
Abstract
Objective
To determine the prediction ability of the National Early Warning Score (NEWS), National Early Warning Score 2 (NEWS2), and quick Sequential Organ Failure Assessment (qSOFA) score for the prognosis of pulmonary embolism (PE) in the emergency department.
Methods
This retrospective study involved 245 patients with PE. The NEWS, NEWS2, and qSOFA scores were compared according to the hospitalization clinic (ward vs. intensive care unit), hospitalization length (<10 vs. >10 days), severity of embolism (massive vs. submassive), and outcome (discharged vs. died).
Results
The areas under the curve of the NEWS, NEWS2, and qSOFA score for 1-week mortality were 0.854 (sensitivity, 78%; specificity, 73%; cutoff, 7.5; confidence interval, 0.807–0.902), 0.870 (sensitivity, 83%; specificity, 73%; cutoff, 5.5; confidence interval, 0.825–0.915), and 0.789 (sensitivity, 83%; specificity, 51%; cutoff, 0.5; confidence interval, 0.720–0.858), respectively.
Conclusion
The NEWS2 more accurately predicts 1-week mortality than do the NEWS and qSOFA score in patients with PE.
Keywords
Introduction
Pulmonary embolism (PE) is a life-threatening condition, and immediate intervention and treatment are required in patients suspected to have PE. The diagnosis and prognosis of PE have recently become much clearer for emergency clinicians.1–6
The patient’s presentation symptoms, physical examination findings, and laboratory and radiological test results in the emergency department (ED) are useful in the diagnosis of PE. 7 Some clinical scores have been improved for the diagnosis of PE, such as the Wells criteria, revised Geneva score, and Pulmonary Embolism Rule-out Criteria.6,8,9 The Pulmonary Embolism Severity Index (PESI) may help to determine the prognosis of these patients. 10 The PESI includes questions about the patients’ medical history, such as lung cancer. However, predicting the prognosis of patients with PE using basic criteria upon arrival (vital signs only, no questions) has become necessary.
The National Early Warning Score (NEWS) has been used to predict the severity of acute disease in the ED.11–13 This scoring system and modified versions such as the NEWS2 are useful for triage in the ED, especially when the ED is crowded.
The quick Sequential Organ Failure Assessment (qSOFA) is a simple scoring system that is widely used in the ED, especially for identifying patients with sepsis. 14 The clinical uses of the NEWS, NEWS2, and qSOFA score with points are shown in Figure 1.
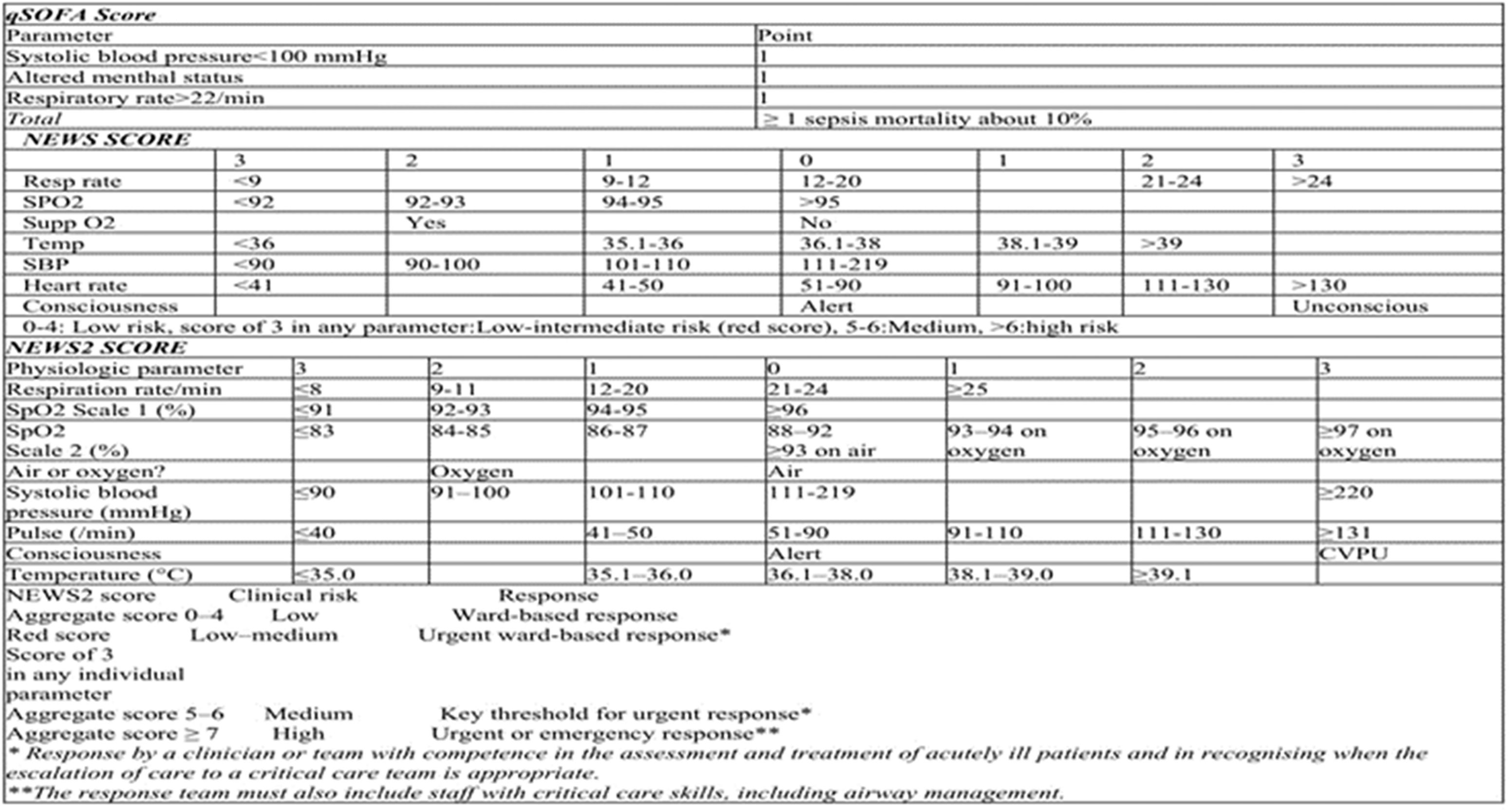
NEWS, NEWS2, and qSOFA score. NEWS, National Early Warning Score; NEWS2, National Early Warning Score 2; qSOFA, quick Sequential Organ Failure Assessment.
The present study was performed to compare the ability of the NEWS, NEWS2, and qSOFA score to predict the prognosis of patients with PE upon arrival in the ED.
Methods
Study design and setting
The reporting of this study conforms to the STROBE guidelines. 15 Patient consent was not required because of the retrospective nature of the study. After obtaining approval from the Adana City Research and Education Hospital Ethics Committee (approval no. 732; approval date: 27 February 2020), we reviewed the data of patients treated in the ED of Adana City Research and Education Hospital from 1 January 2019 to 31 December 2019. The patients’ data were obtained from the hospital automation system. The patients’ age, sex, NEWS, NEWS2, qSOFA score, hospitalization clinic (ward vs. intensive care unit (ICU)), hospitalization length (<10 vs. >10 days), severity of PE (massive vs. submassive), and outcome (discharged vs. died) were noted by two authors blinded to the patients’ data. The diagnosis of PE was validated with thoracic computed tomography angiography. The sample size of this study was calculated using MedCalc software.
Eligibility criteria
This study included all adult patients (>18 years of age) assessed in our ED and diagnosed with PE from 1 January to 31 December 2019. Patients who had undergone cardiopulmonary resuscitation and died in the ED (n = 3) were excluded. Pregnant patients (n = 2) and patients with missing data (n = 12) were also excluded from the study. Our missing data analysis procedures used missing at random (MAR) assumptions. We used the multivariate imputation by chained equations (MICE) method of multiple multivariate imputation. We independently analyzed 10 copies of the data, each with missing values suitably imputed, in the multivariate logistic regression analyses.
Data collection and measurements
Parameters of the NEWS, NEWS2, and qSOFA scores were noted on the study form from the hospital automation system. All clinical signs were measured upon ED arrival. All patients were deidentified. The NEWS, NEWS2, and qSOFA score were calculated for each patient using Microsoft Excel 2010 for Windows (Microsoft Inc., Redmond, WA, USA) from the available physiological measurements.
Outcomes
The primary outcome of this study was mortality. The secondary outcomes were ICU admission, hospitalization of >10 days, severity of PE, and discharge from the hospital.
Statistical analysis
Continuous variables are reported as median (interquartile range) and were compared with univariate analysis by the Mann–Whitney U test. Categorical variables are reported as absolute number (percentage) and were compared by the chi-square test.
Receiver operating characteristic curve analysis was used to estimate the performance of the evaluated scores in predicting the study outcomes. For each threshold score, the sensitivity and specificity were calculated. A p value of 0.05 was considered statistically significant. Data were analyzed using IBM SPSS statistics for Windows, Version 25 (IBM Corp., Armonk, NY, USA).
Results
In total, 150 (61.7%) patients were female and 93 (38.3%) patients were male, and the mean age was 70.2 ± 16.35 years (range, 20–96 years). One hundred eleven patients were diagnosed with massive PE, 58 (23.9%) patients were hospitalized in the ICU, and 167 (68.7%) patients were discharged from the hospital. The 1-week mortality rate was 29.6%.
Most of the patients had a NEWS of 0 points, NEWS2 of 1 point, and qSOFA score of 0 points (Figure 2).
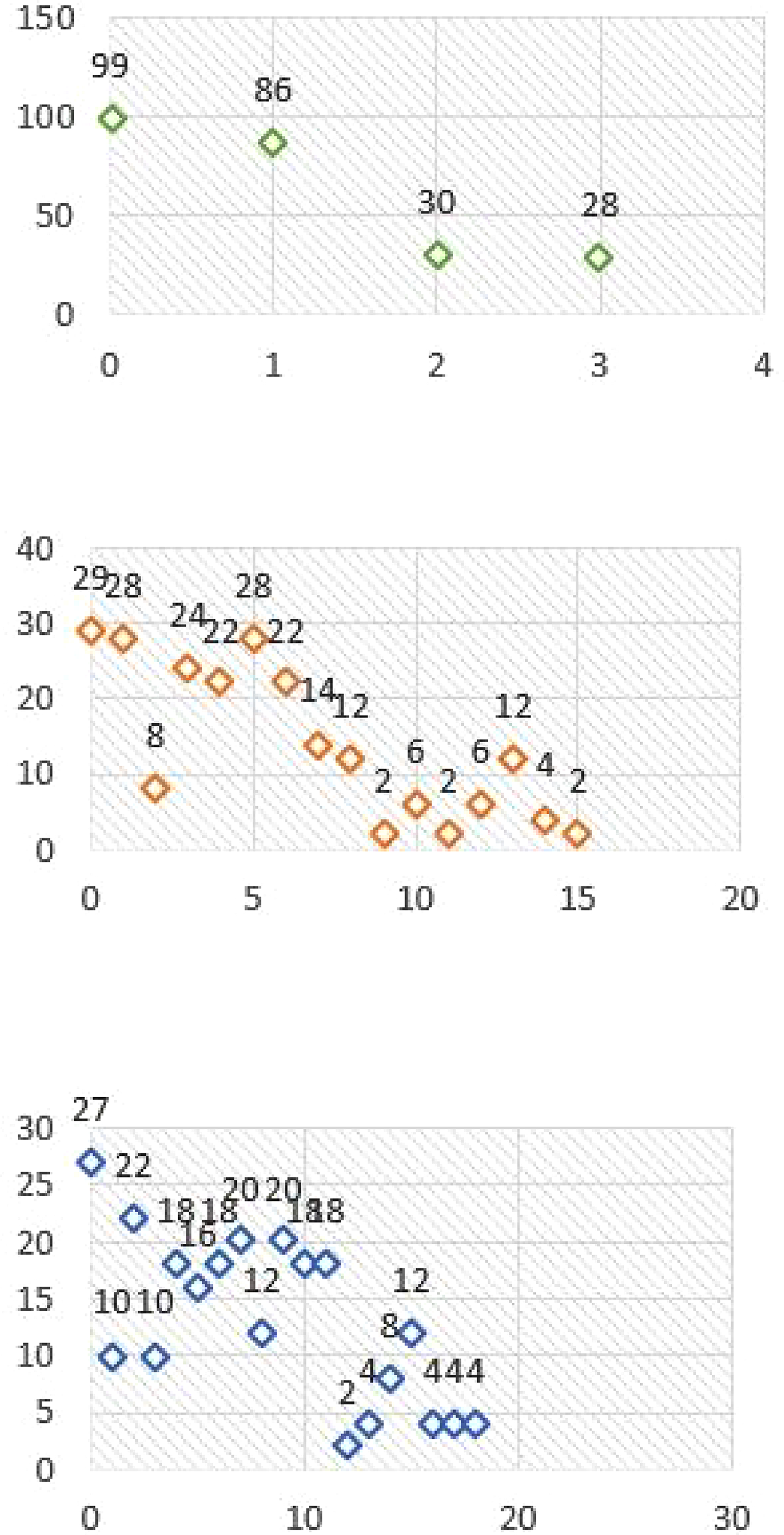
Point frequency graph.
The NEWS, NEWS2, and qSOFA score were significantly different between patients who survived or died within 1 week. The three scores significantly predicted the patients’ hospitalization clinic (inpatient clinic vs. ICU), hospitalization length (<10 vs. >10 days), severity of PE (massive vs. submassive), and outcome (discharged vs. died). Only the qSOFA score for hospitalization length did not significantly differ (Table 1).
Comparison of NEWS, NEWS2, and qSOFA score according to 1-week mortality (died vs. survived), hospitalization clinic (inpatient clinic vs. ICU), hospitalization length (<10 vs. >10 days), severity of embolism (massive vs. submassive), and outcome (discharged vs. died).

NEWS, National Early Warning Score; NEWS2, National Early Warning Score 2; qSOFA, quick Sequential Organ Failure Assessment; SD, standard deviation; CI, confidence interval; ICU, intensive care unit.
The areas under the curve (AUCs) for the NEWS, NEWS2, and qSOFA score for 1-week mortality were 0.854 (sensitivity, 78%; specificity, 73%; cutoff, 7.5; confidence interval, 0.807–0.902), 0.870 (sensitivity, 83%; specificity, 73%; cutoff, 5.5; confidence interval, 0.825–0.915), and 0.789 (sensitivity, 83%; specificity, 51%; cutoff, 0.5; confidence interval, 0.720–0.858), respectively. The AUCs according to 1-week mortality, hospitalization clinic, and outcome are given in Table 2 and Figure 3.
AUCs of NEWS, NEWS2, and qSOFA score according to severity, 1-week mortality, hospitalization clinic, and outcome.

AUC, area under the curve; NEWS, National Early Warning Score; NEWS2, National Early Warning Score 2; qSOFA, quick Sequential Organ Failure Assessment; CI, confidence interval; ICU, intensive care unit.

Receiver operating characteristic curves of NEWS, NEWS2, and qSOFA score according to severity, 1-week mortality, hospitalization clinic, and outcome. NEWS, National Early Warning Score; NEWS2, National Early Warning Score 2; qSOFA, quick Sequential Organ Failure Assessment.
Discussion
Early warning scoring systems are among the most useful triage tools in the ED. Our study showed that in patients with PE, the NEWS2 assessed on arrival at the ED was the most accurate score for predicting the PE severity, ratio of ICU admission, hospitalization length of >10 days, and death within 1 week.
To the best of our knowledge, this is the first study to compare the NEWS, NEWS2, and qSOFA score for prognosis prediction in patients with PE. The PESI is another prognostic score, but it includes parameters other than vital signs, such as the patient’s medical history. The NEWS, NEWS2, and qSOFA score use only vital signs, making their use important when the clinician cannot obtain the patient’s medical history. The NEWS2 includes repetitive oxygen saturation measurements, and the result of the present study suggests that repetitive measurements in a scoring system can more effectively predict the prognosis of patients with PE.
The specificity values of the NEWS2 were higher or lower than those of the NEWS and qSOFA score. For example, the specificity of the NEWS2 was lower than that of the NEWS and qSOFA score for 1-week mortality and the outcome. However, the AUC of the NEWS2 was higher for all parameters, including the hospitalization clinic (ward vs. ICU), hospitalization length (<10 vs. >10 days), severity of PE (massive vs. submassive), and outcome (discharged vs. died). The primary outcome of this study was 1-week mortality, and the AUC of the NEWS2 was higher than that of the NEWS and qSOFA score.
The NEWS and NEWS2 are among the most accurate tools for predicting patient deterioration in the ED. 12 In a comparative study involving 198,755 observation datasets obtained from 35,585 consecutive ED visits, the NEWS more accurately predicted the ICU admission and death ratios than did other scoring systems. 16 The NEWS was updated to the NEWS2 through the addition of a new arterial oxygen saturation scoring scale in patients with type 2 respiratory failure in 2017.17,18
Several studies have focused on the prediction levels of early warning score systems, 13 but there is a lack of data for patients with PE. In our study, the NEWS2 performed better than the NEWS and qSOFA score in predicting ICU admission, hospitalization length, and death within 1 week.
Covino et al. 13 compared various scores for predicting adverse outcomes in patients with COVID-19 admitted to the ED. They calculated the NEWS, NEWS2, modified version of the NEWS2 with the addition of age of >65 years as an independent component (NEWS-C), Modified Early Warning Score (MEWS), qSOFA score, and Rapid Emergency Medicine Score (REMS) from physiological variables measured on arrival. In their study, the NEWS was the most accurate predictor of ICU admission within 7 days (AUC, 0.783; sensitivity, 71.4%), whereas the REMS was the most accurate predictor of death within 7 days (AUC, 0.823; sensitivity, 96.1%). Similar results were observed for ICU admission and death at 48 hours. The MEWS and qSOFA score had the lowest overall accuracy for both outcomes. The authors suggested that the NEWS and REMS measured on ED arrival were the most sensitive predictors of 7-day ICU admission or death in patients with COVID-19. 13
The qSOFA score has been proposed as a prompt to consider possible sepsis in the ED. The criteria with which to calculate the qSOFA score include an altered mental status (Glasgow coma scale score of <15), tachypnea (respiratory rate of >22 breaths/minute), and hypotension (systolic blood pressure of <100 mmHg). The qSOFA is a scoring system for suspected sepsis, and a qSOFA score of ≥2 is associated with a significantly increased risk of hospital mortality. 19 A 10-year study from China combined the qSOFA score with electrocardiography (ECG) findings to determine the risk stratification in patients with acute PE. 20 The study involved 1318 patients (271 in the high-risk group, 1047 in the low-risk group). The authors established a combination predictive scoring system called the qSOFA-ECG score, which was obtained by adding the qSOFA score and the ECG score. The optimal cutoff value of the qSOFA-ECG score was 2, and the sensitivity, specificity, positive predictive value, and negative predictive value were 81.5%, 72.3%, 43.2%, and 93.8%, respectively. The qSOFA-ECG score was superior to the PESI for predicting high-risk stratification and reperfusion therapy. The authors concluded that the qSOFA score contributes to the identification of patients with acute PE who are at risk of hemodynamic decompensation and thus require monitoring and possible reperfusion therapy upon ED arrival when used in combination with the ECG score. 20 In our study, the qSOFA score showed worse performance than the NEWS2.
Conclusion
The NEWS2 seems to be more effective than the NEWS and qSOFA score and may be used to predict the severity, 1-week mortality, ICU admission, and hospitalization length of patients with PE.
Footnotes
Authors’ contributions
SY, AK, NY: conception, design. AK, NY: data collection. AK: statistical analysis. SY,AK: manuscript writing. SY, AK, NY: preparation of final version of the paper.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Data availability
The data of the current study were obtained from our hospital automation system.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.