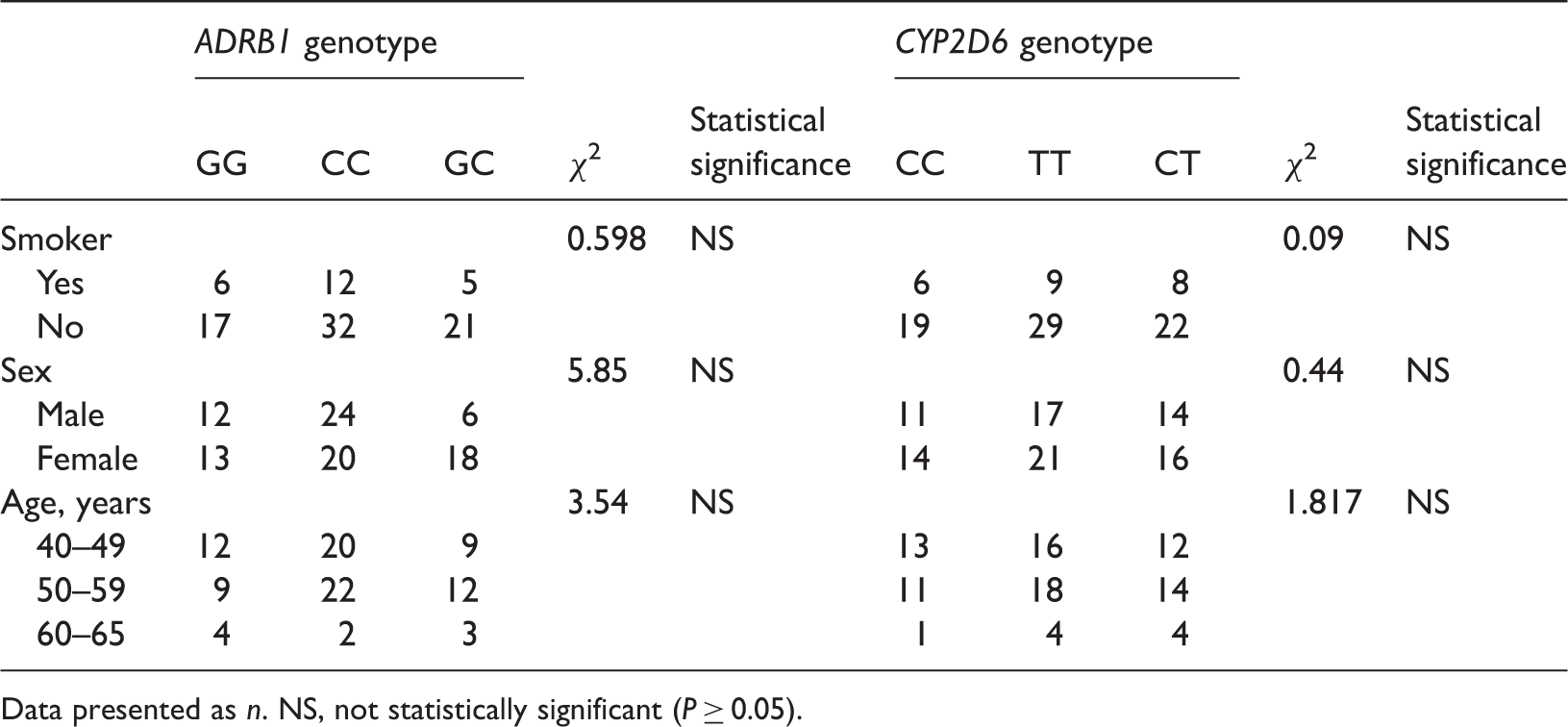
Data presented as n. NS, not statistically significant (P ≥ 0.05).
Correlations between polymorphisms and treatment outcomes
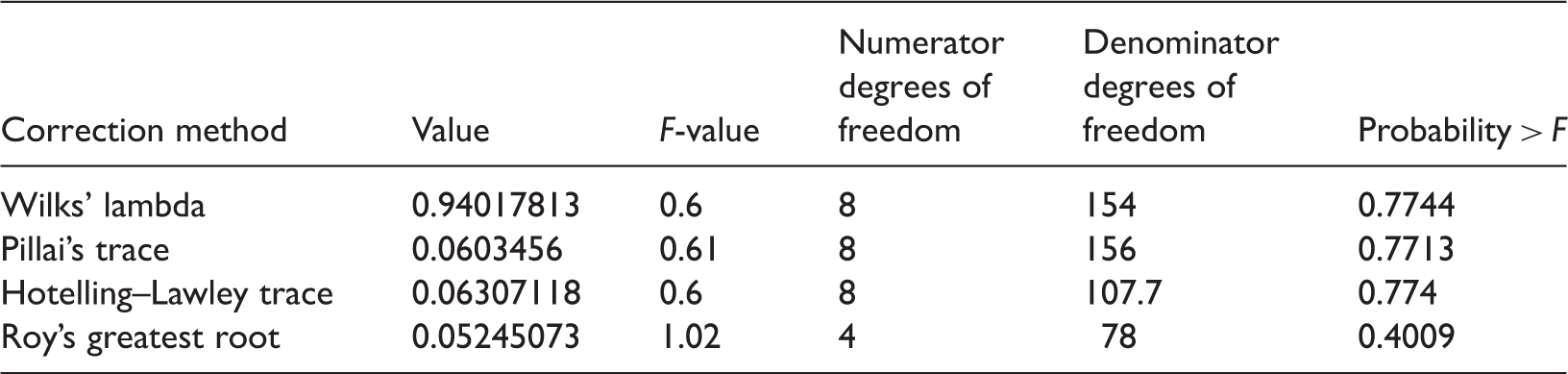
There was no significant interaction between the effects of the ADRB1 and CYP2D6 genes on treatment outcome (Table 5). When the effects of ADRB1 1165G > C and CYP2D6 100 C > T polymorphisms on the outcome of antihypertensive therapy with β-blockers for 12 weeks were analysed, ADRB1 polymorphism was shown to have a significant effect on therapeutic outcome (P < 0.05) (Table 6). Results of our analyses investigating the effects of CYP2D6 polymorphism on the outcome of antihypertensive therapy in this Chinese cohort were not statistically significant (data not shown). Tukey’s posthoc analysis indicated that patients homozygous for the mutant ADRB1 genotype (CC) had better treatment outcomes (systolic value after treatment) than those heterozygous for the mutation (GC) (P < 0.05) (Figure 1). Using multivariate ANOVA, four correction methods indicated that duration of treatment with the β-blocker was an independent factor associated with treatment outcome (P < 0.05) (Table 7); however, there was no correlation between ADRB1 polymorphisms and the duration of β-blocker treatment (P > 0.05) (Table 8).
Association between ADRB1 1165G > C polymorphisms and systolic blood pressure in patients with essential hypertension, treated for 12 weeks with β-blockers. MM, homozygous mutation; WM, heterozygous mutation; WW, wild-type. Analysis of the interaction between the effects of ADRB1 and CYP2D6 gene polymorphisms on the outcome of antihypertensive therapy with β-blockers assessed by analysis of variance using a generalized linear model. Analysis of the effects on the outcome of antihypertensive therapy with β-blockers of ADRB1 gene polymorphisms using two-factor repeated measures analysis of variance. Correlation between duration of β-blocker treatment and treatment outcome using four correction methods with multivariate analysis of variance Correlation between ADRB1 polymorphisms and duration of β-blocker treatment using four correction methods with multivariate analysis of variance



Discussion
The present study demonstrated that, in Chinese patients with essential hypertension, ADRB1 polymorphisms exert a much more important effect on the outcome of therapy with β-blockers than CYP2D6 polymorphisms, with superior efficacy found in patients homozygous for the ADRB1 1165G > C mutant genotype. Frequencies of 61.29% and 58.60%, respectively, were obtained for the ADRB1 and CYP2D6 mutant alleles. There was no significant interaction between the effects of ADRB1 and CYP2D6 gene polymorphisms on treatment outcomes.
Furthermore, the duration of β-blocker treatment was shown to be an independent factor associated with treatment outcome for antihypertensive therapy with β-blockers. Tailoring therapy to a patient’s genotype could potentially improve the efficacy of antihypertensive treatment.
The pathogenesis of essential hypertension is influenced by the interaction of many environmental and genetic factors.1,2 Several gene variants have been evaluated as candidate determinants for hypertension. The CYP2D6 gene is highly polymorphic, with ∼80 distinct alleles and allele variants. CYP2D6 polymorphisms have been demonstrated to affect the enzymatic activity of the expressed protein,26,27 which has been shown to have a major impact on the pharmacokinetics of the β-blocker metoprolol.8,28 This has led to questions about the effects of these kinetic differences on drug adverse effects and efficacy.21,29 In the present study, the CYP2D6 100 C > T polymorphism had a starkly reduced effect on β-blocker efficacy compared with the ADRB1 1165G > C polymorphism, which is are generally in agreement with previous studies. 26 Although CYP2D6 polymorphisms have been demonstrated to affect the metabolic rate of metoprolol in some studies,16,21 inconsistent findings have been reported with regard to the influence of these polymorphisms on the response to metoprolol therapy. 22 Notably, some investigators have reported an association between the response to metoprolol and the CYP2D6*4 allele, 23 while others have observed little or no effect on antihypertensive response rates, blood pressure changes or adverse event rates associated with several polymorphisms, despite clear differences between the variants in enzymatic activity. 24 Hence, it is likely that CYP2D6 polymorphisms have no major clinical impact on the response to therapy with β-blockers.
The β-blockers play a major role in the treatment of essential hypertension, and are widely used for the management of cardiovascular diseases. The efficacy of β-blockers is mainly attributed to their actions at the β1-adrenoceptor, which plays an important role in regulating the activity of the sympathetic nervous system. 30 However, the response to β-blockers varies between individuals, and this may be due in part to ADRB1 gene polymorphisms. Multiple studies have demonstrated the influence of ADRB1 polymorphisms on the response to treatment with β-blockers. For example, the expression level of myocardial ADRB1 was shown to affect the antihypertensive effects of metoprolol. 31 In addition, a clear association between ADRB1 polymorphisms and antihypertensive response to β-blockers such as metoprolol and carvedilol has been demonstrated.32,33 Importantly, a frequent ADRB1 polymorphism affecting the heart-rate response to carvedilol has been identified. 34 The present study demonstrated that the ADRB1 mutation had a significant clinical effect on β-blocker therapy. This is consistent with reports that mutations in the ADRB1 gene cause decreased β1-adrenoceptor sensitivity,26,27 and is in good agreement with other findings in both healthy individuals and essential hypertension patients. In healthy men, homozygosity for the Arg389 allele appeared to confer an enhanced response to metoprolol in terms of heart rate and blood pressure.11,35
Furthermore, in essential hypertension patients, Ser49Gly and Arg389Gly polymorphisms were associated with the response to metoprolol therapy, with Ser49Arg389/Ser49Arg389 and Gly49Arg389/Ser49Gly389 being found in the best and worst responders, respectively.12,13 Other studies have revealed an association between Gly389 and lower systolic and/or diastolic blood pressures, as well as reduced risk of essential hypertension.35–37 The Ser49Gly polymorphism has also been shown to be associated with heart rate, 7 diastolic blood pressure 38 and the systolic blood pressure response to antihypertensive medication. 39 Interestingly, pharmacokinetic studies have shown an impact of ADRB1 polymorphisms on carvedilol pharmacokinetics. 30 In particular, real-time optical recording has demonstrated differences in the response to carvedilol between the two codon-389 alleles in ADRB1 Arg389Gly polymorphisms. 40
A few limitations of the present study need to be considered. First, this was a preliminary prospective study with loose patient inclusion and exclusion criteria, susceptible to the limitations and biases inherent in such a design. Second, the sample size was small, meaning that the data may not properly define the gene–drug interactions. Furthermore, the follow-up time was very short. Therefore, a large-scale, prospective, controlled study is needed to confirm the importance of ADRB1 and CYP2D6 gene polymorphisms on the antihypertensive effect of β-blockers.
In conclusion, the identification of appropriate genetic markers may be of great benefit for the management of hypertension and related chronic diseases in future, allowing the tailoring of personalized therapies for patients with hypertension. Data from the present study demonstrated that the ADRB1 1165G > C homozygous mutant genotype is associated with increased β-blocker efficacy in hypertension, suggesting that the selection of antihypertensive therapy should take into consideration the patient’s genotype.
Footnotes
Acknowledgements
The authors sincerely thank all the investigators and co-ordinators who contributed to this study.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the Longyan Science and Technology Plan Projects (2013LY56).