
Abstract
Objective
To explore the basic values of regional cerebral oxygen saturation (rSO2) among different age groups.
Methods
One hundred twenty patients who were scheduled for elective surgery aged 0 to 80 years (American Society of Anesthesiologists [ASA] physical status I or II) or neonates just after birth via cesarean section were enrolled and divided into the following six groups: infant (0 month and ≤12 months), toddler (>1 and ≤3 years old), preschool (>3 and ≤6 years old), school age (>6 and ≤18 years old), adult (>18 and ≤65 years old), and elderly (>65 and ≤80 years old) groups. There were 20 patients in each group.
Results
The basic values of rSO2 in infant, toddler, preschool, school age, adults, and elderly groups were 70.41% ± 4.66%, 72.43% ± 3.81%, 70.77% ± 3.27%, 70.62% ± 2.20%, 69.76% ± 6.02%, and 62.69% ± 3.14%, respectively. The basic value in the elderly group was lower compared with other five groups. There was no significant difference among infant, toddler, preschool age, school age, and adult groups.
Conclusions
The basic value of rSO2 in elderly patients is lower. Age is an important factor that affects the underlying value of rSO2.
Introduction
Regional cerebral oxygen saturation (rSO2) is a non-invasive monitoring technique that uses near-infrared spectroscopy (NIRS) to measure oxygen saturation of superficial brain cortex regions, which are among the most vulnerable to ischemic–hypoxic injury. NIRS is sensitive to hypoxia in tissues and organs. Even if the oxygenation of tissues and organs is slightly changed, such as pulse oximetry (SpO2) that is still within the normal range, the rSO2 value could be significantly changed. 1 The more obvious the decrease in rSO2, the more serious hypoxia there is in the brain tissue, which could be used to judge the prognosis. 2 A study showed that the cerebral hypoxia–ischemia threshold of rSO2 for functional impairment was 33% to 44%. 3 Yao et al. 4 reported that patients with a nadir rSO2 <35% or areas of rSO2 <40% for more than 10 minutes had significantly higher incidences of postoperative cognitive impairment. Most studies5–7 set the threshold to 50%, and they showed that rSO2 <50% is related to adverse outcomes. rSO2 monitoring could provide a bedside method that continuously and conveniently monitors “real-time” oxygen consumption, and that also monitors important tissues and organs, especially the brain, kidneys, and intestines. 8 It is, therefore, increasingly used as a complement to traditional monitoring in clinical practice especially in major surgeries that seriously affect the cerebral circulation. However, there is currently no uniform standard for its basic value, and there is no consensus on the influencing factors of the value of rSO2.
It has been reported that the rSO2 value was negatively correlated with the patient’s age, positively correlated with hemoglobin concentration, and also related to type of equipment and sensor location, but not related to patient weight, height, head size, or gender. 9 Another study found that the basic value of rSO2 was not related to patient age, gender, and body weight. 10 Therefore, the purpose of this study was to explore the basic values of rSO2 in different age groups of patients who were schedule for elective surgery and neonates who were just born after cesarean section, and to provide a reference for the clinical application of rSO2. We hypothesized that different age groups have different basic values of rSO2.
Methods
This study was registered at www.chictr.org.cn, registration number ChiCTR1800017406. The study protocol was reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University (No. 2018-10). Informed consent was provided by all enrolled patients or their relatives (legally authorized guardian). The inclusion criteria included the following: obtained informed consent from the patient or guardian; patients aged 0 to 80 years; American Society of Anesthesiologists (ASA) physical status I to II (newborn Apgar score ≥7 points); SpO2 ≥97%; and normal body temperature. The exclusion criteria including the following: mental developmental disorders; hypertension, heart disease, and diabetes; history of head injury, epilepsy, and psychosis; those with cerebrovascular disease or cranial CT or MRI showing cerebrovascular disease; history of lung infection or pulmonary insufficiency; the patient could not cooperate; or the cerebral oxygen monitoring site could not be revealed.
All patients who were scheduled for elective surgery or neonates just after birth via cesarean section were divided into six groups based on their age, as follows: infant group (0 month and ≤12 months); toddler group (>1 and ≤3 years old); preschool group (>3 and ≤6 years old); school age group (>6 and ≤18 years old); adult group (>18 and ≤65 years old); and elderly group (>65 and ≤80 years old). All the subjects were assigned to a well-ventilated and smoke-free room, and kept in a resting state for more than 15 minutes. A Somanetics INVOS 5100C (Medtronic Inc., Minneapolis, MN, USA) cerebral oxygen monitor and appropriate sensor based on the patient’s weight was applied (an adult sensor for body weight ≥40 kg, a pediatric sensor for body weight <40 kg, or a baby special sensor for infants and neonates). The sensors were placed at the right and left frontal regions, 1 cm above the patients’ eyebrows, and the edges of the sensors on both sides were 1 cm from the median line. To avoid problems that are possibly caused by ambient lighting, sensors were covered with an opaque plastic covering. The SpO2 probe was fixed on the right index finger. The average value of the rSO2 from the left and right sides was taken as the basic value. The values of rSO2, SpO2, and pulse rate (PR) at 1 minute (T1), 3 minutes (T3), and 5 minutes (T5) after starting the monitor was recorded. The hemoglobin concentrations of all subjects were obtained before the tests.
The SPSS 24.0 (IBM Corp., Armonk, NY, USA) statistical software package was used for data analysis. After the normality test and the homogeneity test of variance, the measurement data with normal distribution were expressed as the mean ± standard deviation (SD), and the q test was used for comparison between groups (S-N-Ka). The intra-group comparison was analyzed by repeated measures analysis of variance. P < 0.05 was considered to be statistically significant.
Results
The study was conducted from August to December 2018. There were 131 patients who were assessed for eligibility, and eight patients were excluded because they did not meet the study entry criteria, they refused to participate, or their hemoglobin concentration levels before the study could not be obtained, and three infants were non-cooperative. Thus, 120 patients were enrolled with 20 patients in each group, as described in Figure 1. All 120 patients completed the study. The basic hemoglobin concentration in infant, toddler, preschool, school age, adult, and elderly patient groups were 126.5 ± 10.3 (116–159) g/L, 123.5 ± 6.4 (110–138) g/L, 124.3 ± 8.5 (111–140) g/L, 125.0 ± 9.7 (113–151) g/L, 123.4 ± 10.2 (111–152) g/L, and 121.8 ± 10.0 (109–142) g/L, respectively. There was no significant difference in the hemoglobin concentration among the six groups.
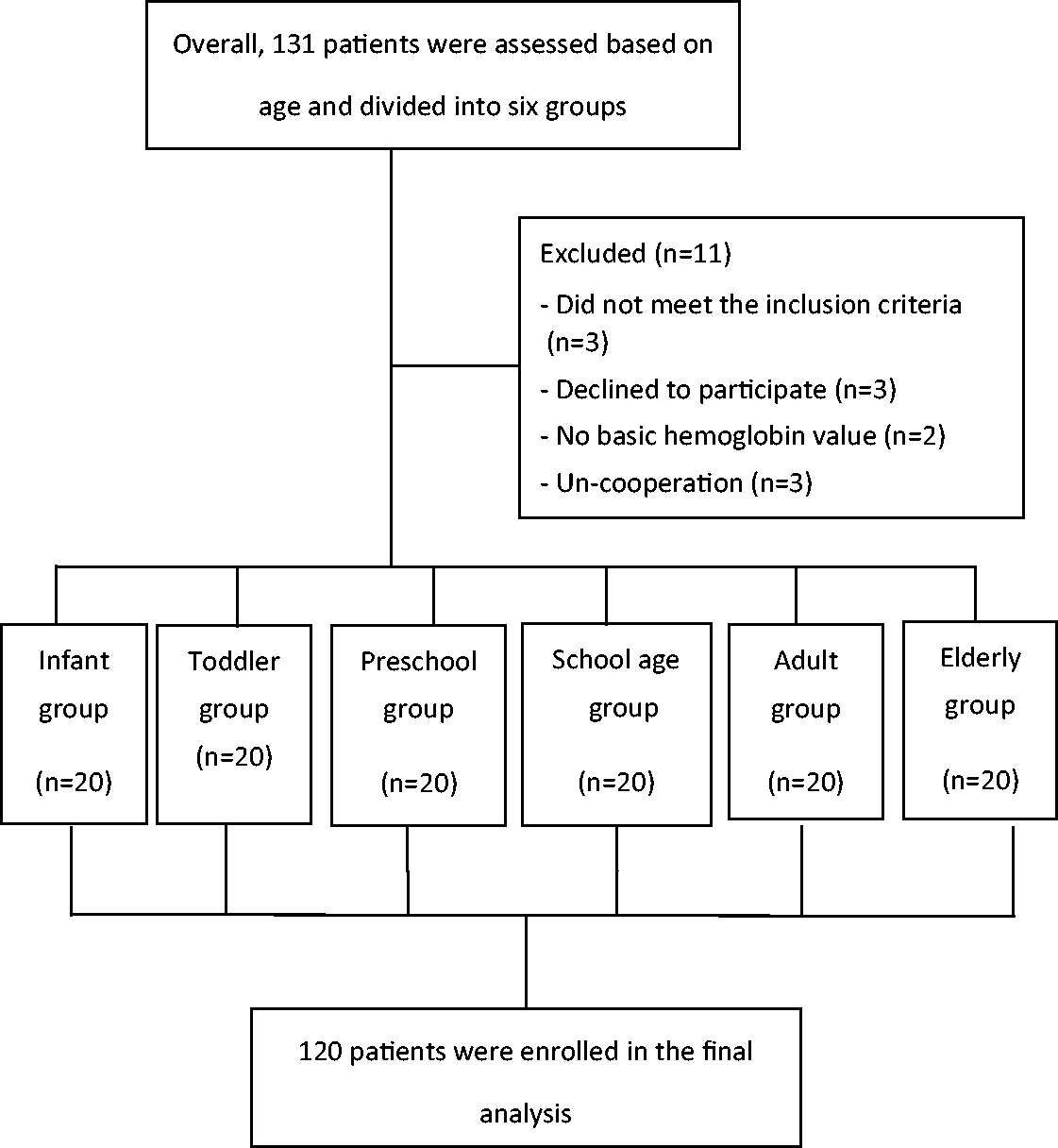
The flowchart of the study.
For each group, the values of SpO2 and PR were not significantly different at T1, T3, and T5 time points (Table 1). The values of rSO2 had wide ranges among the six groups, from 54.65% to 80.90%. The basic values of rSO2 in infant, toddler, preschool, school age, adult, and elderly patient groups were 70.41% ± 4.66%, 72.43% ± 3.81%, 70.77% ± 3.27%, 70.62% ± 2.20%, 69.76% ± 6.02%, and 62.69% ± 3.14%, respectively (Table 2). The basic value of rSO2 in the elderly group was lower compared with the other five groups (P < 0.05). There was no significant difference among infants, toddlers, preschool children, school age children, and adults. Additionally, the maximum difference of basic rSO2 value was 14.5% (62.5%–77.0%) in the infant group, 12.4% (66.6%–79.0%) in the toddler group, 13.6% (63.8%–77.4%) in the preschool group, 8.4% (65.5%–73.9%) in the school age group, 22.4% (58.5%–80.9%) in the adult group, and 16.1% (54.6%–70.7%) in the elderly group.
SpO2 and PR among six age groups at three time points.
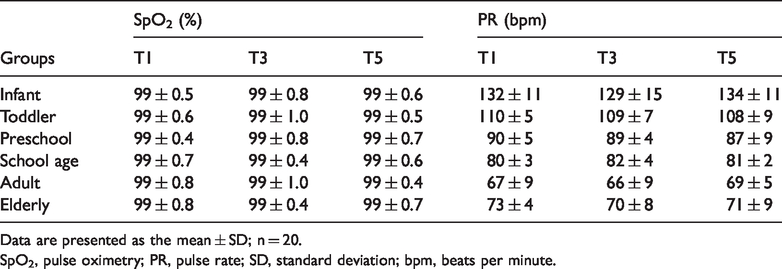
Data are presented as the mean ± SD; n = 20.
SpO2, pulse oximetry; PR, pulse rate; SD, standard deviation; bpm, beats per minute.
The values of rSO2 among six age groups at three time points.

*P < 0.05 vs. infant, toddler, preschool, school age, adult groups.
Data are presented as a percent (%, n = 20).
rSO2, regional cerebral oxygen saturation; SD, standard deviation; Min, minimum; Max, maximum.
Discussion
The main outcome of this current study was that the values of rSO2 had a wide range among the six groups, from 54.7% to 80.9%. Additionally, the basic value of rSO2 in the elderly group was lower, while there was no significant difference among other five groups.
It has been reported that when the sensor position moved 1 cm lateral from the midline, the rSO2 value was significantly reduced. 9 However, when the sensor was placed at the center of the forehead, the rSO2 value was significantly higher compared with other parts. This phenomenon is consistent with our study; when the position of the sensor was not fixed, the value of rSO2 changed rapidly. In this study, the position of the sensors was uniformly placed 1 cm above the eyebrows on both sides, and the edges of the sensors on both sides were 1 cm from the center line of the forehead. Thus, the test error caused by different devices and different sensor positions was effectively avoided.
Torella et al. 11 reported that the rSO2 value was closely related to the hemoglobin concentration, and the basic value of rSO2 increased when the hemoglobin concentration increased. Lassnigg et al. 12 demonstrated a strong correlation between cerebral oxygenation and hemoglobin concentration during hemodilution by cardiopulmonary bypass. Liem et al. 13 also reported that blood transfusion increased cerebral oxygenation in premature infants with anemia, while the opposite changes were observed during hemodilution. In this study, the hemoglobin concentration among the six groups showed no statistical difference, and thus, the interference of hemoglobin concentration on rSO2 could be eliminated. However, there are subtypes of hemoglobin. It is speculated that the content of hemoglobin subtypes may differ in different age groups, which affects the basic values of cerebral oxygen saturation in all age groups. Therefore, further research is required to confirm the effect of hemoglobin type on rSO2 values.
Currently, there is no uniform standard for the basic values of rSO2 in different age groups, and the influencing factors on the basic values of rSO2 remain unclear, although related rSO2 studies have been reported.9,10,14–17 rSO2 monitoring reflects the mixed oxygen saturation of the local brain tissue, which consists of about 70% venous blood, 20% arterial blood, and 10% capillary blood. The reference value of arterial oxygen saturation in normal people ranged from 95% to 98%, and the venous oxygen saturation ranged from 60% to 85%. Theoretically, the normal base value of rSO2 should be about 70%,18–20 which is consistent with our findings. Ružman et al. 21 showed that the mean basal values of rSO2 on the left and right sides were 71.42 ± 7.92% and 72.98 ± 7.94%, respectively, which is much closer to our results, but they did not find any correlation with age. Alderliesten et al. 22 reported that the average rSO2 in neonates was approximately 65% at admission, and it increased with gestational age (1% per week). The average basal values of rSO2 were slightly higher than our results. Increasing of age (months) and different sensors might be the reasons for the diversity of their results compared with our study. There are many commercially available NIRS devices on the market, and numerous studies23–27 have compared the differences between them. The related results showed that there were significant differences between the devices in how they respond to changes in oxygen saturation, so caution should be used when applying evidence that was generated with one manufacturer’s device to all devices. Even if the same device is used, the values measured by different probes may be different. The value measured with a neonatal probe was reported to be 10% higher compared with the adult probe. However, the monitoring probe was selected according to the manufacturer’s recommendation and common clinical practice to observe the differences in the normal basic values of rSO2 between different ages rather than to assess the value differences for using an adult probe in children or a neonatal probe in adults.
The current study showed that the basic value of rSO2 in the elderly group was lower compared with the other groups, while there was no difference among other five groups. Kishi et al. 9 measured the basic values of rSO2 in 111 patients between 7 to 89 years old under general anesthesia. The results showed that the basic values were related to the patient’s age, hemoglobin concentration, and the position of the sensors, but they were not significantly associated with the patient’s height, weight, gender, and head circumference. However, the enrolled patients were mainly limited to adults and the elderly. Our study also confirmed that the basic values of rSO2 were related to the age. A previous small-sample study by Hock et al. 28 also reported that the basic values of rSO2 were significantly correlated with age in awake subjects of different ages. The mechanisms of this correlation remain unclear. The possible explanations are suggested as follows: first, there are age-associated decreases in cerebral blood flow, cerebral blood volume, cerebral metabolic rate of oxygen, and cerebral hemoglobin oxygenation response during brain activation, and brain atrophy is gradually increased in elderly people. This leads to a decrease in brain volume and the number of brain cells and accompanies cerebrovascular degeneration, 29 which will have an important impact on the basic values, resulting in a low rSO2 value in elderly people. Second, with increasing age, the central nervous system myelin sheath is gradually prolonged (especially in the elderly), resulting in a significant extension of the length of the intracranial near-infrared light path. 30 The duration from when the rSO2 detector probe emits near-infrared light to when it receives the reflected near-infrared light is significantly prolonged and the energy attenuation is significantly increased, resulting in a decrease in the measured value of rSO2. This may be a major factor leading to the low basic values of rSO2 in elderly people. Finally, the configuration of hemoglobin changes with age, giving rise to a decrease in cerebral hemoglobin oxygenation. 31 The total amount of hemoglobin is equal to the sum of oxyhemoglobin and deoxyhemoglobin. With aging, the amount of oxyhemoglobin decreases and the amount of deoxyhemoglobin gradually increases, leading to a decline in the oxygen carrying capacity of cerebral hemoglobin, thereby decreasing the basic value of rSO2 in elderly people. However, the validity of these explanations requires further experimental evidence, and more clinical studies are warranted.
The rSO2 value is susceptible to fluctuation that is caused by external factors. One study showed that the mental state, posture, external sounds, light, and environmental ventilation conditions may have an effect on the value of rSO2. 32 Another study found that the rSO2 value was significantly increased when the subject’s brain was doing a calculation, and the value was significantly reduced when the carotid artery was lightly pressed. 33 Our study also observed that the values of rSO2 changed rapidly and the sensitivity was high. In this study, the maximum difference of basic rSO2 value was 14.5% (62.5%–77.0%) in the infant group, 12.4% (66.6%–79.0%) in the toddler group, 13.6% (63.8%–77.4%) in the preschool group, 8.4% (65.5%–73.9%) in the school age group, 22.4% (58.5%–80.9%) in the adult group, and 16.1% (54.6%–70.7%) in the elderly group. Therefore, the external conditions should be uniformly defined during the measurement of the basic rSO2 value.
There were some limitations in our study. First, although 120 ASA grade I to II patients of all ages were included in this study, this was a pilot investigation study and the sample size in our study was small. The selected subjects were also hospitalized in the same hospital, and there might have some selection bias. Thus, a large multi-center study is required to further confirm this result. Second, the Somanetics INVOS 5100C has good repeatability, but with the extension of the measurement duration, the fluctuation range of rSO2 may increase. 34 Thus, a measurement period of 5 minutes may not be long enough. Finally, the value measured using the neonatal probe is 10% higher compared with the adult probe. However, the values obtained using the same probe in different age groups were not measured, which may partially limit the clinical application of the experimental results.
In summary, this study provides the normal basic values of rSO2 under Somanetics INVOS 5100C monitoring among all age groups (from newborn to elderly). This could show whether the patient’s rSO2 value is in a reasonable range. Additionally, the baseline value of rSO2 in ASA grade I to II elderly patients (>65 and ≤80 years old) tended to be lower compared with other age groups, and there was no significant difference among the other five age groups. Thus, age is an important factor that affects the underlying rSO2 value.
Footnotes
Acknowledgements
The authors thank the Zhejiang Provincial Public Welfare Technology Application Research Foundation of China (2018ZD033).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The research was funded by Zhejiang Provincial Public Welfare Technology Application Research Foundation of China (2018ZD033).