
Abstract
Objective
Angiolipoma is a benign tumor that rarely occurs in the gastrointestinal (GI) tract. This case series was performed to increase clinicians’ understanding of the diagnosis and management of GI angiolipoma.
Methods
We evaluated the clinical presentations, diagnoses, and treatments of 3 patients with angiolipoma in the upper GI tract in our hospital and 27 cases reported in the literature.
Results
Among all 30 cases of GI angiolipoma, 2 originated in the esophagus, 4 in the stomach, 2 in the duodenum, 1 in the jejunum, 7 in the ileum, 1 in the cecum, 9 in the colon, 2 in the rectum, and 2 in both the duodenum and colon.
Conclusion
Angiolipoma of the GI tract may be more likely to occur in middle-aged and elderly men and be located in the ileum and colon. The clinical manifestations generally involve upper GI hemorrhage and lower GI pain and obstruction. Computed tomography and endoscopy may be effective diagnostic techniques, but postoperative histopathologic examination is still the gold standard. The management of angiolipoma in the GI tract depends on the size and type of lesion. Most cases in the present series were managed by complete surgical resection, after which no recurrence was found.
Introduction
Angiolipoma, a common benign tumor composed of adipose tissue and proliferative vascular components,1–3 usually occurs in the subcutaneous tissues of the extremities and trunk. 4 Angiolipoma of the gastrointestinal (GI) tract is extremely rare2,5; we identified only 27 cases reported in English-language publications from 1989 to 2018. Although radiological techniques such as computed tomography (CT) and endoscopy are helpful for reaching a diagnosis,6–9 the gold standard diagnostic method is still histopathologic examination. We herein describe three cases of angiolipoma of the GI tract from 1983 to 2018 in Peking Union Medical College Hospital (PUMCH) and further review the literature regarding angiolipoma of the GI tract to discuss the clinical manifestations, diagnosis, and treatments of this condition. Our aim is to increase clinicians’ understanding of the optimal methods of diagnosis and treatment.
Materials and methods
Patients
Three patients were diagnosed with angiolipoma of the GI tract from January 1983 to December 2018 in PUMCH. We also identified 27 cases reported in the English-language literature from 1989 to 2018; these case reports were retrieved from PubMed.
Methods
The age and sex of the 30 patients; localization and sizes of the tumors; and symptoms, diagnostic methods, therapies, histopathological findings, and follow-up were documented and retrospectively analyzed. The medical services performed for the three patients treated in our hospital were recorded in detail.
Results
Case 1
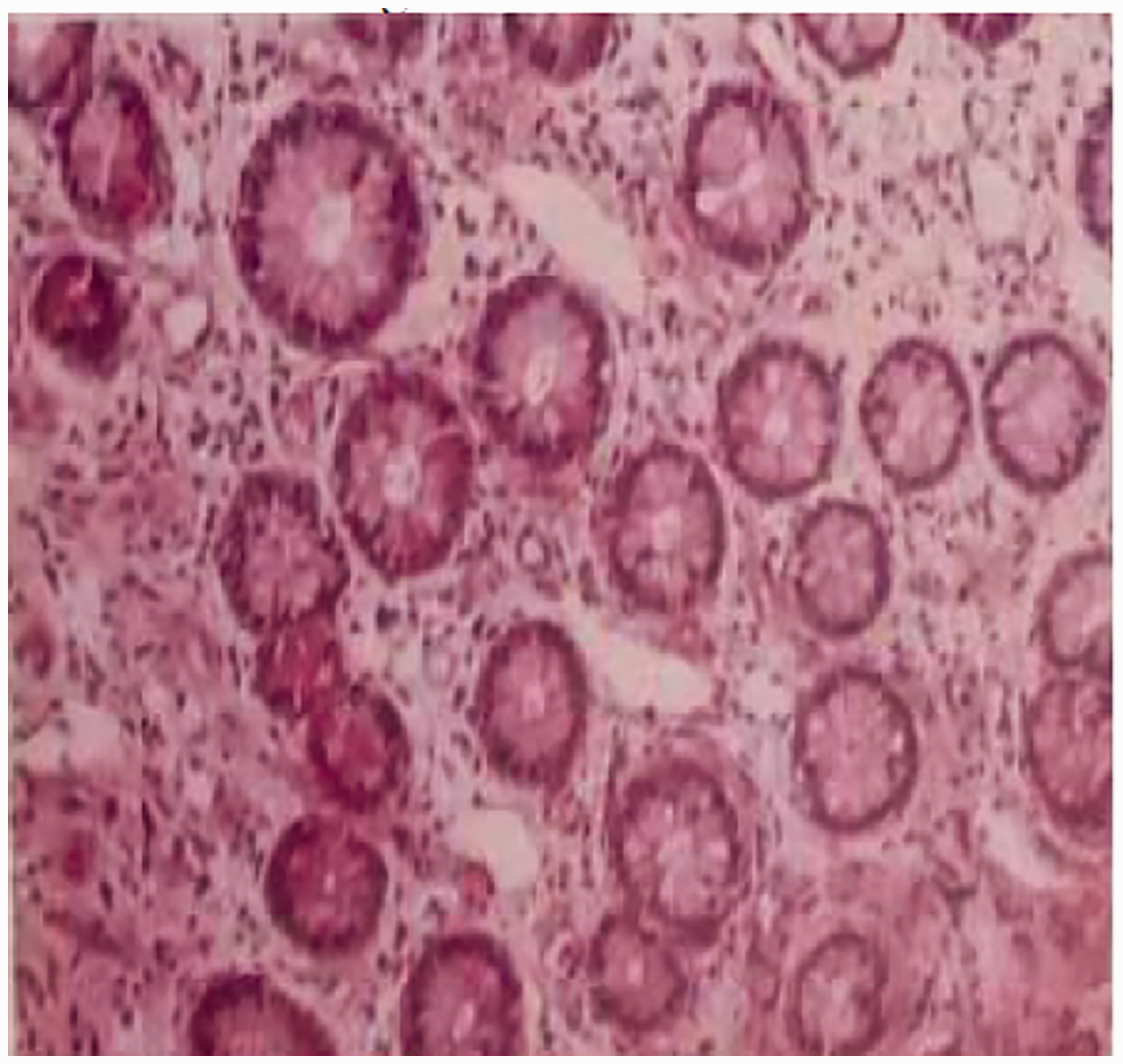
Case 1 involved a 48-year-old woman who was admitted to our hospital on 6 September 2018 with a 1-month history of lower abdominal pain with diarrhea. Her medical history included hypertension for 7 years, diabetes for 1 year, and acute cholecystitis for which open cholecystectomy had been performed 7 years previously. Physical examination on arrival at our hospital revealed mild tenderness in the upper right abdomen and a circular lump of about 5 × 5 cm in diameter palpated in the right upper abdomen. The mass had a clear boundary, moderate mobility, and normal overlying skin. The remaining physical examination and laboratory test results, including routine blood examination, liver and kidney function tests, blood coagulation parameters, and tumor markers [alpha fetoprotein, carcinoembryonic antigen, cancer antigen (CA) 19-9, CA242, CA125, and CA72-4], were unremarkable. Abdominal contrast-enhanced CT showed changes consistent with intussusception at the colonic hepatic flexion and transverse colon (Figure 1). Colonoscopy performed in another hospital showed a mass in the hepatic flexure of the colon. Biopsy showed chronic inflammation of the mucosa with hyperemia and erosion. A barium enema showed an irregular lamellar filling defect in the hepatic flexure of the colon with obstructed passage of contrast material. According to the patient’s medical history and related examination findings, we determined that an intussusception had caused an incomplete intestinal obstruction, and colon cancer could not be ruled out. Therefore, the patient underwent laparoscopic-assisted radical resection of the right colon. Intraoperatively, the mass was found to be approximately 4.0 cm in diameter, located in the right segment of the transverse colon, and protruding into the intestine, resulting in partial narrowing and obstruction (Figure 2). Postoperative histopathology showed that the mass in the hepatic flexure of the colon was consistent with colonic angiolipoma (Figure 3). Examination also revealed ulceration on the mucosal surface and chronic inflammation of the mesenteric lymph nodes. Among seven lymph nodes found, none exhibited metastatic carcinoma. During the 6-month follow-up, the patient showed no recurrence.
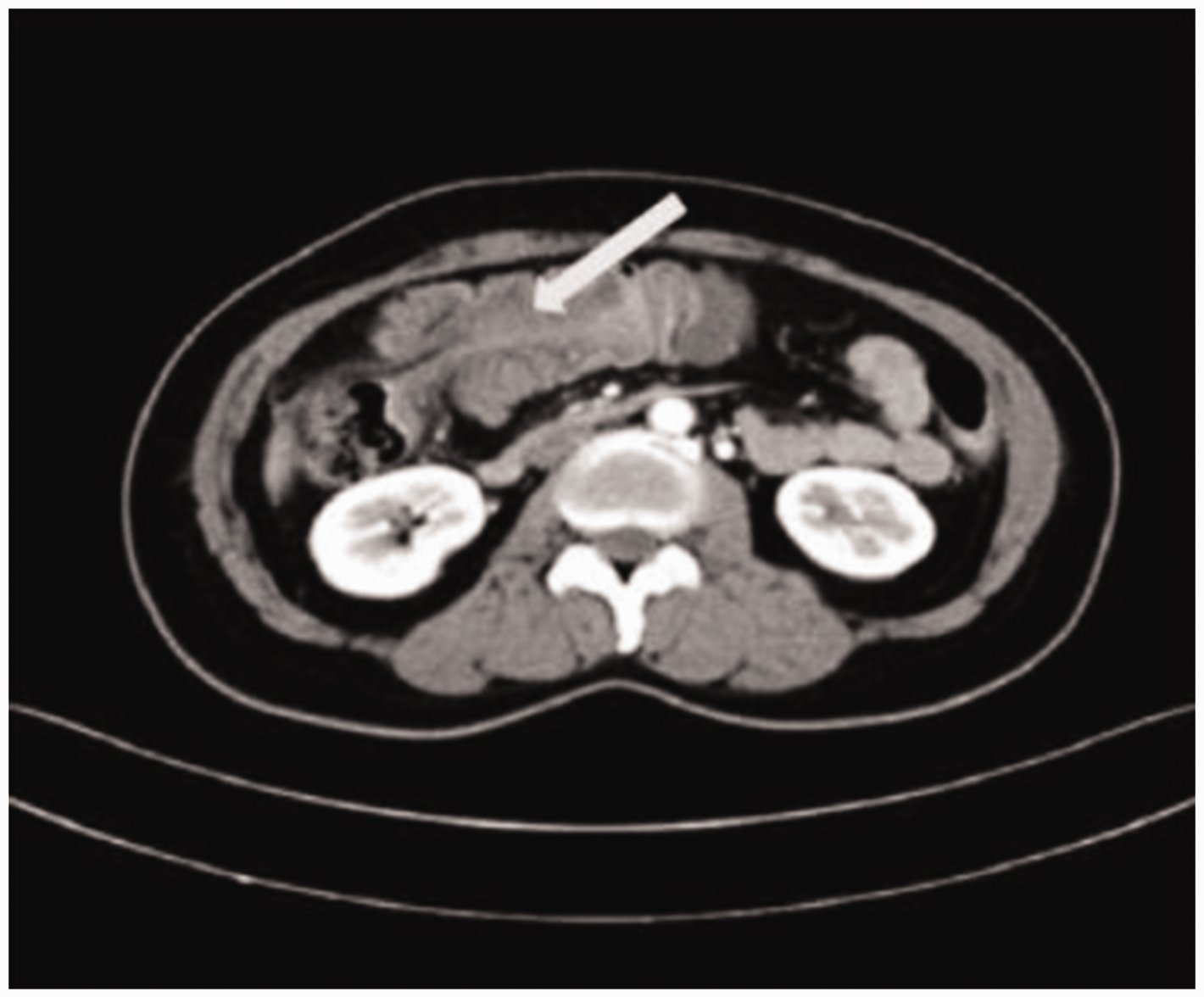
Abdominal contrast-enhanced computed tomography in Case 1 showing intussusception changes at the colonic hepatic flexion and transverse colon.

Gross appearance of colonic angiolipoma in Case 1. The mass was approximately 4.0 cm in diameter, protruding into the intestine and resulting in partial narrowing, leading to obstruction; ulceration was observed on the mucosal surface.

Postoperative histopathology in Case 1 showing that the mass in the hepatic flexure of the colon was consistent with a colonic angiolipoma.
Case 2
Case 2 involved a 52-year-old man who was admitted to our emergency department on 31 May 2015 with a 3-day history of upper abdominal pain with blood in the stool, accompanied by nausea and vomiting. Physical examination on arrival at our hospital revealed only tenderness in the lower right abdomen; the remaining physical examination was unremarkable. On laboratory testing, routine blood parameters were unremarkable except that the lymphocyte ratio (10.7%) and hemoglobin level (115 g/L) were slightly low, and liver and kidney function tests showed a low albumin level (27 g/L) and calcium level (1.82 mmol/L); blood coagulation parameters and the procalcitonin level were both unremarkable. Abdominal enhanced CT showed concentric changes from the ileocecal region to ascending colon (Figure 4). Abdominal ultrasound (US) revealed concentric circles in the right abdomen. Finally, partial enterectomy was performed. Postoperative histopathologic examination showed angiolipoma of the terminal ileum. During the 3-year follow-up, the patient showed no recurrence.

Abdominal contrast-enhanced computed tomography in Case 2 showing concentric changes from the ileocecal to ascending colon.
Case 3
Case 3 involved a 68-year-old woman who was admitted to our hospital on 1 October 2005 with a 2-week history of abdominal pain with the inability to pass gas or defecate and a 1-week history of blood in the stool. On her physical examination, mild epigastric and right upper abdominal tenderness was noted, but no rebound tenderness or masses were identified. Laboratory test results upon arrival at our hospital, including routine blood tests, liver and kidney function, blood coagulation parameters, and tumor markers (alpha fetoprotein, carcinoembryonic antigen, CA19-9, and CA125), were unremarkable. Abdominal radiographs obtained in the erect and supine positions showed a suspicious gas:liquid ratio. Enteroscopy showed a large strip-shaped space in the transverse colon near the hepatic flexure. A biopsy showed chronic inflammation of the colonic mucosa (Figure 5), and a barium enema showed intussusception of the ileocolon. Therefore, the patient underwent a partial ileectomy and right hemicolectomy. Postoperative pathologic examination showed intermuscular angiolipoma of the terminal ileum. During follow-up, the patient showed no recurrence.
Biopsy in Case 3 showing chronic inflammation of the colonic mucosa.
Previously published cases
We identified 27 cases of GI angiolipoma reported in the English language (Table 1); including our 3 cases, there were 30 cases. Among these 30 cases, 9 (30.00%) were located in the colon,10–15 7 (23.33%) in the ileum,16–20 4 (13.33%) in the stomach,5,21–23 2 (6.67%) in the esophagus,24,25 2 (6.67%) in the duodenum,6,26 2 (6.67%) in the rectum,27,28 2 (6.67%) in both the duodenum and colon,26,29 1 (3.33%) in the jejunum, 30 and 1 (3.33%) in the cecum. 31 The 30 patients comprised 20 men and 10 women. Two patients were <30 years old, 3 were 40 to 50 years old, and the remaining patients (83.3%) were >45 years old.
Reported cases of angiolipoma.
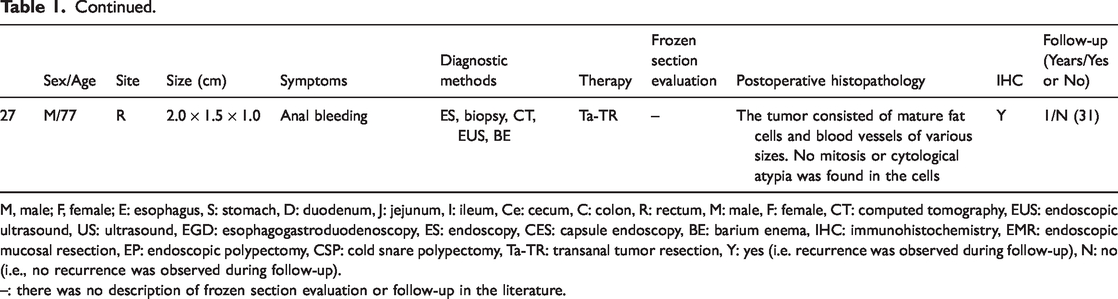
M, male; F, female; E: esophagus, S: stomach, D: duodenum, J: jejunum, I: ileum, Ce: cecum, C: colon, R: rectum, M: male, F: female, CT: computed tomography, EUS: endoscopic ultrasound, US: ultrasound, EGD: esophagogastroduodenoscopy, ES: endoscopy, CES: capsule endoscopy, BE: barium enema, IHC: immunohistochemistry, EMR: endoscopic mucosal resection, EP: endoscopic polypectomy, CSP: cold snare polypectomy, Ta-TR: transanal tumor resection, Y: yes (i.e. recurrence was observed during follow-up), N: no (i.e., no recurrence was observed during follow-up).
–: there was no description of frozen section evaluation or follow-up in the literature.
Discussion
Angiolipoma was initially reported in 1912 by Bowen. 32 In 1960, Howard and Helwig 4 described the differences in the clinicopathological features of angiolipoma and lipoma. According to the composition ratio of adipose and vascular tissues, angiolipomas can be divided into predominantly lipomatous and predominantly angiomatous. Angiolipomas are benign tumors that can occur in most subcutaneous adipose tissues of the body; they are usually found as a single mass or multiple masses on the arms or trunk and are accompanied by pain. 33 However, angiolipomas rarely occur in the GI tract. When they do occur in this location, they are usually found in the ileum and colon of middle-aged to elderly men.
The pathogenesis of GI angiolipoma is still unclear. However, to the best of our knowledge, all 20 subcutaneous angiolipomas from 10 patients had normal karyotypes in a study by Sciot et al.. 34 This finding is in stark contrast to ordinary lipomas, which usually have karyotypic abnormalities involving 12q, 6p, and 13q.4,35 Additionally, among 35 karyotyped subcutaneous angiolipomas reported in other literature, all but one showed a normal karyotype.36,37 The finding that subcutaneous angiolipomas have a virtually consistent normal karyotype more likely supports their clinicopathologic impression of being reactive or hamartomatous. 34 However, whether GI angiolipomas are similar to this requires further study. The pathogenesis of GI angiolipoma may be associated with connective tissue degeneration caused by inflammatory stimuli, adipose tissue deposition caused by lymphatic circulation disorders, congenital dysplasia, systemic lipodystrophy, and intestinal malnutrition.
Most patients with angiolipomas of <2 cm in diameter may have no obvious symptoms, but those with tumors of >2 cm often have abdominal pain, diarrhea, bloody mucoid stools, acute or chronic bleeding, anemia, weight loss, and intra-abdominal masses, among other symptoms. The tumors in 23 (76.67%) of the 30 patients discussed in the present article were >2 cm in diameter, and 14 (46.67%) caused obstruction or intussusception. Only one (3.33%) patient had no obvious symptoms; this patient had a tumor of <0.6 cm in diameter. Additionally, 17 (56.67%) tumors were identified because of acute or chronic bleeding, and 14 (46.67%) were accompanied by pain focused in the lower GI tract. Therefore, the clinical manifestations of angiolipoma are not very specific and have a close relationship with the volume of the tumor, complicating the diagnosis.
In terms of the preoperative diagnosis of angiolipoma in the GI tract, the currently used auxiliary examinations mainly include barium radiographs, CT, magnetic resonance imaging (MRI), abdominal US, endoscopy, and endoscopic US. Among the 30 patients, 19 (63.33%) underwent CT and 24 (80.00%) underwent endoscopy, but only 8 (26.67%) had biopsies that showed chronic inflammation of the mucosa. In addition, 7 (23.33%) patients underwent a barium enema, 6 (20.00%) underwent US, and only 1 (3.33%) underwent MRI. In most cases, angiolipoma cannot be diagnosed on the basis of the results of one of these diagnostic modalities; therefore, a combination of these methods is needed. An angiolipoma is usually visualized as a filling defect in the lumen on barium enema, 9 a heterogeneous hyperechoic mass on abdominal US, 38 and a submucosal mass in the GI wall on endoscopic US. 25 On enhanced CT, the characteristics depend on the tissue composition. For predominantly lipomatous angiolipomas, no contrast enhancement can be observed, and they are usually diagnosed as lipomas. 8 In contrast, predominantly angiomatous angiolipomas show many small round, dense enhancements.39,40 Thus, because the CT findings are not entirely specific, they may not be very helpful when trying to distinguish angiolipomas from other types of tumors. However, they can provide tumor density and blood supply measurements, which can preliminarily distinguish between benign and malignant tumors and clearly define the relationship of the tumor tissue with the surrounding tissues and blood vessels. When an angiolipoma is viewed on MRI, the T1-weighted phase appears as a peripheral isointense signal and central highly intense signal, T1-weighted out-of-phase MRI shows low signal intensity, and dynamic MRI enhanced with fat suppression shows peripheral strong enhancement with an area of central mild enhancement. 19
Another examination technique is endoscopy. Endoscopic examination allows physicians to visually locate the mass and perform a biopsy when conditions permit, which may be helpful in distinguishing the angiolipoma from a malignant tumor prior to the operation. However, some small lesions, including intestinal lesions, cannot be detected on endoscopy. Although capsule endoscopy can solve some of these problems, it is still difficult to directly observe the whole GI tract under endoscopy and find masses. Among the 24 patients who underwent endoscopy, 3 had negative findings on normal endoscopy; these patients’ tumors were found by with capsule endoscopy (n = 2) and MRI (n = 1). In other words, although many methods can be used to achieve an exact diagnosis, the most common and accurate methods may still be CT and endoscopy, and we identified 13 (43.33%) patients in whom both CT and endoscopy were used.
In most cases, a swollen mass was observed in the intestine; the mass was solid, the cut surface usually appeared grayish yellow, and the texture ranged from soft to medium. As Table 1 shows, nearly all of the angiolipomas were histologically identical. Angiolipomas are composed of mature adipose tissue with interspersed vascular proliferation. These lesions are usually ulcers on the mucosal surface that are accompanied by active inflammation and reactive epithelial changes and exhibit fibrinopurulent exudates. 41 Preoperative colonoscopy biopsy is mostly confined to the mucosa, while angiolipoma of the GI tract is mainly located under the mucosa; thus, a biopsy may only show nonspecific features. Intraoperative frozen section evaluation may be a useful adjunct diagnostic method in the setting of local resection. Only three patients underwent this evaluation, which indicated that the tumors were angiolipomas (Table 1); thus, partial enterectomy was performed. As for many other tumors, postoperative histopathologic examination is still regarded as the gold standard for diagnosing angiolipomas, and biopsy and frozen section evaluation may be helpful to some degree.
Generally, angiolipomas can be diagnosed by hematoxylin staining, and immunohistochemistry is rarely required. If needed, immunohistochemistry may be positive for proteins in the adipocytes and endothelial markers in the vascular components. Only six patients in the present review underwent immunohistochemical tests, and the results were different (Table 1). Immunohistochemistry was also performed in the third patient in our hospital, showing positivity for CD34 and CD31. Therefore, it may be inferred that immunohistochemical testing is not very helpful for diagnosing angiolipoma. In addition, unlike other adipocytic neoplasms, angiolipoma usually has a cytogenetically normal karyotype. 38 This may indicate a difference in the pathogenesis of angiolipomas and other adipocytic neoplasms.
The treatment of angiolipoma is determined by its size. Small pedunculated polyps can be resected endoscopically. However, angiolipoma is often found only in the presence of complications such as blood in the stool, obstruction, and intussusception; thus, most angiolipomas are not identified in the early stage, and the best time for endoscopic resection has already passed. Considering the risk of bleeding or perforation, endoscopic resection may not be recommended for large lesions or those with broad implantation bases. 9 In other words, when the angiolipoma has grown to a very large or obstructive lesion, surgical excision may be the best treatment. 16 Limited intestinal segment resection can be performed according to the location and obstructiveness of the tumor identified during the operation because angiolipomas are benign tumors.7,15 In addition, an excellent prognosis can be expected when the tumors are completely excised.18,27 In the present study, 18 patients had follow-up information, and none showed recurrence over the course of their different follow-up times.
Conclusion
Angiolipoma is a benign tumor, and when it occurs in the GI tract, the clinical symptoms vary. Generally, angiolipomas in the upper alimentary canal mainly present as hemorrhage, while those in the lower alimentary canal mainly present as pain and obstruction. CT and endoscopy may be the best preoperative diagnostic techniques. Biopsy can be useful but is not conclusive. Postoperative histopathologic examination is still the gold standard, while immunohistochemistry appears to be less specific. Surgical resection of the lesion is regarded as the best treatment choice, and intraoperative frozen section evaluation, if conditions permit, may be helpful to decide whether the resection should be radical or partial. Additionally, angiolipoma is a benign tumor with a good prognosis; in the cases identified, no recurrence was observed after the tumor was completely resected. Because angiolipoma of the GI tract is rare, we have herein summarized 30 cases to draw some general conclusions and thus further increase clinicians’ understanding of this disease. The findings in this report can be used to establish diagnostic and treatment guidelines.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics
The analysis was performed using anonymous clinical data that were obtained after each patient had provided written informed consent to undergo treatment. The study was approved by the Ethics Review Committee of Peking Union Medical College Hospital, Chinese Academy of Medical Science.
Funding
This work was supported by the CSCO-ROCHE Research Fund (No. Y-2019 Roche-015), the Beijing Xisike Clinical Oncology Research Foundation (No. Y-HS2019-43), and the Wu Jieping Medical Foundation (No. 320.6750.19020).