
Abstract
Objective
This study was performed to examine the treatment regimen used for an elderly patient with diffuse large B-cell lymphoma (DLBCL) complicated with renal dysfunction.
Case report
An 85-year-old man presented with nasal and sinus disorders in May 2018. He was also found to have renal insufficiency caused by long-term consumption of compound aminopyrine phenacetin tablets. Physical examination revealed irritation of the nasal mucous membrane on the right side and dark red nasal passages with a smooth surface. The right side of the neck contained several small peanut-sized lymph nodes. A biopsy of the right nasal neoplasm revealed germinal center type DLBCL. The mini–rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone regimen (mini-R-CHOP) was administered as the main chemotherapy regimen. Additionally, the use of thrombopoietin prevented further deterioration in renal function. This individualized treatment program helped the patient to achieve complete remission. The creatinine level decreased and was well maintained.
Conclusion
The mini-R-CHOP and rituximab cross-use regimen was found to be safe in an elderly patient with chronic renal insufficiency. Thrombopoietin exerted a protective effect on renal function.
Keywords
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common type of non-Hodgkin’s lymphoma (NHL) in the elderly population, 1 with an incidence rate of about 30% to 40%. The median age at onset is about 60 to 70 years; 50% of patients are aged more than 60 years, 2 while about 40% of patients are aged more than 70 years. 3 The incidence of NHL increases with age and has doubled in the last two decades. 4
The incidence of adverse reactions to chemotherapy increases with age because of the weak immune system in the elderly, leading to a poor prognosis and high mortality rate in older patients with NHL. Although treatment can result in remission, the long-term survival rate is low. Maartense et al. 5 showed that among patients with NHL, the survival rate was significantly lower in those aged >70 than <70 years. The 5-year survival rate of patients aged 80 to 85 years and >85 years was 15% and 8%, respectively. 5
Elderly patients with DLBCL are a heterogeneous group, and treatment is based mainly on anthracycline chemotherapy drugs. 6 Despite certain efficacy, the treatment is greatly influenced by morphological characteristics, immune phenotypes, genetics, and biology, and many patients do not achieve complete or partial remission and are prone to relapse. 1 The combination of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) is considered the standard treatment for DLBCL. 7 However, the treatment of elderly patients remains challenging. Many elderly patients have renal insufficiency, especially at advanced ages. Renal function is a main factor that limits the standard dose of chemotherapy and affects the prognosis, but no specific prevention or treatment is currently available. This study was performed to examine the treatment of an elderly patient with NHL complicated with renal dysfunction. Thrombopoietin (TPO) was used to prevent the deterioration of renal function, and complete remission was achieved with an individualized treatment program.
Case presentation
The study protocol was approved by the ethics committees of the Second Medical Center and National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing. The participant provided written informed consent.
An 85-year-old Chinese Han man was diagnosed with DLBCL; 23 days later (25 June 2018), he was admitted to the Department of Health Medicine of PLA General Hospital. He was found to have nasal and sinus disorders in May 2018. Positron emission tomography/computed tomography (PET-CT) examination outside the hospital revealed foci of increased metabolic activity on the right side of the frontal sinus, ethmoid sinus, and maxillary sinus and in the nasal cavity. Further, multiple lymph nodes with increased metabolic activity were present on the right side of the neck and bilateral supraclavicular fossae. Hence, malignant lesions were considered. A nasal biopsy was performed, and the postoperative pathological examination revealed right nasal DLBCL (germinal center type). The immunohistochemical results were as follows: AE1/AE3 (−), Ki-67 index (70%), p53 (−), CD3 (scattered +), CD2 (+), CD10 (+), Bcl-6 (+), cyclin D1 (−), and Mum-1 (−). The result of Epstein–Barr virus-encoded RNA in situ hybridization was negative, and the patient was diagnosed with NHL. He also had renal insufficiency due to long-term use of compound aminopyrine phenacetin tablets, and his serum creatinine level was 143 µmol/L. Physical examination revealed irritation of the nasal mucous membrane on the right side and dark red nasal passages with a smooth surface. Multiple hard peanut-sized lymph nodes were palpated on the right side of the neck; these were diagnosed as DLBCL. The patient and his family members refused a lumbar puncture and cerebrospinal fluid examination. An individualized treatment plan was developed according to the patient’s advanced age and renal insufficiency, and TPO (15,000 IU) was administered after each chemotherapy cycle. The first cycle of R-COP chemotherapy was performed in the hospital in July 2018. On 24 July 2018, the second cycle of mini-R-CHOP chemotherapy was performed. After the treatment, no obvious abnormally enlarged lymph nodes were found in the neck or bilateral supraclavicular fossae. The mini-R-CHOP plan was implemented on 14 August 2018 and rituximab was given once in the fourth cycle because of bladder inflammation. The fifth cycle of the mini-R-CHOP program was launched on 9 October 2018. TPO was administered after each of the aforementioned cycles. A systemic PET-CT examination on 15 October 2018 revealed the following: (1) thickening of the left nasal mucosa and a slight increase in metabolism, which we anticipated might change after the treatment (the complete molecular response score was 1–2); (2) increased metabolism on the left side of the nasopharynx, which we considered might be due to nonspecific uptake or inflammation; and (3) right maxillary sinus and ethmoid sinusitis. The detailed treatment plan is shown in Table 1 (the patient agreed to receive the aforementioned treatment and provided written informed consent).
Detailed treatment plan for patient in the present study.

Imaging, routine blood testing, and renal function changes before and after treatment
Comparison of PET-CT imaging before and after treatment
The patient’s physical examination in the hospital revealed irritation of the right nasal mucosa and dark red nasal passages with a smooth surface. Multiple hard peanut-sized lymph nodes were palpated on the right side of the neck. Before the second chemotherapy cycle, no enlarged superficial lymph nodes were found throughout the body, and the nasal mucosa was neither hyperemic nor edematous. No new microorganisms were seen in the middle nasal tract. The patient’s clinical symptoms and signs disappeared. The PET-CT findings were compared before and after the treatment (Figures 1 and 2, respectively).

Positron emission tomography–computed tomography report from Peking Union Medical College Hospital on 5 June 2018, before treatment. A soft tissue density shadow was seen in the right frontal sinus, ethmoid sinus, maxillary sinus, and nasal cavity, with increased radioactive uptake. The standardized uptake value was 20.4, and the shadow was invading the right orbit. The radioactivity uptake increased on the right side of the neck (areas I, II, III, and V) and supraclavicular fossae. The size of the shadow was 0.4 to 1.0 cm, and the maximum standardized uptake value was 1.7 to 8.1.

Positron emission tomography–computed tomography report of PLA General Hospital on 15 October 2018, after treatment. The soft tissue density shadow had disappeared from the right frontal sinus, ethmoid sinus, maxillary sinus, and nasal cavity. The previously observed increased radioactivity uptake was not seen on the right side of the neck (areas I, II, III, and V) or in the supraclavicular fossae. The left nasal mucosa was thickened, and the metabolic activity in this area was slightly increased. The complete metabolic response score was 1 to 2.
Changes in routine blood parameters during treatment
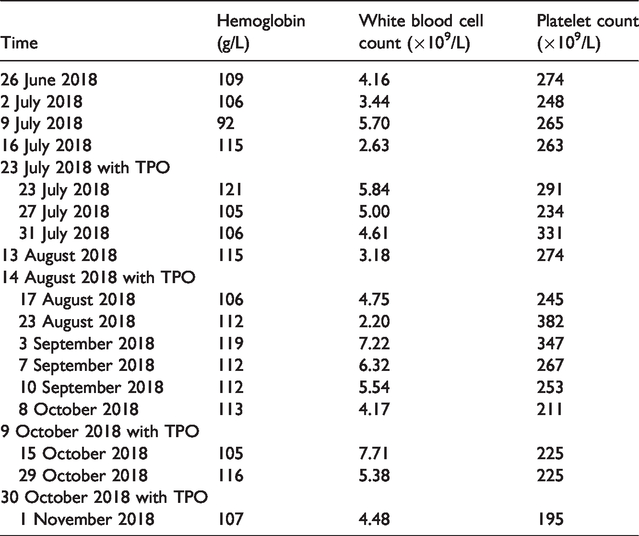
The patient had good tolerance to chemotherapy. No obvious indications of bone marrow suppression were seen except for a slight decrease in the total number of white blood cells on 16 July and 23 August. After each TPO administration, the platelet count increased to different degrees, but the hemoglobin and white blood cell count were not significantly affected (Table 2 and Figure 3).
Changes in hemoglobin level, white blood cell count, and platelet count during thrombopoietin treatment.

Changes in platelet count, hemoglobin level, and white blood cell count during treatment.
Changes in creatinine and urea nitrogen levels after TPO administration
The patient had a history of renal insufficiency caused by long-term use of pain-relieving tablets. After each TPO administration, the creatinine and urea nitrogen levels decreased and then increased until the next TPO administration (Table 3 and Figure 4).
Changes in creatinine and urea nitrogen levels during thrombopoietin treatment.


Changes in renal function (creatinine and urea nitrogen) after thrombopoietin treatment.
Discussion
Chronic renal insufficiency is a common disease among the elderly population. The incidence of renal insufficiency increases gradually with age. Survey data show that the prevalence of chronic kidney disease in patients aged less than 60 years, more than 60 years, and more than 75 years is approximately 10%, 20%, and 50%, respectively. Further, 11% of elderly patients aged more than 65 years without diabetes or high blood pressure have at least stage 3 renal disease. 8 Renal insufficiency has become the bottleneck of clinical drug use and treatment for elderly patients, especially those of very advanced age. While treating elderly patients with chronic renal insufficiency, the treatment plan should be reasonably chosen with consideration of various factors.
The present report described an 85-year-old patient with DLBCL. Despite his good general condition, the patient had chronic renal insufficiency due to long-term use of compound aminopyrine phenacetin tablets. A detailed assessment was performed before the treatment according to the European Society for Medical Oncology Clinical Practice Guidelines, 9 and a comprehensive geriatric assessment was also performed. 10 The patient could not tolerate the standard dose of R-CHOP chemotherapy; therefore, he required either a reduced dose or progressive therapy. R-COP was adopted in the first cycle, and mini-R-CHOP and rituximab cross-use treatment was given on the basis that the renal function did not worsen after chemotherapy with the goal of achieving complete remission.
TPO was administered at the end of each cycle of chemotherapy. After each TPO administration, the patient’s renal function (creatinine and urea nitrogen levels) showed a relatively obvious downward trend and then gradually increased until TPO was administered again after the next cycle of chemotherapy. Therefore, we speculated that TPO might have had a protective effect on renal function in this patient with senile lymphoma. A renal protective function of TPO has not been reported in previous clinical studies, but relevant basic and animal experiments have been conducted. TPO has been found to promote the expression of immediate early gene X-1 (IEX-1) and its related pathways, scavenge free radicals, and promote repair of DNA damage.11–13 Wang et al. 14 confirmed that TPO could promote hematopoietic stem cell regeneration in rats treated with radiotherapy and that TPO administration before radiotherapy could reduce hematopoietic stem cell damage and mutagenesis in mice. DNA damage repair occurred via the DNA–protein kinase-dependent pathway. 15
Our patient’s renal function was stable, and his creatinine level was lower than that during his first admission. We conclude that the mini-R-CHOP and rituximab cross-use regimen was relatively safe for this elderly patient with chronic renal insufficiency. TPO combined with chemotherapy may have a protective effect on renal function; however, its clinical mechanism needs further exploration.
Ethics
The study protocol was approved by the ethics committees of the Second Medical Center and National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing. The participant provided written informed consent.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Bidding Project of the National Center for Clinical Medicine of Geriatric Diseases in 2017 (NCRCG-PLAGH-2017011) and the Translational Medicine Project of PLA General Hospital (2017TM-020).