
Abstract
Objective
The study aimed to evaluate the predictive value of the Short Physical Performance Battery (SPPB) and its three components for identifying the requirement for a prolonged hospitalization for coronary artery bypass grafting (CABG) in older patients.
Methods
This prospective, observational study included 425 older patients who consecutively underwent selective CABG surgery. All patients were assessed for the SPPB. We analysed the association of the postoperative length of hospital stay with the SPPB and three components. Receiver operating characteristic curve analysis was performed to determine the validity of the SPPB for predicting older patients with a prolonged hospitalization (>8 days).
Results
The SPPB and its three individual components were independent risk factors for a prolonged postoperative length of hospital stay. Only the SPPB summary score and the 4-m gait speed components showed good discriminative capabilities. An SPPB score cut-off of 9.5 provided the best accuracy for identifying a prolonged hospitalization. A poor physical performance (SPPB <10 score) was related to an increased risk of adverse cardiac and cerebrovascular events within 6 months after discharge.
Conclusions
This study provides evidence for clinical utility of the SPPB score for identifying older patients undergoing CABG who are at risk of prolonged hospitalization.
Keywords
Introduction
Coronary artery bypass grafting (CABG) is the standard surgical treatment for coronary artery disease and is performed regularly. Despite improvements in medical care, patients undergoing CABG tend to be older and have more comorbidities, which may be associated with postoperative complications and a prolonged length of hospital stay (LOHS). 1 Preoperative risk evaluation has played a crucial role in this occurrence. However, current risk prediction models, including the European System for Cardiac Operative Risk Evaluation, do not include objective measures for physical frailty.2,3 For older patients, physical frailty is being increasingly recognized as an indicator of a poor health status and vulnerability. 4 Many studies have examined the effect of frailty on outcomes of hospitalizations for several surgeries and found it to negatively affect index outcomes.2,5–8 However, there is variability in the available measures of frailty. Additionally, the amount of time and resources required for all frailty measurements limits the integration of these measurements into clinical practice. 9 Therefore, an effective measurement method is urgently required.
The Short Physical Performance Battery (SPPB) is one of the best physical performance tests for identifying frail adults10,11 and one of the most widely used instruments for measuring physical performance in population studies on ageing. 11 The SPPB has good concurrent validity compared with other measures of frailty, internal consistency, and satisfactory short- and long-term reliability. 12 The SPPB has also been widely used in the past few years because it is standardized and objective, rapid and simple to conduct, and fairly resistant to individual differences in cultural and educational backgrounds.
To date, several studies have reported the usefulness of the SPPB as a predictor of poor clinical outcomes in patients undergoing percutaneous intervention 13 and cardiac surgery.14–16 Nevertheless, the predictive value of the SPPB in older adult patients undergoing CABG is unknown. Therefore, this study aimed to determine the clinical value of the SPPB summary score in evaluating a prolonged postoperative LOHS in patients who undergo CABG. The secondary aim was to assess whether any component of the SPPB is equivalent to the full test battery in terms of clinical value and for evaluating the postoperative LOHS.
Methods
The reporting of this study conforms to the STROBE guidelines. 17
Participants
This prospective, observational study was conducted in our institution between October 2018 and September 2019. Patients (≥60 years) who underwent CABG during this period were screened. The same surgical team in Tianjin, China performed surgeries in the study population. The exclusion criteria were a history of serious cerebrovascular accidents and New York Heart Association functional class IV. The performance-based measures of physical function and interviews were assessed at hospital admission (within 48 hours after hospital admission, 2 hours after a meal in the morning). During 1 year, a consecutive sample of eligible patients was identified from health examinations of the patients. Patients who died in the operating room or surgical ward before discharge were excluded. For patients who underwent more than one CABG surgery, the final selection included only the most recent procedure. After surgery, patients who stayed in the hospital >8 days were classified as having a prolonged LOHS. 18 The average number of hospitalization days was 7.7 days. The study protocol was approved by the TEDA International Cardiovascular Hospital Institutional Review Board (reference no. 2018-0626-4, 24 August 2018) in Tianjin, China and was conducted in accordance with the Declaration of Helsinki. Informed written consent was obtained directly from the participants. Our research is registered at the Chinese Clinical Trial website (registry number: ChiCTR1800018465).
SPPB
This study used methodology from a previously published study and the SPPB was composed of three timed tests. 19 These tests were the standing balance test, the 4-m gait speed (4MGS) test, and the five-repetition sit-to-stand (5STS) test. The standing balance test required participants to maintain the following positions for 10 s each: standing with the feet in the side-by-side position, semi-tandem position, and tandem position. The 4MGS measured the time required to walk 4 m at the usual pace. This test was repeated twice, and the analysis used the shorter time of the two measurements. The 5STS required participants to stand up and sit down five times as quickly as possible with their hands folded across their chest. Each of the three performance assessments was assigned categorical scores (range: 0–4), and the sum ranged from 0 to 12.
Covariates
Data were prospectively collected during the patients’ admission by interviews and physical examinations. The collected data were as follows: age, sex, body mass index, waist to hip ratio, educational level, occupation, current diagnoses, left ventricular ejection fraction, New York Heart Association classification, a history of smoking and drinking, daily physical activity, psychological conditions, and a history of hypertension, hyperlipidaemia and diabetes. Information on smoking and drinking was obtained from a questionnaire survey. Physical activity was assessed with the short form of the International Physical Activity Questionnaire in Chinese. 20 Psychological conditions were assessed with the Generalized Anxiety Disorder scale 21 and the Patient Health Questionnaire. 22 Surgical data obtained from medical records comprised the operation type, duration of surgery, bypass time, length of stay in the intensive care unit (ICU), and duration of an indwelling drainage tube. Postoperative complications were defined as the occurrence of any of the following events: atrial fibrillation, myocardial infarction, reintubation, renal failure, stroke, anaemia, haemorrhage, infection, and sternal problems. All patients were followed up 6 months after randomization. The primary clinical end point was a composite of major adverse cardiac and cerebrovascular events (i.e., death from any cause, stroke, myocardial infarction, or repeat revascularization) and was assessed by medical records, clinical visits, and phone contacts. The end point assessors were blinded to the preoperative SPPB results.
Statistical analysis
Demographic and clinical variables are presented as mean ± standard deviation, median (interquartile range), or percentage. Differences between these variables were examined by analysis of variance (continuous variables) or the chi-square test (categorical variables), and differences were defined as significant when P<0.05. We performed multiple logistic regression analyses to test the SPPB and its three components as independent predictors of postoperative LOHS in each model. The SPPB and its three components were treated as continuous variables. The odds ratio (OR) and 95% confidence interval (CI) were computed. Multiple logistic regression analyses of Model 1 were adjusted for sex, age, and body mass index. Model 2 was additionally adjusted for smoking, drinking, depression, anxiety, diabetes, hypertension, and hyperlipidaemia on the basis of Model 1. Model 3 was additionally adjusted for the number of bridge vessels, operation type, duration of the operation, bypass time, length of stay in the ICU, duration of an indwelling drainage tube, and postoperative complications on the basis of Model 2.
Receiver operating characteristic (ROC) analysis was performed to define the best cut-off score for discriminating a prolonged hospitalization based on the sensitivity and specificity values associated with the scores of the various SPPB component tests. We chose the value for which sensitivity + specificity −1 was maximized as the best cut-off point. We assessed the sensitivity of the SPPB summary score and its three components to discriminate patients with a prolonged hospitalization from those without a prolonged hospitalization. To verify that the SPPB summary score was the best predictor, the SPPB was treated as a categorical variable to observe the primary clinical end point after discharge. All analyses were performed with SPSS version 19 statistical software (IBM Corp., Armonk, NY, USA). P<0.05 was considered statistically significant.
Results
Population characteristics
A total of 425 patients were included in the study. The baseline characteristics, preoperative data, and outcome variables of the patients who had CABG according to the postoperative LOHS are shown in Table 1. Overall, 331/425 (77.8%) patients who underwent bypass surgery in ≤8 days were discharged from the hospital, and 94 (22.1%) patients spent >8 days in the hospital after CABG. Among all patients, the postoperative LOHS ranged from 2 to 28 days (mean, 7.7±3.8 days), with a median of 7 days. A higher percentage of patients with a prolonged LOHS (postoperative LOHS day >8 days) underwent CABG combined with other surgeries than those without a prolonged LOHS (P<0.05). Patients with a prolonged LOHS had a longer operation time, bypass time, length of stay in the ICU, and duration of an indwelling drainage tube (all P<0.001; Table 1). There were no significant differences in physical activity, anxiety, or depression between the two groups.
Characteristics of the study participants according to the postoperative hospital stay.

Data are mean ± standard deviation, median (interquartile range), number, or percentage.
BMI, body mass index; WHR, waist to hip ratio; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; IPAQ, international physical activity questionnaire; MET/wk, metabolic equivalent task minutes per week; SPPB, Short Physical Performance Battery; 4MGS, 4-m gait speed; 5STS, five-repetition sit-to-stand; CABG, coronary artery bypass grafting; ICU, intensive care unit.
SPPB and outcome
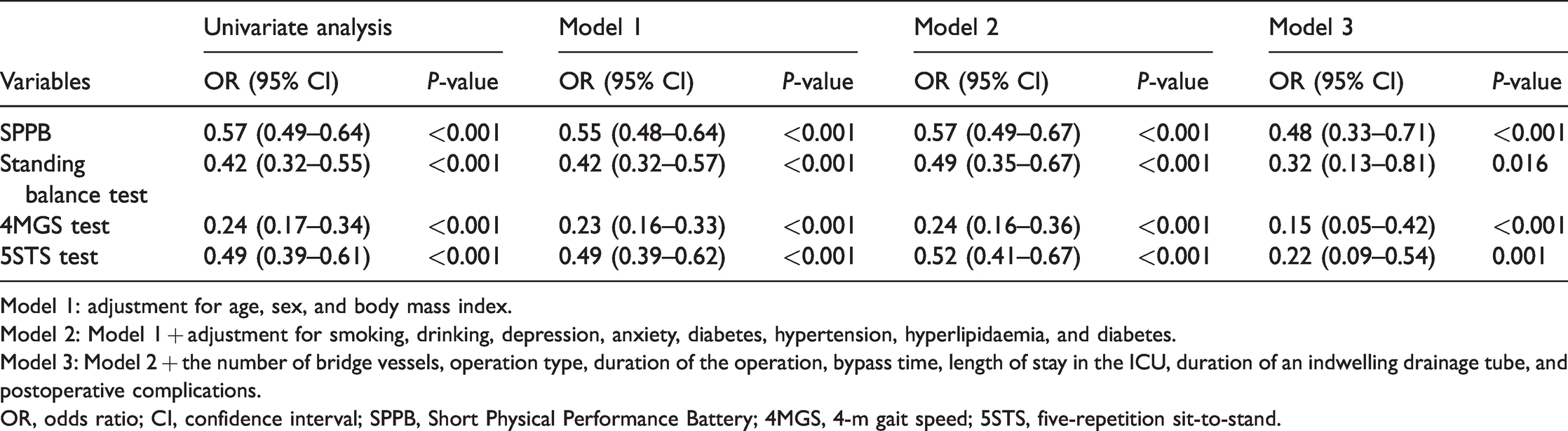
Patients with a prolonged postoperative LOHS had a significantly lower SPPB score than patients without a prolonged LOHS (P<0001) (Table 1). The results from univariate and multivariate logistic regression models for the SPPB related to the postoperative LOHS are shown in Table 2. After adjusting for potential confounders, the SPPB was an independent risk factor for a prolonged postoperative LOHS (Model 3; OR: 0.48, 95% CI: 0.33–0.71, P<0.001) (Table 2). For the SPPB summary score, a cut-off score of 9.5 (<10) provided the most accurate discrimination of a prolonged postoperative LOHS. Using this cut-off score, we calculated sensitivity and specificity values of 0.847 and 0.756, respectively (Table 3). Forty patients achieved the primary clinical end point. Detailed information of the primary end point according to the SPPB score is shown in Table 4. The crude and multivariable-adjusted ORs of a poor physical performance (SPPB score <10) for the primary clinical end point after discharge are shown in Table 5. The crude model showed that a poor physical performance was related to the primary clinical end point (OR: 2.41, 95% CI: 1.25–4.67, P=0.009). After adjusting for confounding factors, the OR for adverse cardiac and cerebrovascular events was 2.26 (95% CI: 1.02–4.99, P=0.044).
Multiple logistic regression analysis of the postoperative hospital stay and the SPPB.
Model 1: adjustment for age, sex, and body mass index.
Model 2: Model 1 + adjustment for smoking, drinking, depression, anxiety, diabetes, hypertension, hyperlipidaemia, and diabetes.
Model 3: Model 2 + the number of bridge vessels, operation type, duration of the operation, bypass time, length of stay in the ICU, duration of an indwelling drainage tube, and postoperative complications.
OR, odds ratio; CI, confidence interval; SPPB, Short Physical Performance Battery; 4MGS, 4-m gait speed; 5STS, five-repetition sit-to-stand.
AUC and cut-off point of the SPPB and individual components of the SPPB according to the receiver operating characteristic curve.

AUC, area under the curve; CI, confidence interval; SPPB, Short Physical Performance Battery; 4MGS, 4-m gait speed; 5STS, five-repetition sit-to-stand.
Primary clinical end point in patients divided by SPPB score cut-off points at 6 months of follow-up.
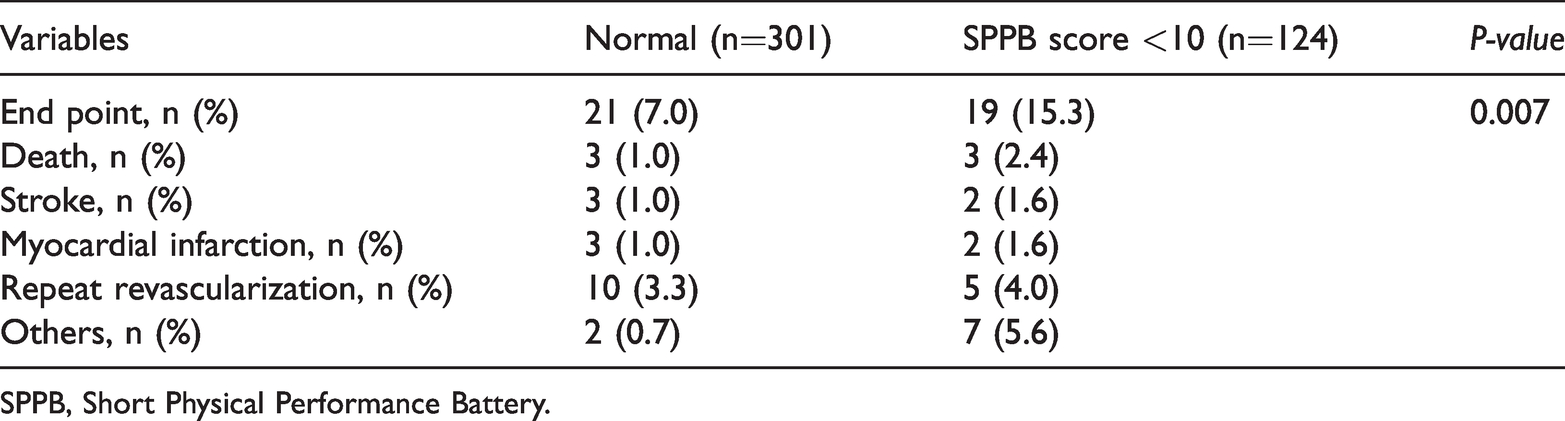
SPPB, Short Physical Performance Battery.
Crude and multivariable-adjusted ORs using the cut-off values of the SPPB score at 6 months of follow-up.
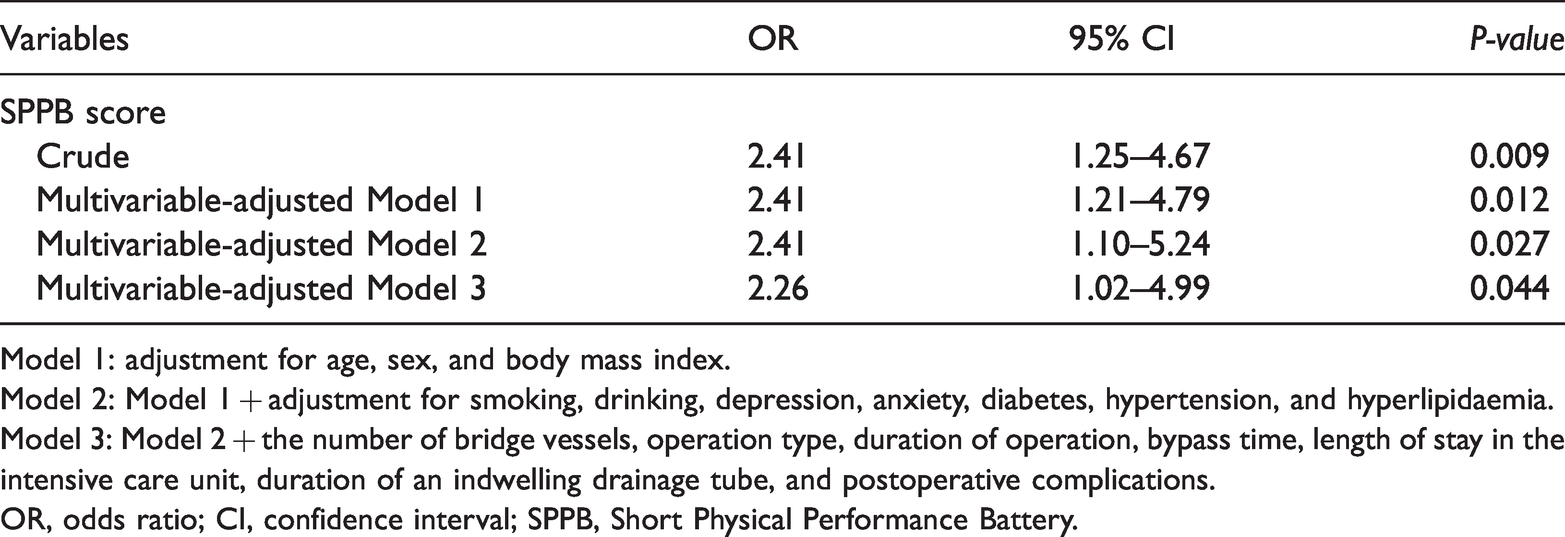
Model 1: adjustment for age, sex, and body mass index.
Model 2: Model 1 + adjustment for smoking, drinking, depression, anxiety, diabetes, hypertension, and hyperlipidaemia.
Model 3: Model 2 + the number of bridge vessels, operation type, duration of operation, bypass time, length of stay in the intensive care unit, duration of an indwelling drainage tube, and postoperative complications.
OR, odds ratio; CI, confidence interval; SPPB, Short Physical Performance Battery.
Three components of the SPPB and outcome
After adjusting for potential confounders, the individual components of the SPPB were independent risk factors for a prolonged postoperative LOHS (OR: 0.32, 95% CI: 0.13–0.81, P=0.016 for the standing balance test; OR: 0.15, 95% CI: 0.05–0.42, P<0.001 for the 4MGS test; and OR: 0.22, 95% CI: 0.09–0.54, P <0.001 for the 5STS test). Only the 4MGS test showed good discrimination (area under the curve: 0.771). The ROC curve plotted using sensitivity and specificity calculated from the SPPB and the three test components with the hospitalization stay after CABG is shown in Figure 1.

Receiver operating characteristic curve plotted using sensitivity and specificity calculated from the SPPB and its three components for predicting the hospitalization stay after coronary artery bypass grafting.
Discussion
Our findings provide evidence for the clinical value of the SPPB and 4MGS test in assessing a prolonged postoperative LOHS in patients who had CABG. Although the area under the curve values of the standing balance and 5STS tests were <0.7, these two components were also independent risk factors for postoperative hospitalization. To the best of our knowledge, this is the first study to assess the clinical value of each of the three SPPB components compared with that of the SPPB as a whole in evaluating patients with CABG.
SPPB scores predict LOHS
There is a large amount of evidence showing that different physical performance tests can be used to predict various adverse outcomes in older adults. 23 However, to date, physical performance measures in the cardiac surgery clinical setting have received little attention. The present study showed that the SPPB score at hospital admission had the highest discriminatory ability for a prolonged and typical postoperative LOHS. Our results confirm and extend the findings of previous studies at the clinical level. Moreover, our findings are consistent with those of a study conducted by Nastasi and colleagues who suggested that the SPPB is a valid indicator for functional and clinical status and that SPPB impairment was independently associated with a longer LOHS. 24 Measures of physical performance, including factors such as ageing, comorbidities, and disease severity, reflect the overall and multisystem health status of older individuals.25–27 Similar to other biomarkers, the SPPB might be a nonspecific, but highly sensitive, indicator for an individual’s overall health status because it reflects several underlying physiological impairments. 28 Some patients with low SPPB scores are more likely to be frail, vulnerable, and clinically unstable. Therefore, these patients have a higher risk of a prolonged postoperative LOHS. Additionally, poor SPPB scores indicate a higher risk of a prolonged postoperative LOHS owing to an increased need for cardiopulmonary bypass and a period of anoxia during CABG surgery. These findings may explain why the SPPB showed a better prognostic value than the other individual indicators in our study.
In this study, we found that an SPPB summary score with a cut-off of <10 showed the highest discriminatory ability for a prolonged postoperative LOHS. An SPPB score <10 is a known predictor of mortality in the general population, 29 which is consistent with our findings. Moreover, this cut-off value is also used to identify older persons with chronic obstructive pulmonary disease and a high risk of functional impairment 30 and mobility limitations. 19 Additionally, SPPB scores <7 are generally associated with a higher fall rate in older adults, and an SPPB score <5 can identify patients with a major risk of death after discharge from acute care hospitals. 31 Therefore, different cut-off values of the SPPB score are required for different types of diseases. To the best of our knowledge, this is the first study to examine the cut-off value of the SPPB in patients with CABG.
The potential value of the present study lies in its clinical applications. The SPPB assessment tool is performed in patients undergoing complex surgical procedures because it only takes 10 minutes to complete the assessment. Once a patient is identified as having impaired physical function, surgeons take impaired physical function into consideration and weigh the risks and benefits of surgery. Patients also benefit from interventions to reduce risk, such as a preoperative increase in balance, walking ability, and strength training. Well-designed clinical studies are required to develop targeted risk reduction strategies for patients with impaired physical function.
Three components of SPPB scores predictive of LOHS
In this study, we tested whether any of the three SPPB components (standing balance, 4MGS, and 5STS tests) were suitable for identifying patients at risk of a prolonged postoperative LOHS. We found that the 4MGS test had the largest area under the curve value in ROC analysis than the other two components of SPPB scores. The assessment method and significance of the 4MGS test are the same as those of the 4-m walking speed. The 4-m walking speed is used to predict 30-day mortality and major morbidity in older adult patients undergoing cardiac surgery. 32 Additionally, a recent study showed a significant association between the preoperative gait speed and an increased LOHS following cardiac surgery, which is consistent with our study. 33 Gait speed is an easy-to-determine, valid, and reliable assessment that has been frequently cited as a useful clinical indicator of an individual’s physical frailty and future morbidity and mortality. 34 Gait speed can predict 30-day mortality following transcatheter aortic valve replacement, 35 and there is good interrater and retest reliability. From this point of view, our findings reinforce the concept that gait speed is an established marker for exercise capacity in older adult patients and may prove useful as a component of multidimensional assessment of physical performance in patients with CABG. Therefore, assessing physical performance using a standardized definition can help patients and physicians make more informed decisions.
Although the area under the curve values of the standing balance and 5STS tests were <0.7, this study showed that these two components were also independent risk factors for the LOHS in patients with CABG. Additionally, this relationship remained significant after adjustment for confounding factors. Impaired balance is common in older adults with impaired function. Because strength, muscle mass, and balance are closely interlinked, the 5STS test is an appropriate indicator of lower limb muscle strength and balance. Many cross-sectional and prospective studies have shown that muscle strength is an indicator of functional decline in older individuals. 36 Skeletal muscle, which is the largest tissue of the body, accounts for a high percentage of glucose and protein consumption. Skeletal muscle also plays major roles in maintaining nutritional homeostasis, providing nutrients for the immune system, and rapid tissue repair. 37 Poor nutritional status increases the risk for adverse clinical outcomes, 38 which can lead to an increased risk of a prolonged postoperative LOHS. Therefore, strength and balance are closely related and are important for improving dynamic balance and increasing strength. Additionally, both of these factors help to prevent a decrease in physical function in older patients who undergo elective CABG.
There are some limitations to this study. First, the sample size is the main limitation. This study included all eligible operations in our medical centre, and no a priori sample size was calculated. Second, the discriminative ability of the SPPB may not be sufficiently generalizable to different settings because our study was restricted to a single province of China. Third, our study on prediction using the SPPB in patients with CABG is a relatively new area of research, and there was a limited study time and a lack of relevant previous studies to compare with. Temporal, geographical, and external validation cannot be performed at present. Finally, we only examined the short-term predictive value of the SPPB. Factors indicative of more long-term clinical value need to be assessed in follow-up studies.
In conclusion, this study provides evidence for the clinical utility of the SPPB summary score and the 4MGS test for identifying patients at risk of a prolonged postoperative LOHS after CABG. However, more studies, especially studies with a large and longitudinal design, are required, and cut-off points for the SPPB score should be tested in another sample as a further validation step. Further evidence of the predictive utility of SPPB may lead to SPPB analysis as a standard pre-screening tool for CABG. This tool may subsequently assist physical therapists and other clinicians in identifying patients who may require more intensive services, a longer duration of hospital stay, or placement in a skilled nursing facility before surgery.
Footnotes
Acknowledgements
The authors thank all of the members of the Department of Rehabilitation Medicine for their generous technical assistance and guidance, and the nurse team led by the Department of Surgery for their technical support. We also thank all of the study participants for their kind participation and cooperation.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Shanghai Sailing Program (grant number: 20YF1418200), the Scientific Research Foundation of SUMHS (SSF-21-03-007), and Wu Jieping medical foundation (grant number: 320.6750.17073).
Author contributions
Material preparation, data collection and analysis were performed by Fandi Xie, Xiaocheng Liu, Zhigang Liu, Qi Guo, Bohan Shao, Xiangjing Liu and Bo Yuan. The first draft of the manuscript was written by Peipei Han, Hairui Yu, and Yuanyuan Zhang. All authors commented on various versions of the manuscript. All authors read and approved the final manuscript.