
Abstract
A 34-year-old man presented to our hospital with a 2-month history of repeated dull upper abdominal pain. Gastroscopy and endoscopic ultrasonography indicated a hemispherical mass at the junction of the greater curvature and the gastric fundus, with hypoechogenicity originating from the intrinsic muscular layer. He was diagnosed with a gastric body submucosal lesion and gastrointestinal stromal tumor, and underwent endoscopic full-thickness resection. However, postoperative pathological examination of the mass unexpectedly revealed heterotopic spleen tissue (accessory spleen). Intragastric ectopic spleen tissue originating from the intrinsic muscular layer of the stomach is a rare clinical condition, with no specific clinical symptoms. This finding is of great clinical significance for the identification of gastric submucosal tumors.
Keywords
Introduction
The occurrence of ectopic spleen tissue includes an accessory spleen and ectopic spleen implantation. An accessory spleen includes isolated spleen tissue outside the normal spleen, usually located in the splenic hilum and the tail of the pancreas, but occasionally in the greater omentum and gastrointestinal tract. An intragastric accessory spleen is relatively rare, and is caused by failed fusion of the original spleen buds located in the dorsal mesangial membrane of the stomach during the fifth week of embryo development. 1 In contrast to a congenital accessory spleen, ectopic spleen implantation refers to autologous transplantation of spleen tissue after splenectomy, following trauma or other reasons. This occurs in 67% of patients with splenic rupture and splenectomy. 2 The location of the spleen tissue is often inconsistent with that in congenital accessory spleen, and there may be multiple sites. 3
Intragastric ectopic splenic tissues are clinically rare, and usually have no specific clinical symptoms.1,4,5 Because they can manifest as a submucosal eminence under gastroscopy, they are easily misdiagnosed as a gastrointestinal stromal tumor (GIST), which is the most common type of submucosal tumor in the stomach.
We report a case of ectopic spleen tissue originating from the intrinsic muscular layer of the stomach, with important implications for the identification of gastric submucosal tumors. It is necessary to emphasize the need to consider the possibility of heterotopic splenic tissue in patients with gastric mucosal lesions to avoid unnecessary excision and surgery.
Case report
A 34-year-old man was admitted to our hospital with a 2-month history of abdominal pain. He also had a history of alcohol consumption and had undergone splenectomy for splenic rupture more than 10 years earlier. His main symptom was repeated dull upper abdominal pain over the past 2 months, aggravated at night and relieved spontaneously. After admission, physical examination showed no positive signs. His hemoglobin was 147 g/L, his platelet count was 480 × 109/L, and other laboratory tests showed no abnormalities. Gastroscopy showed a smooth bulge on the fundus of the stomach (Figure 1), about 1.5 × 2.0 cm in size, diagnosed as gastric fundus submucosal uplift. Endoscopic ultrasonography showed a hemispherical protuberance at the junction of the greater curvature and the fundus of the stomach, with a size of about 2.0 × 2.0 cm. Ultrasound revealed a hypoechoic, oval-like lesion, with uniform internal echo, a section size of about 1.8 × 1.2 cm (Figure 2), and a clear boundary, originating from the intrinsic muscle layer.

A bulge at the bottom of the stomach under gastroscopy, measuring about 1.5 × 2.0 cm in size, with a smooth surface.
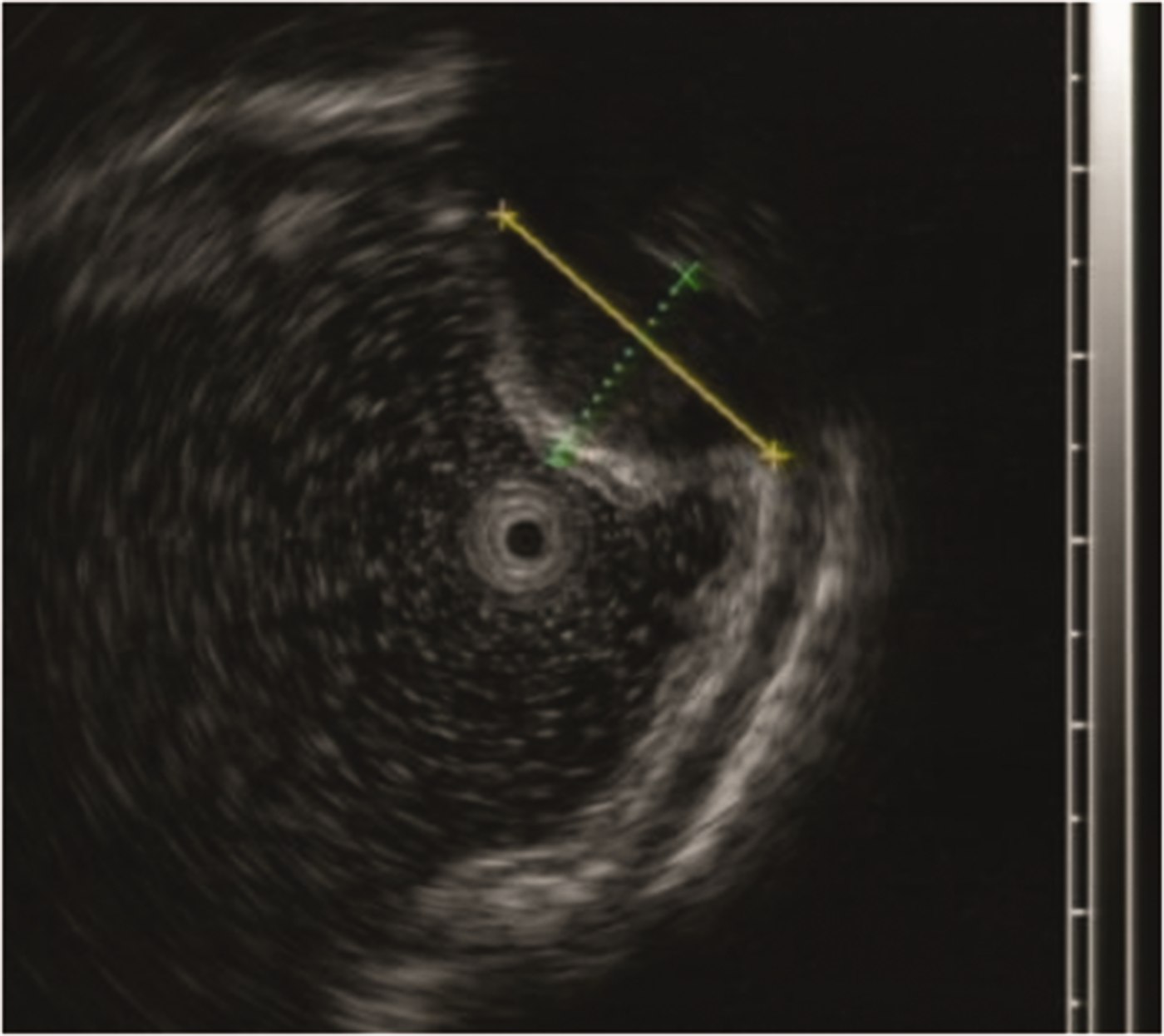
The focus was hypoechoic and oval-like, with a uniform internal echo. The section was about 1.8 × 1.2 cm in size, and the boundary was clear. The lesion originated from the intrinsic muscle layer.
The submucosal lesion was diagnosed as a GIST, and endoscopic full-thickness resection was successfully performed. However, postoperative pathology showed that the tissue was mainly composed of lymphocyte nodules surrounded by sinusoids containing red blood cells. The histological structure was consistent with an accessory spleen (Figure 3). The immunohistochemical results were as follows: CD117(−), CD34(+), CK(−), Desmin(−), Dog-1(−), Ki-67(10%), S-100(−), SMA(+), CD31(+), CD45(partial+), and Vim(+).

The tissue was mainly composed of lymphocyte nodules and surrounded with sinusoids containing red blood cells. The histological structure was consistent with that of an accessory spleen. Hematoxylin–eosin staining, magnification ×200.
All of the examinations described in this article were performed for medical purposes. The patient’s information was kept strictly confidential during the study. Written informed consent was obtained from the patient for publication of this case report and the accompanying images.
Discussion
GISTs can occur in any part of the stomach, but are usually located in the body and antrum of the stomach. They present as single lesions with or without a capsule, and can be >10 cm in diameter. The tumor can show ischemic necrosis and calcification, and the surface can form erosions and ulcers. Under ultrasonic endoscopy, the lesions are generally hypoechoic, with high or medium-low echo, even internal or uneven echo, or liquefying area and calcification, mostly round, fusiform, or lobulated, with clear boundaries, and most originate from the intrinsic muscle layer.
Heterotopic spleen tissue is usually located in the gastric fundus and appears round or oval. Ultrasonic endoscopy reveals a mostly hypoechoic or hyperechoic focus, often similar to the echo intensity of the spleen. 6 Its internal echo is uniform and its boundary is clear. It may originate from the intrinsic muscle layer, serous layer and the outside of the cavity and close to the stomach wall.
An accessory spleen is usually found incidentally in most patients with the condition, and has no clinical significance.7,8 However, they may occasionally be clinically important, e.g., if an accessory spleen in a certain location resembles certain tumors, such as GIST and pancreatic tumors. In addition, splenectomy may cause secondary splenic hyperplasia, leading to the recurrence of hematological diseases. It is therefore important to distinguish between an accessory spleen and gastric submucosal or abdominal visceral tumors.9,10
The endoscopic ultrasound features of intragastric ectopic splenic tissues and GIST are very similar, such as in the current case in which homogeneous hypoechoic lesions originated from the intrinsic myometrium. These conditions can therefore be easily misdiagnosed based on ultrasound endoscopy findings, and it is important to also consider the patient’s clinical history. It has been reported3,6 that ectopic spleen tissue may be prone to appear in the gastric fundus, and this possibility should therefore be considered in patients with a history of spleen trauma or splenectomy, with homogeneous hypoechoic lesions in the fundus of the stomach originating from a serous layer or out of the cavity. The diagnosis can be clarified by fine needle aspiration or technetium99m isotope imaging to avoid unnecessary endoscopic treatment or surgery.
Splenosis is a rare disease involving the implantation of heterotopic splenic tissue, usually after splenic trauma or resection, causing part of the spleen to fall off and become embedded in other parts of the body. Splenosis can therefore occur in any place where diffuse spleen tissue can be implanted. The clinical manifestation is single or multiple round masses. 11 While an accessory spleen is functionally and histologically similar to normal spleen tissue, splenosis tissue lacks key splenic features, such as a thick capsule, smooth muscle component, and splenic arterial blood supply. 12 In the current case, although the heterotopic splenic tissue was derived from the intrinsic muscular layer of the stomach, it was more consistent with the characteristics of an accessory spleen, and the patient’s history of splenectomy due to traumatic rupture of the spleen >10 years ago meant that we could not completely rule out the possibility of splenosis. Clinicians must therefore keep in mind the possibility of splenosis in patients presenting after splenic trauma.