
Abstract
Objective
Osteoarthritis (OA) patients who undergo staged bilateral total knee arthroplasty (TKA) feel postoperative hyperalgesia in the second operated knee compared with the first knee. Ketamine is an important drug for central temporal summation and inhibition of secondary mechanical hyperalgesia. This study investigated whether central sensitization has a significant effect on hyperalgesia after consecutive operations.
Methods
Seventy-one of 80 OA patients were randomly allocated to the ketamine or saline group. A bolus of ketamine (group K) or saline (group C) (0.5 mg/kg) was injected before induction and at an infusion rate of 3 µg/kg/minute during surgery. A visual analog scale (VAS) was used to assess resting and moving pain and opioid consumption on postoperative days 1, 2, and 3.
Results
The difference in the VAS score between stages 1 and 2 (DV2-V1) was higher in the ketamine compared with the saline group. DV2-V1 for movement between the two groups was not inferior for all periods. Ketamine did not show a large analgesic effect on second-operated knee hyperalgesia in staged bilateral TKAs.
Conclusions
We could not confirm that hyperalgesia was only related to central sensitization with low-dose ketamine. Other factors might be also associated with the hyperexcitability of nociceptive stimuli.
Clinical Research Information Service (CRIS) trial registry no: KCT0001481
Keywords
Introduction
Generally, patients who undergo surgery feel more pain compared with before the operation, regardless of the region that is involved. This phenomenon is related to a reduction in the pain threshold to nociceptive stimuli, and pain is sensed more severely. 1 Patients with osteoarthritis (OA) experience similar results during total knee arthroplasty (TKA). TKA is one of the most painful operations, and this pain limits motion, delays postoperative recovery and rehabilitation, and increases time in the hospital. When bilateral TKA is performed at intervals, it has been shown that greater pain is experienced in the second operated knee, regardless of the degree of damage. 2
Central sensitization originates from extending the receptive fields that are used for normal sensation and amplifying the responses at the spinal level. 3 However, determining the original mechanism of hyperalgesia in staged TKA is difficult, and the exact pain mechanism has not been previously determined.
Ketamine is a phenyl-piperidine derivative that principally acts on hemodynamic stability and psychotic symptoms, 4 which is important for central temporal summation and inhibiting secondary mechanical hyperalgesia. 5 Ketamine causes adverse effects when used at higher doses than the usual anesthetic dose. 6 However, low doses are used for pain control7–11 and administration at a subanesthetic dose does not cause side effects.8,12,13
Using the hypothesis that central sensitization mainly affects hyperalgesia in the second operated knee, we investigated the relationship between central sensitization and hyperalgesia in OA patients who underwent TKA using ketamine, which affects the central pain mechanism.
Methods
Study population
Study subjects were selected from a population of patients with degenerative American Society of Anesthesiologists Physical Status (ASA-PS) grade I to II OA, who were between 20 and 89 years old, and were scheduled for bilateral staged total knee arthroplasty (TKA) at a 1-week interval from March 2015 to March 2016 in Seoul St. Mary’s hospital. Exclusion criteria included a history of postoperative nausea and vomiting (PONV) or side effects of patient-controlled analgesia (PCA); a visual analogue scale (VAS) score for pain ≥4 before surgery at rest; continuous opioid use; use of drugs to treat psychiatric disease or cognitive dysfunction; patients who were not able to follow the instructions for this study; a previous history of TKA; contraindications of ketamine use; or patients with severe heart, liver, or kidney disease.
Ethics
Ethics approval for this study (Ethical Committee No. KE14OIS10567) was provided by the Ethics Committee Institute Research Board (IRB), at the Catholic University of Korea, Seoul St. Mary’s Hospital, Seoul, Korea (Chairman Prof KS Kim) on 10 March 2015 (registration date 11/03/2015). Clinical Research Information Service (CRIS) KCT0001481 approval was provided by the Korea Center for Disease Control and Prevention (KCDC), which was submitted to the WHO ICTRP (International Clinical Trials Registry Platform) on 1 June 2015.
Study design and processing
Participants were assigned to one of two treatment groups: a ketamine group (group K) or a normal saline (NS) group (group C). Randomization was performed by selection of sequentially numbered sealed envelopes containing a group assignment, and these envelopes had been previously assembled based on a computer-based list of random numbers by a person who has used the program and who was unrelated to this study. After parallel allocation of the patients to groups, the study was performed in accordance with relevant guidelines after confirming that informed consent had been provided by all participants. All assigned patients were treated identically. All operations were performed under general anesthesia and by a single surgeon in a standard fashion. All the procedures were performed in a double-blind manner, including the participating patients, orthopedic surgeon, and anesthesiologists who assessed outcomes. Surgery was performed first on the more severely damaged knee. During anesthetic induction in each group, ketamine (group K) or NS (group C) was injected intravenously (i.v.) in a bolus of 0.1 mL/kg (0.5 mg/kg), and infused at a rate of 0.045 mL/kg/hour (3 µg/kg/minute) starting before the skin incision (start of nociceptive stimuli) and continuing until the skin was closed. Each group received ketamine or NS during the second TKA in a same manner. Both groups subsequently received injections of 1% propofol (1.5 mg/kg) and rocuronium bromide (Esmeron® Merck, Kloosterstraat, The NetherlandsPlease click here to enter your response.) (0.8 mg/kg). Anesthesia was maintained using desflurane (4–6 vol%), air (2.5 mL/hour), and O2 (1.5 mL/hour) and remifentanil (0.15–0.2 µg/kg/minute) for intraoperative pain control. For the surgical method, a posterior-stabilized prosthesis (LOSPA; Corentec, Seoul, Korea) was implanted in all patients using the subvatus approach. The patella was not resurfaced, and cement fixation was used for all components in all cases. An intramedullary alignment system was used for the femoral cuts and an extramedullary system was used for the tibial cut. There was no intra-articular injection. When the surgery was almost concluded, we did not change from remifentanil to another opioid to reduce the opioid side effects.
Pain management and the postoperative care plan
The subjects took 400 mg of Celebrex® twice daily beginning at the first TKA to manage postoperative pain and inflammation, and i.v. patient-controlled analgesia (PCA) (Auto Med® 3200, Acemedical, Seoul, South Korea) (1000 µg fentanyl; 1 µg bolus, lock-out time 5 minutes, no background infusion) was also used. The pain score was assessed using a 10-point VAS (0, without pain; 10, the most severe pain). If the pain was continued or suddenly occurred despite the use of PCA, rescue drugs such as fentanyl 50 µg, pethidine 50 mg, and then tramadol 100 mg were administered i.v. in the same order in both groups. Rescue drugs were measured by the total number of uses, not by their category. If patients had opioid complications such as nausea, vomiting, drowsiness, or dizziness, PCA was stopped and replaced with the above rescue drugs. For postoperative nausea and vomiting, 0.3 mg of ramosetron was injected.
Evaluation categories
Preoperative VAS was measured in parallel with the first and second knee before the first surgery. VAS scores were measured in two states: maximum flexion and the resting state. The recruited patients began to exercise (light walking and full extension and 90-degree flexion) on postoperative day (POD) 1 and they began rehabilitation treatment with full knee flexion on POD 2. VAS scores were assessed in the first and second knees on PODs 1, 2, and 3. Total opioid consumption and opioid side effects were also measured. Hyperalgesia and sensitization were assessed using quantitative sensory such as temporal summation or pressure pain threshold). However, sensory testing could not be used because the patients’ operated knees were wrapped with bandages and the patients were wearing braces.
Sample size calculation
This study aimed to show the effect of ketamine on second knee hyperalgesia during staged bilateral TKA. Because of a lack of references, we assessed the VAS scores in the first and second knee 24 hours after surgery in a pilot study that enrolled ten patients, and the mean and standard deviation were 0.5 and 2, respectively. Because TKA was performed under general anesthesia, which is in contrast to the previous TKA, 2 the VAS score in the resting state was 3.4, and the VAS score under maximum movement was 6.8 on POD 1 after the first TKA. This was higher compared with the VAS scores that were reported in the previous study. A significant difference in the pain index was considered to be 2 based on clinical evidence,14–17 but the differences in the VAS scores for the first and second surgeries did not exceed 1. Therefore, a value of 1 was considered to represent the non-inferiority margin (50% rule), which was the delta value. This study was considered to represent the minimal clinically important differences (MCID) that would be a VAS score of 1 and a patient acceptable symptomatic state (PASS), which was considered to be VAS 2. This study was designed as a non-inferiority trial. Based on a two-sided 5% significance value and 80% power, 42 participants were required, and 50 participants were selected, assuming a 10% drop-out rate. At least 25 participants were needed in each group.
Study endpoints
The primary objective was to compare the VAS score difference for maximum pain at rest and during movement on POD 1 in the ketamine group compared with the saline group. Pain during movement was the main end point. The resting state consisted of a lack of stimuli, and decreased pain over time in this state was considered to be a natural phenomenon. The secondary objectives were to compare the maximum VAS scores on subsequent days (PODs 2 and 3) in an exploratory study and PCA use with adverse events in the ketamine group compared with the saline group.
Statistical analysis
We primarily analyzed the data from the clinical study using the per protocol (PP) study population. Baseline demographic data were described using descriptive statistics. All statistical tests were performed using independent t-tests for continuous variables, and the Chi-square test was used for categorical variables. We considered that P values < 0.05 (2-sided) were statistically significant. Analyses were conducted using SAS software, version 9.3 (SAS Institute Inc., Cary, NC, USA). The VAS and PCA consumption were calculated based on a correlation coefficient (CC).
Results
Study flow chart
Among 80 patients who were recruited, five patients were excluded from the analysis before screening, as follows: one patient did not meet the inclusion criteria and four others declined to participate after providing informed consent. Seventy-five patients were randomized. During the study processing, and after randomization, five patients in group C were excluded because they changed their mind about undergoing only a unilateral TKA after the previous TKA (n = 2) or they wanted to expand the interval to more than 1 week between the staged operations (n = 3). Five patients who were scheduled for unilateral TKA initially were included in group K because they changed their mind about undergoing staged bilateral TKA right before the first TKA (n = 5). Therefore, 43 patients in group K and 32 patients in group C participated in the study. As the study progressed and until the end of the study, 40 patients remained in group K except for three who were lost to follow-up (n = 2) or withdrawn from the study (n = 1) because they were transferred to another department during the postoperative period as a result of a thromboembolism. Thirty-one patients were included in group C except for one patient who was lost to follow-up. Data from the remaining 71 patients were analyzed (Appendix 1).
Patients’ baseline characteristics
Preoperative average VAS scores were similar in the two groups. Most of them did not exceed 2 despite a long period of chronic OA in the patients’ daily life. No significant differences were observed in the basic characteristics (e.g. age, sex, ASA-PS) of the patients in groups K and C (Table 1).
Baseline characteristics of the patients.

Continuous variables are expressed as the mean ± standard deviation.
Categorical variables are expressed as the number (percentage).
§VAS of scheduled first TKA: VAS of scheduled second TKA.
VAS, visual analog scale; TKA, total knee arthroplasty; ASA, American Society of Anesthesiologists; BMI, body mass index; N.S., not significant.
Comparison of the VAS scores between groups K and C
The second operated knee exhibited a higher VAS score compared with the first operated knee in both groups. In addition, the VAS scores for the second operation in group K were higher compared with those in group C for all 3 days, but the difference was not significant (Figure 1a and b).

Comparison of the VAS scores between group K and group C. VAS scores at each operation and at each time. (at rest). (b) Comparison of the VAS scores between group K and group C VAS scores at each operation and at each time (while moving).

Comparison of the VAS scores between group K and group C (while moving).
Efficacy test results based on the VAS difference
In this study, the 95% confidence limit (CL) was higher compared with the non-inferiority margin for both the resting and moving states on POD 1 (24 hours) (Table 2–1, Figure 2, and Figure 3).
Efficacy test of the differences between VAS scores (24 hours).

Group C, patients in this group were administered saline.
Group K, patients in this group were administered ketamine.
aDiff, VAS difference (first TKA − second TKA).
VAS, visual analog scale; TKA, total knee arthroplasty; Diff, difference; CL, confidence limit.

Differences in the VAS scores in the resting state within the time period.
Thus, the DV2-V1 of group K was inferior to the DV2-V1 of group C. Based on the exploratory study, the DV2-V1 for group K was also inferior to the DV2-V1 for group C during movement on PODs 2 and 3 (Table 2–2, Table 2-3). However, during rest, the DV2-V1 values for group K on PODs 2 and 3 were lower compared with the non-inferiority margin (Table 2–3 and Figure 2).
Efficacy test of the differences between VAS scores (48 hours).

Group C, patients in this group were administered saline.
Group K, patients in this group were administered ketamine.
aDiff, VAS difference (first TKA − second TKA).
Data are presented as the mean ± standard deviation or as the mean with 95% confidence limit.
*: below non-inferiority margin (1).
VAS, visual analog scale; TKA, total knee arthroplasty; Diff, difference; CL, confidence limit.
Efficacy test of the differences between VAS scores (72 hours).

Group C, patients in this group were administered saline.
Group K, patients in this group were administered ketamine.
aDiff, VAS difference (first TKA − second TKA).
Data are presented as the mean ± standard deviation or as the mean with 95% confidence limit.
*: below non-inferiority margin (1).
VAS, visual analog scale; TKA, total knee arthroplasty; Diff, difference; CL, confidence limit.
Comparison of PCA consumption and side effects
Patients in groups K and C showed similar PCA consumption at each time point. The VAS and PCA were statistically significant based on the CC regardless if the patient was resting or moving (resting: 0.36, 0.24, and 0.13; movement: 0.34, 0.24 and 0.11 at 24, 48, and 72 hours, respectively; P < 0.05). However, these showed a weak correlation despite showing statistical significance. Based on these data, the increase in the VAS scores for group K was not correlated with PCA consumption. This means that the increase in PCA consumption was not proportional to the postoperative pain severity (Table 3–1).
PCA dose after each operation.
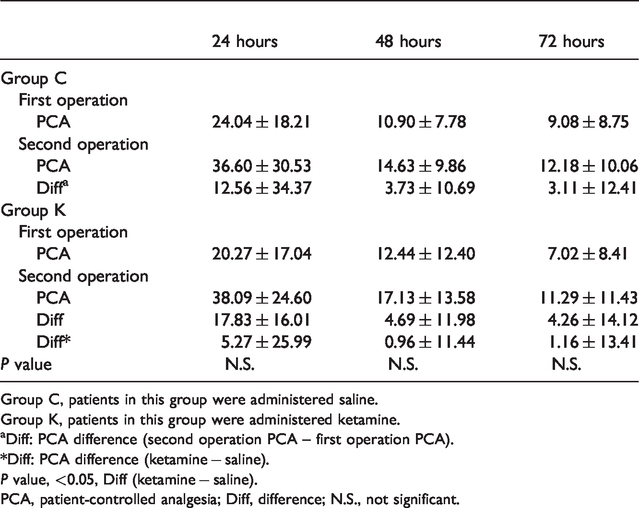
Group C, patients in this group were administered saline.
Group K, patients in this group were administered ketamine.
aDiff: PCA difference (second operation PCA – first operation PCA).
*Diff: PCA difference (ketamine − saline).
P value, <0.05, Diff (ketamine − saline).
PCA, patient-controlled analgesia; Diff, difference; N.S., not significant.
Based on the above results, PCA consumption cannot be used as a main measurement of pain severity. The side effects of PCA, including nausea, drowsiness, and dizziness, were more frequently experienced by group K compared with group C patients, but there was no statistical significance (Table 3–2).
Adverse effects of PCA.
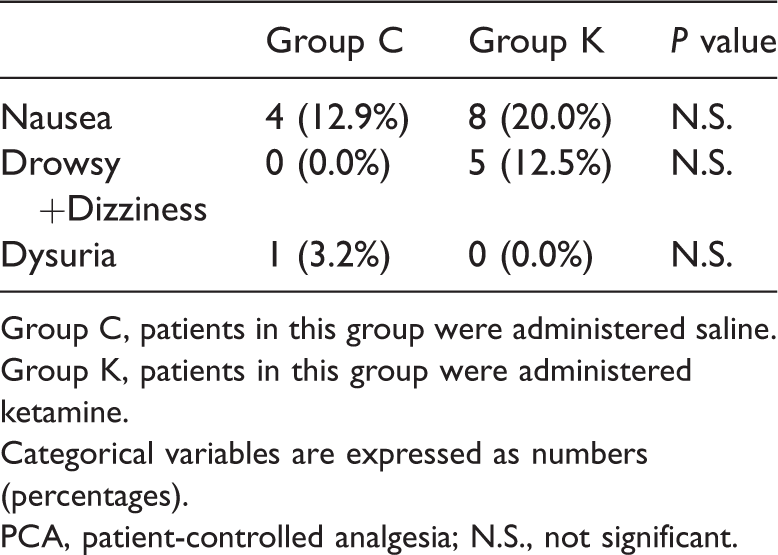
Group C, patients in this group were administered saline.
Group K, patients in this group were administered ketamine.
Categorical variables are expressed as numbers (percentages).
PCA, patient-controlled analgesia; N.S., not significant.
Comparison of rescue drug use
There were no significant differences in the total number of uses at each stage between groups, and within each group, there were no differences between the stages (Table 4).
Comparison of rescue drug use.
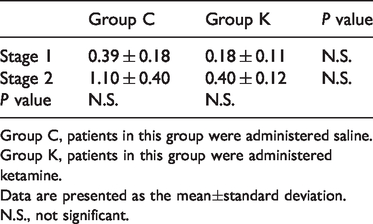
Group C, patients in this group were administered saline.
Group K, patients in this group were administered ketamine.
Data are presented as the mean±standard deviation.
N.S., not significant.
Discussion
This study showed that ketamine did not have a strong analgesic effect on second-operated knee hyperalgesia in staged bilateral TKA.
Previous studies have shown a relationship only between central sensitization for postoperative hyperalgesia and a repetitive nociceptive impulse 2 and acute activity with central sensitization of the N-methyl-D-aspartate (NMDA) receptor. 3 However, based on the results of this study, we suggest that central sensitization was not the most important cause because of the explanations given below, even if chronic OA patients were exposed to pain for a long time.
First, we used the NMDA receptor antagonist ketamine to examine a relationship with central sensitization. Based on the results of previous studies, the VAS score difference (DV2-V1) should be affected by a blockade of the central sensitization that is induced by ketamine, and the DV2-V1 results in group K would subsequently be lower compared with the DV2-V1 in group C. However, the VAS scores were observed on PODs 1, 2, and 3, and they were higher in group K compared with group C. In addition, DV2-V1 was higher in group K at each time point especially during movement and on POD 1 at rest. Based on these results, we could not conclude that central sensitization is the main pain mechanism, and we could not ascertain the effect of ketamine on hyperalgesia.
Second, this phenomenon was generalized hyperalgesia instead of tertiary hyperalgesia. Tertiary hyperalgesia is pain occurring in an area that is distant from the injured tissue, 15 and second and tertiary hyperalgesia are affected by central sensitization. 2 However, in our study, hyperalgesia occurred near the areas and the incision site because it was receiving nociceptive input. This hyperalgesia might not result in tertiary hyperalgesia.
Third, the second operated groups in group K and group C experienced increased pain and consequently increased PCA consumption regardless of ketamine administration. If ketamine had been appropriate for the pain, the total consumption of PCA would have been lower or at least not more compared with the first operated groups. However, in this study, our data did not support the hypothesis that ketamine decreases opioid consumption 18 or the central sensitization hypothesis.
Finally, based on a previous study, 2 the nociceptive input during the first TKA caused hyperalgesia after the second TKA. However, this staged operation had an interval period that was too short to cause hyperalgesia resulting from central sensitization, and we did not think that it was the result of only the first TKA.
Based on the lack of relevance to central sensitization and the pathogenesis of the previously mentioned contralateral hyperalgesia, 19 our results can be interpreted in other ways and their mechanisms should be used for therapeutic approaches. The causes of hyperalgesia are described below.
Regardless of central sensitization, peripheral sensitization plays a large role in maintaining and developing central sensitization. 20 When chronic OA causes central sensitization, more pain would be experienced at a later peripheral incision site compared with a previous incision site. This is caused by sensitization because of inflammatory mediators that are activated by continuous nociceptive input such as TKA, which is a painful operation. Persistent, intense, or repeated input from peripheral sensitization can control the activity of the spinal cord pain-transmitting signals to neurons, reducing the pain threshold and causing pain hypersensitivity by synaptic excitability. 3
Additionally, the mechanism explains the role of neurotransmitters (NTs) in pain and cytokine overexpression. The excitatory NT levels are increased by mechanical nociceptive stimuli in chronic OA over the long term, and various excitatory cytokines are in the activated state. Its activation further increases when TKA is performed repeatedly.
Before this study, the hyperalgesia that was observed in staged bilateral TKA was expected to be related to central sensitization. However, the low-dose ketamine that was used to block central sensitization did not control this hyperalgesia completely. Because pain is mediated by more than one mechanism in a complex manner, blocking central sensitization alone cannot control pain. Other factors, such as psychosocial factors, mood, and coping mechanisms might affect the pain severity. 21
Although the pain observed in the second-stage knee hyperalgesia and in the staged TKA was somewhat influenced by central modulation through increased pain sensitivity and a decreased pain threshold in both knees during the preoperative period, this hyperalgesia was more severe in the injured area because of direct noxious stimuli, which is different from the mechanism of secondary or tertiary hyperalgesia. Therefore, although central sensitization was related to pain episodes, it seemed unlikely to be the largest contributor.
It is thus unlikely that central sensitization alone will play a major role in postoperative hyperalgesia in patients with chronic pain who undergo repeated surgery. The other factors should be identified in addition to the central mechanism. Further studies are warranted to determine whether peripheral sensitization synergistically contributes to the effect of central sensitization on hyperalgesia and the other hyperalgesia pathways.
Limitations of the study
There were some limitations to this study. There was allocation concealment, and a problem of allocation arose because the drop-out frequency increased gradually compared with the initial dataset. In addition, some recruited patients were changed from their assigned group to the other group because they were changed from unilateral TKA to staged bilateral TKA immediately before surgery. Therefore, although the results were based on a randomized controlled trial, 22 there was a difference in the number of patients in each group. Additionally, this study only included the PP population in the analysis.
This study was based on the initial assumption that all recruited patients were already exposed to central sensitization by experiencing chronic pain over long periods of OA. Generally, central sensitization is thought to be induced by pain that lasts for more than 3 months. Therefore, if the time interval that is used in a staged operation is only 1 week, it is difficult to determine the relevance of surgical injury to central sensitization.
Summary
For staged bilateral TKA, hyperalgesia at rest after the second knee operation was not significantly affected by ketamine. It is difficult to conclude that central sensitization alone increased pain sensitivity. Other mechanisms might have contributed to the decrease in the pain threshold, and blocking central sensitization alone did not control pain completely. Thus, hyperalgesia following staged bilateral TKA in patients with chronic OA involves central sensitization and many other variables, such as peripheral sensitization, genetics, and personality factors, in this hyperalgesic mechanism.
Supplemental Material
sj-jpg-1-imr-10.1177_0300060520938934 - Supplemental material for Does central sensitization affect hyperalgesia after staged bilateral total knee arthroplasty? A randomized controlled trial
Supplemental material, sj-jpg-1-imr-10.1177_0300060520938934 for Does central sensitization affect hyperalgesia after staged bilateral total knee arthroplasty? A randomized controlled trial by Hyun Jung Koh, Yong In, Eun Sung Kim, Jae Woong Hwang, Ji Yeong Kim, Soo Jin Lim and Hue Jung Park in Journal of International Medical Research
Supplemental Material
sj-jpg-2-imr-10.1177_0300060520938934 - Supplemental material for Does central sensitization affect hyperalgesia after staged bilateral total knee arthroplasty? A randomized controlled trial
Supplemental material, sj-jpg-2-imr-10.1177_0300060520938934 for Does central sensitization affect hyperalgesia after staged bilateral total knee arthroplasty? A randomized controlled trial by Hyun Jung Koh, Yong In, Eun Sung Kim, Jae Woong Hwang, Ji Yeong Kim, Soo Jin Lim and Hue Jung Park in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_0300060520938934 - Supplemental material for Does central sensitization affect hyperalgesia after staged bilateral total knee arthroplasty? A randomized controlled trial
Supplemental material, sj-pdf-3-imr-10.1177_0300060520938934 for Does central sensitization affect hyperalgesia after staged bilateral total knee arthroplasty? A randomized controlled trial by Hyun Jung Koh, Yong In, Eun Sung Kim, Jae Woong Hwang, Ji Yeong Kim, Soo Jin Lim and Hue Jung Park in Journal of International Medical Research
Supplemental Material
sj-jpg-4-imr-10.1177_0300060520938934 - Supplemental material for Does central sensitization affect hyperalgesia after staged bilateral total knee arthroplasty? A randomized controlled trial
Supplemental material, sj-jpg-4-imr-10.1177_0300060520938934 for Does central sensitization affect hyperalgesia after staged bilateral total knee arthroplasty? A randomized controlled trial by Hyun Jung Koh, Yong In, Eun Sung Kim, Jae Woong Hwang, Ji Yeong Kim, Soo Jin Lim and Hue Jung Park in Journal of International Medical Research
Supplemental Material
sj-pdf-5-imr-10.1177_0300060520938934 - Supplemental material for Does central sensitization affect hyperalgesia after staged bilateral total knee arthroplasty? A randomized controlled trial
Supplemental material, sj-pdf-5-imr-10.1177_0300060520938934 for Does central sensitization affect hyperalgesia after staged bilateral total knee arthroplasty? A randomized controlled trial by Hyun Jung Koh, Yong In, Eun Sung Kim, Jae Woong Hwang, Ji Yeong Kim, Soo Jin Lim and Hue Jung Park in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.