
Abstract
Objective
The aim of the current study was to evaluate the value of plasma endostatin for predicting 30-day mortality of patients with acute kidney injury (AKI).
Methods
Patients who underwent non-cardiac major surgery and developed AKI in the first 48 hours after admission to the intensive care unit were consecutively included. Concentrations of plasma neutrophil gelatinase-associated lipocalin (NGAL), cystatin C (Cys C), and endostatin were measured at three time points: 0, 24, and 48 hours after the AKI diagnosis. Clinical patient characteristics were recorded after AKI was diagnosed.
Results
A total of 256 new-onset AKI patients were enrolled. Of these, 48 (18.7%) patients died within 30 days. The difference in plasma endostatin values between 0 and 24 hours (ΔEndostatin-24h) yielded the best area under the curve (AUC) of 0.747 for predicting 30-day mortality in AKI patients; NGAL and Cys C achieved AUC of 0.672 and 0.647, respectively. The predictive AUC increased to 0.833 when ΔEndostatin-24h was combined with sequential organ failure assessment score and AKI classification.
Conclusion
Dynamic plasma endostatin is useful for predicting 30-day mortality in AKI patients. The predictive power of dynamic plasma endostatin can be significantly improved when it is combined with clinical patient data.
Keywords
Introduction
Acute kidney injury (AKI) is a common disease and is independently associated with high mortality in critically ill patients. Mortality is substantially higher in patients with even the mildest stage of AKI than in those without AKI.1,2 Early diagnosis, risk stratification, and implementation of effective interventions play important roles in decreasing the mortality of patients with AKI. 3 The appropriate combination of novel AKI biomarkers with clinical patient data may help to predict the development and prognosis of AKI early and provide more information for clinical decision-making, which could help physicians implement early supportive interventions to improve outcomes.4,5
Recently, significant progress has been made in the early diagnosis of AKI. Plasma endostatin is a promising novel biomarker for AKI prediction. Its predictive value is superior to that of neutrophil gelatinase-associated lipocalin (NGAL) and cystatin C (Cys C).6,7 Endostatin derives from the cleavage of collagen XVIII and reflects renal structural damage in early AKI. Collagen XVIII exists widely in the renal tubular epithelium, Bowman’s capsule, and glomerular basal membrane.8,9 When the kidneys are injured, collagen XVIII decomposes and produces endostatin. An elevated plasma endostatin level is closely associated with the severity of renal damage. 10 Therefore, detecting plasma endostatin in the early stage of AKI may indicate the progress and outcome of AKI. However, no studies have explored the prognostic value of plasma endostatin for AKI. The current study was conducted to assess whether serial measurement and trends in plasma endostatin concentration could predict 30-day mortality in non-cardiac postoperative AKI patients.
Materials and methods
Study setting and population
This was a prospective observational study conducted in the 20-bed surgical intensive care unit (ICU) of Beijing Chao-yang Hospital from May 11, 2016, to January 1, 2018. The study was approved by the Human Ethics Committee of Beijing Chao-Yang Hospital, Capital Medical University (Beijing, China; ethics no. 2016-73; approved May 11, 2016). Patient consent forms were submitted and approved by the Human Ethics Committee of Beijing Chao-Yang Hospital, Capital Medical University. Written informed consent from each patient or their next of kin was obtained before patients joined the study.
We screened non-cardiac postoperative patients who stayed in the ICU longer than 48 hours. Patients were prospectively and consecutively enrolled if they developed AKI in the first 48 hours after admission to the ICU. The exclusion criteria were (1) age <18 years; (2) diagnosed with AKI before ICU admission; (3) complicating chronic kidney disease; or (4) insufficient blood samples acquired. Patients taking nephrotoxic drugs (e.g., aminoglycosides, angiotensin converting-enzyme inhibitors, nonsteroidal anti-inflammatory drugs) were enrolled. Enrolled patients had undergone liver surgery; gastrectomy; small bowel resection; colectomy; rectectomy; pancreaticoduodenectomy; reduction and internal fixation of cervical, thoracic, and lumbar vertebra; or closed reduction and internal fixation of fractures. All eligible patients in this study were managed according to the following guidelines: positive treatment of primary disease and complications, and the same principles of organ support and treatment with antibiotics. Renal replacement therapy was initiated if at least one of the following criteria was met: severe hyperkalemia (>6 mmol/L), severe acidosis (pH <7.15), severe pulmonary edema refractory to diuretics, serum urea >40 mmol/L, or oliguria >72 hours. The renal replacement therapy modality was continuous venous-venous hemofiltration.
Clinical endpoint and data collection
The primary endpoint was 30-day mortality of non-cardiac postoperative patients with new-onset AKI. The secondary endpoints were duration of mechanical ventilation, ICU stay, and hospital stay. Patients were followed until 30 days after AKI (in-hospital follow-up during hospitalization; telephone follow-up after discharge). AKI was diagnosed by serum creatinine and urine output criteria, proposed by Kidney Disease: Improving Global Outcomes.11–13 Chronic kidney disease was defined according to the definition of the National Kidney Foundation as estimated glomerular filtration rate (eGFR) <60 mL/minute/1.73 m2 for at least 3 months, irrespective of the cause. The Cockcroft–Gault formula was used to calculate eGFR.14,15
For each patient, patient characteristics, diagnosis, comorbidities, and significant intraoperative risk factors were recorded. Acute physiology and chronic health evaluation (APACHE II) and sequential organ failure assessment (SOFA) scores were assessed on the day that AKI was diagnosed. Serum creatinine was detected at ICU admission and every 12 hours thereafter until 48 hours after admission. Urine output was measured every hour from the urinary catheter until 48 hours after admission.
Blood sampling and assays
Blood samples were collected at predetermined time points: 0, 24, and 48 hours after diagnosis of AKI. The samples were centrifuged immediately after collection at 3000 × g for 10 minutes, and the supernatant was stored frozen at −80°C before analysis. Endostatin, NGAL, and Cys C in plasma were measured by enzyme-linked immunosorbent assay (ELISA) kits [ab100508, lot no. GR3183088-1 (endostatin); ab119600, lot no. GR316206-1 (NGAL); ab179883, lot no. GR308840-1 (Cys C); Abcam, Cambridge, UK]. The technicians measuring biomarkers were blinded to patient information, and the physicians in charge were blinded to the results.
Statistical analysis
All statistical analyses were performed using SPSS Statistics (version 24.0; IBM, Armonk, NY, USA) and R 2.1.2 (https://www.R-project.org/). The variables are presented as mean ± standard deviation (SD), median, or percentiles, as appropriate. Clinical patient data between patients with and without 30-day survival were compared. Student’s t-test or Mann–Whitney U-test was used to analyze continuous variables, and repeated-measures analysis of variance was used to analyze serial measurements of biomarker concentrations. Categorical variables were compared using the Chi-square test or Fisher’s exact test. Univariate analyses were used to screen clinical variables adding risk for 30-day mortality. Variables with p < 0.1 were subsequently included in the multivariate logistic regression model. Receiver operating characteristic (ROC) curve analysis was conducted to assess the predictive accuracy of changed biomarker levels for 30-day mortality. The following values of 0.90 to 1.0 (excellent), 0.80 to 0.89 (good), 0.70 to 0.79 (useful), 0.60 to 0.69 (poor), and 0.50 to 0.59 (not useful) were used to describe areas under the curve (AUCs). 7 A combination of the ROC curve with multivariate logistic regression analysis was performed to further evaluate the predictive value of changed biomarker levels and clinical variables for 30-day mortality. The model fit was assessed by the Hosmer–Lemeshow goodness-of-fit test. The net contribution of changed biomarker levels to predict 30-day mortality was tested by integrated discrimination improvement (IDI) and net reclassification improvement (NRI). A two-sided p-value < 0.05 was considered statistically significant.
Results
Patient characteristics
A total of 2011 non-cardiac postoperative patients were admitted to our ICU during the study period. Among them, 292 (14.5%) patients were diagnosed with AKI in the first 48 hours after admission to the ICU. After excluding ineligible patients, 256 new-onset AKI patients were enrolled. Among the 256 patients, 208 (81.2%) survived to 30 days after AKI. The 30-day mortality of patients with AKI stage 1, 2, and 3 were 8.7%, 19.8%, and 38.3%, respectively. The flow diagram of the study population is shown in Figure 1.

Study flow diagram.
The characteristics of patients surviving and not surviving to 30 days are compared in Table 1. We found no significant difference in demographic characteristics, serum creatinine before surgery, chronic comorbidities, or surgery data between the two groups of patients. However, compared with the non-survivor group, we found a lower incidence of stage 3 AKI (p = 0.045) and a higher incidence of stage 1 AKI (p = 0.038) in the survivor group. Further, non-survivors had more serious illness with higher SOFA scores (7.5 [6.0, 9.0] vs. 6.0 [3.0, 8.0], p = 0.041) and APACHE II scores (13.5 [12.0, 16.0] vs. 15.5 [13.3, 18.7], p = 0.045), more severe bleeding during surgery (800 [200, 1100] mL vs. 350 [150, 900] mL, p = 0.036) and longer ICU stays (10 [6.0, 16.2] days vs. 5.5 [4.0, 11.5] days, p = 0.031) than survivors.
Clinical characteristics of enrolled patients with acute kidney injury (AKI).

Values are median (interquartile range) or n (%).
AKI, acute kidney injury; APACHE II, acute physiology and chronic health evaluation; SOFA, sequential organ failure assessment; COPD, chronic obstructive pulmonary disease; MODS, multiple organ dysfunction syndrome; NGAL, neutrophil gelatinase-associated lipocalin; Cys C, cystatin C; ICU, intensive care unit; MV, mechanical ventilation; RRT, renal replacement therapy; Endostatin-0h, -24h, -48h, plasma endostatin concentration at 0, 24, and 48 hours after AKI diagnosed, respectively; NGAL-0h, -24h, -48h, plasma NGAL concentration at 0, 24, and 48 hours after AKI diagnosed, respectively; Cys C-0h, -24h, -48h, plasma Cys C concentration at 0, 24, and 48 hours after AKI diagnosed, respectively; ΔEndostatin-24h and -48h, difference value of plasma endostatin between 0 and 24 hours, 0 and 48 hours, respectively; ΔNGAL-24h and -48h, difference value of plasma NGAL between 0 and 24 hours and between 0 and 48 hours, respectively; ΔCys C-24h and -48h, difference value of plasma Cys C between 0 and 24 hours and between 0 and 48 hours, respectively.
Plasma endostatin of non-AKI patients in the current study was 49.3 ng/mL. We compared 0-, 24-, and 48-hour plasma biomarker levels and difference values of plasma biomarkers between 0 and 24 hours and between 0 and 48 hours between patients surviving and not surviving to 30 days (Table 1). We observed a trend for biomarker levels to increase in non-survivors and to decrease in survivors from the time of diagnosis of AKI (0 hours) until 48 hours after AKI.
Factors related to 30-day mortality
A logistic regression analysis was performed, where selected independent variables were forced into the model for analysis, and then the independent risk factors were screened. Independent risk factors for 30-day mortality included SOFA score (odds ratio [OR] 1.43, 95% confidence interval [CI] 1.22–1.64, p = 0.036), AKI classification (OR 2.13, 95% CI 1.62–2.59, p = 0.012), 48-hour plasma endostatin (OR 1.08, 95% CI 1.03–1.17, p = 0.028), and difference in plasma endostatin between 0 and 24 hours (ΔEndostatin-24h) (OR 1.10, 95% CI 1.06–1.12, p = 0.013). The data are shown in Table 2.
Multivariate logistic regression analysis of risk factors for 30-day mortality.

CI, confidence interval; OR, odds ratio; SOFA, sequential organ failure assessment; AKI, acute kidney injury; Endostatin-48h, plasma endostatin concentration at 48 hours after AKI diagnosed; ΔEndostatin-24h, difference value of plasma endostatin between 0 and 24 hours.
Prognostic performance of biomarker levels for 30-day mortality
In the predictions of plasma endostatin, NGAL and Cys C, ΔEndostatin-24h yielded the best AUC of 0.747 (95% CI 0.632–0.862, p = 0.001) for predicting 30-day mortality in AKI patients. The predictive power for 30-day mortality was significantly improved when ΔEndostatin-24h was combined with clinical patient data (SOFA score and AKI classification); the AUC increased to 0.833 (95% CI 0.714–0.904, p < 0.001). The predictive model of endostatin-clinical patient data was confirmed by Hosmer–Lemeshow’s test (p > 0.05), supported by both NRI (p = 0.045) and IDI analysis (p = 0.026). In contrast, neither NGAL nor Cys C greatly improved the predictive value for 30-day mortality when combined with clinical patient data. The predictive performance of biomarker levels and combination models are presented in Table 3. The ROC curves of ΔEndostatin-24h and its combination model are shown in Figure 2.
Prognostic performance of biomarker levels and their combination models for 30-day mortality.

AKI, acute kidney injury; SOFA, sequential organ failure assessment; AUC, area under the receiver operating characteristic curve; NGAL, neutrophil gelatinase-associated lipocalin; Cys C, cystatin C; CI, confidence interval; IDI, integrated discrimination improvement; NRI, net reclassification improvement; Endostatin-0h, -24h, -48h, plasma endostatin concentration at 0, 24, and 48 hours after AKI diagnosed, respectively; NGAL-0h, -24h, -48h, plasma NGAL concentration at 0, 24, and 48 hours after AKI diagnosed, respectively; Cys C-0h, -24h, -48h, plasma Cys C concentration at 0, 24, and 48 hours after AKI diagnosed, respectively; ΔEndostatin-24h and -48h, difference value of plasma endostatin between 0 and 24 hours, 0 and 48 hours, respectively; ΔNGAL-24h and -48h, difference value of plasma NGAL between 0 and 24 hours and between 0 and 48 hours, respectively; ΔCys C-24h and -48h, difference value of plasma Cys C between 0 and 24 hours and between 0 and 48 hours, respectively.
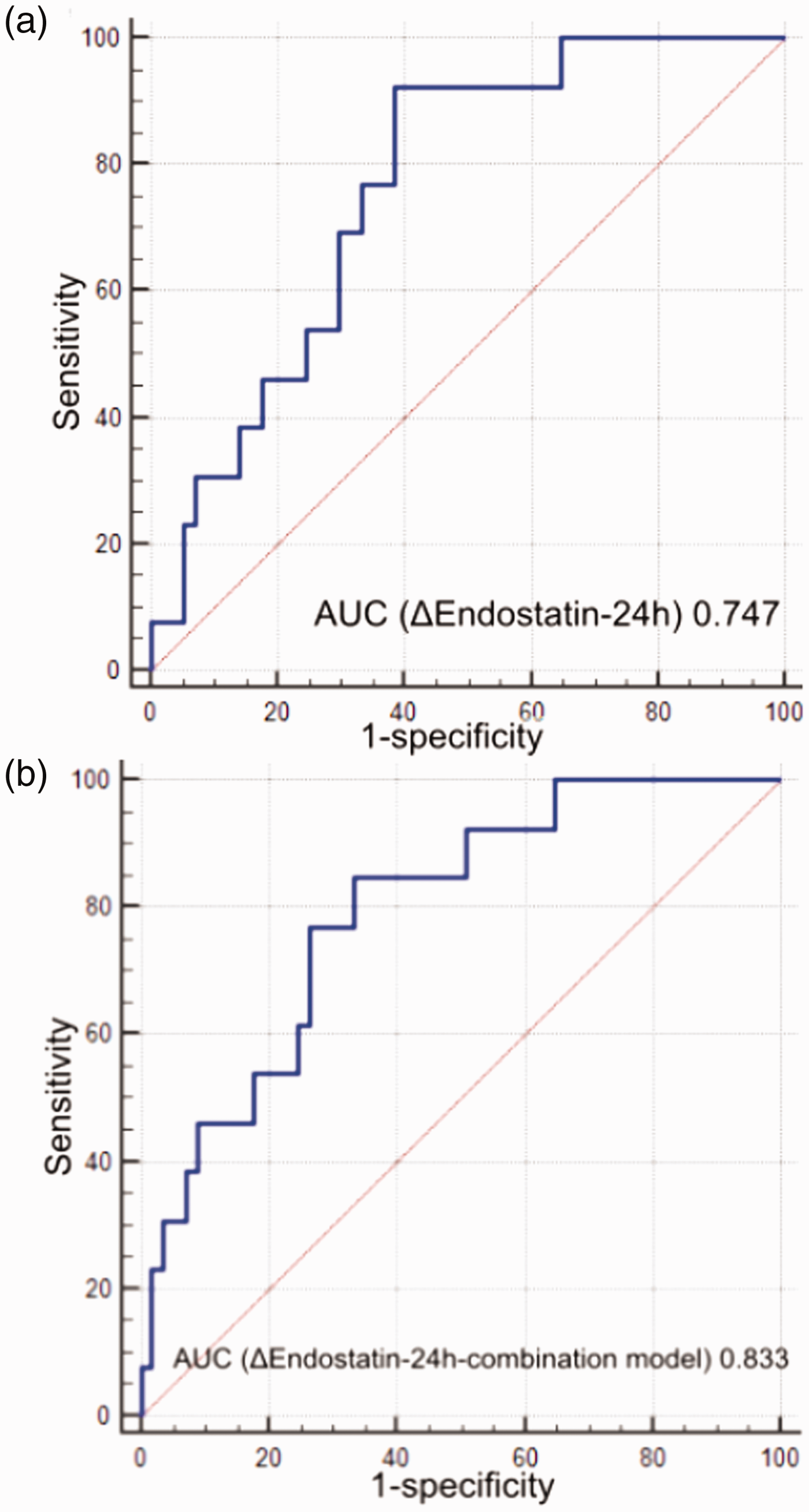
The predictive value of dynamic endostatin and its corresponding prediction model. (a) ROC curve of ΔEndostatin-24h for predicting 30-day mortality in AKI patients. (b) ROC curve of ΔEndostatin-24h combined with clinical patient data for predicting 30-day mortality in AKI patients.
Discussion
The present study represents the first comparative analysis of the prognostic performance of plasma endostatin, NGAL, and Cys C for 30-day mortality in non-cardiac postoperative patients with AKI. ΔEndostatin-24h was the best predictor of 30-day mortality, outperforming NGAL and Cys C. Non-survivors showed a trend for increasing endostatin concentration from time of diagnosis of AKI until 48 hours later, whereas endostatin concentration showed a trend to decline in survivors. Serial measurement and trends of plasma endostatin concentrations may help clinicians recognize those patients who may not survive to 30 days after AKI. The logistic regression model that included endostatin concentration and clinical patient data significantly improved the predictive ability for 30-day mortality, with a maximum AUC of 0.833.
NGAL is considered an important biomarker of damage in the early detection and prognostic prediction of AKI.16–18 NGAL is secreted by epithelial cells of renal tubules in addition to various inflammatory cells. It becomes elevated 48 hours earlier than serum creatinine as a reflection of kidney damage. 19 A study that included patients in the emergency department and used a single urine NGAL measurement found that urine NGAL had predictive ability for prognosis in these patients. 20 Another study showed that plasma NGAL was an independent risk factor for in-hospital mortality in patients with AKI. Cys C is a novel biomarker that has been used in recent years in the early diagnosis of AKI. 21 High Cys C concentrations increase risk for short-term mortality of AKI patients in the ICU. 22 Our study enrolled non-cardiac postoperative AKI patients and detected plasma concentrations of NGAL, Cys C, and endostatin at 0, 24, and 48 hours after diagnosis of AKI. Plasma endostatin, especially ΔEndostatin-24h, had useful predictive value for 30-day mortality, whereas NGAL and Cys C showed poor performance for predicting 30-day mortality.
Endostatin is a newly reported biomarker of AKI. It is produced by cleavage of collagen XVIII, a major constituent of the basement membrane in kidney. 8 Gene expression of endostatin changes in the early stage of kidney injury. 23 Evidence indicates that endostatin participates in the physiological response of renal impairment and is associated with pathophysiological inflammatory processes in the progression of AKI. 24 A continuous increase in plasma endostatin indicates deterioration of renal function. Mårtensson et al. 6 initially showed that endostatin was elevated in the plasma of patients with AKI. Perkins et al. 25 showed that plasma endostatin was elevated in patients with acute lung injury. The lung function of patients in our study was better than that of patients in the study by Perkins et al., as assessed by PaO2/FiO2 ratio. Most of the patients in the current study did not suffer from acute lung injury, although some patients did develop acute liver injury. However, no study has reported correlations of acute liver injury with plasma endostatin level. The elevated plasma endostatin in our study was mainly derived from damaged kidneys.
Previous studies have shown many different baseline values of plasma endostatin concentration in healthy individuals. The baseline values of endostatin were significantly different from the mean concentration of 20.3 ng/mL reported by Gu et al., 26 43.2 ng/mL by Teh et al. 27 to 93.4 ng/mL by Sponder et al., 28 and 105 ng/mL by Shah et al. 29 Concentrations of endostatin are reported to be affected by sex, age, physical activity, muscle mass, and diseases such as like acute lung injury.26,29–31 In our study, the levels of plasma endostatin at diagnosis of AKI were 93.5 ng/mL and 49.3 ng/mL in non-survivors and in patients without AKI, respectively. Mårtensson et al. 6 showed that levels of plasma endostatin in non-AKI and AKI patients were 31 and 42 ng/mL, respectively. The patients with AKI included in our study were older and had more complications than the patient population in the study of Shah et al. 29 Our patients did not exercise on a daily basis and had less muscle mass. Therefore, we consider that the difference in baseline plasma endostatin concentration between AKI patients included here and the healthy population in other studies could be due to less physical activity and muscle mass. Based on these differences, more studies are needed to confirm the related factors for plasma endostatin levels in different populations.
Mårtensson and colleagues 6 reported that endostatin had potential predictive value for AKI in critically ill patients and significantly improved prediction for AKI based on clinical risk factors. Ruge and colleagues 10 conducted a community-based cohort study to investigate the association between circulating endostatin and renal dysfunction in an elderly population. They found that higher circulating marker levels were associated with a lower glomerular filtration rate and independently predicted the development of chronic kidney disease. An increased risk of all-cause mortality was seen in patients with decreased renal function, which was closely associated with plasma endostatin. 32 However, no study has explored the relationship between mortality and plasma endostatin. In our study, endostatin was valuable in predicting 30-day mortality, especially when combined with clinical patient data. If clinicians can accurately assess patients’ condition and predict the progression and prognosis of AKI, treatments of patients with poor prognosis may be changed early to more effective intervention measures. Thus, the adverse outcomes of patients with AKI may be altered and mortality could be reduced.
There are some limitations to this study. First, it was conducted in a single center and included non-cardiac postoperative patients. We did not perform a sample size calculation. The limited number of samples may affect the statistical significance of the results. Second, we were unable to show a relationship between endostatin and long-term prognosis of patients with AKI because many patients were lost to follow up. Future studies are required to investigate the predictive value of plasma endostatin for long-term outcomes in patients with AKI.
Conclusion
Serial measurement of plasma endostatin has useful predictive value for 30-day mortality in AKI patients. The predictive power is significantly improved when plasma endostatin concentration is combined with clinical patient data.
Footnotes
Acknowledgement
We thank Professor Li-Rong Liang in Beijing Chao-yang Hospital for statistical analysis.
Authors’ contributions
H-MJ contributed to data interpretation, drafting of the manuscript and critical revision of the manuscript. YZ and W-LM contributed to data collection and data interpretation and performed statistical analysis. YH and T-EZ contributed to interpretation and revision of the manuscript. J-YJ, XZ, and S-YG contributed to data collection and data interpretation. W-XL chaired the group, conceived and designed the study, performed statistical analysis, and contributed to data collection, data interpretation, and critical revision of the manuscript. All authors reviewed the manuscript, and all authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.