
Abstract
Microvascular decompression (MVD) is an effective and safe approach for treating hemifacial spasm (HFS). Postoperative complications may include facial nerve palsy, hearing loss, intracerebral haematoma, and brainstem infarction. The occurrence of intracranial cyst following MVD is extremely rare, with few cases documented in the literature. Herein, the cases of two patients with HFS who developed ipsilateral cerebellar cyst following MVD are reported. The first patient was a 50-year-old male presenting with a 6-year history of HFS on the right side of his face. MVD was performed, and 12 days postoperatively he developed dizziness and nausea. Magnetic resonance imaging (MRI) showed a cyst in the ipsilateral cerebellum. Antibiotic treatment provided no benefit, and the cyst was drained. The second patient was a 44-year-old female presenting with a 4-year history of HFS on the right side of her face. MVD was performed, and 18 days following surgery, she developed dizziness and nausea. MRI showed an ipsilateral cerebellar cyst. Conservative treatment was applied and the cyst shrunk. At the 2-month follow-up appointment, symptoms were completely resolved in both patients. Cerebellar cyst is a rare complication following MVD. Timely diagnosis and appropriate treatment should be emphasized, and surgical treatment may be unnecessary.
Introduction
Hemifacial spasm (HFS) refers to a neuromuscular disorder characterized by irregular, involuntary unilateral muscle contractions.1,2 HFS is caused by vascular compression of the VIII cranial nerve, and typically starts in the periorbital area, subsequently progressing inferiorly to the cheek, mouth, and neck. 2 Microvascular decompression (MVD) has been widely used to treat a variety of neurovascular compression syndromes, including HFS, trigeminal neuralgia, glossopharyngeal neuralgia, intractable tinnitus, and intractable hiccups.3–6 MVD of the facial nerve is proven to be an effective and safe approach for treating HFS, and the most common postoperative complications associated with this procedure include facial nerve palsy, hearing loss, intracerebral haematoma, and brainstem infarction.7,8 Iatrogenic intracranial cyst secondary to MVD is extremely rare, with only limited cases documented in the literature.9–12 Moreover, to the best of the present authors’ knowledge, an intracranial cyst occurring in the cerebellar hemisphere following MVD has not been described previously.
Herein, two cases of HFS, in which a cerebellar cyst developed after MVD, are reported. The clinical and radiological profiles are presented, and relevant pathogenesis is discussed. Published literature regarding brain cysts following MVD is then reviewed.
Case reports
The Ethics Committee of The First Hospital of Jilin University provided written consent to publish these case reports, and verbal informed consent was provided by the patients.
Case 1
A 50-year-old male presented at the First Hospital of Jilin University, Changchun, China in November 2015 with a 6-year history of intermittent, involuntary muscle contractions on the right side of his face. The spasms were aggravated in stressful situations and alleviated in relaxed situations. Oral carbamazepine had been prescribed by local practitioners, and although the spasms were partially relieved in the initial days, the symptoms returned again later. An injection of botulinum toxin was administered to the facial muscles, but this provided no benefit. After referral to the First Hospital of Jilin University, neurological examination revealed unilateral, involuntary, paroxysmal contractions of the facial muscles, which were exacerbated during facial activities such as smiling, speaking, blinking, and opening the mouth. Ophthalmological and otological examinations were all normal. Magnetic resonance imaging (MRI) was performed using a Philips Intera 1.5T MRI system, and axial images yielded normal results (Figure 1a and b). The patient was diagnosed with HFS, and MVD was scheduled.

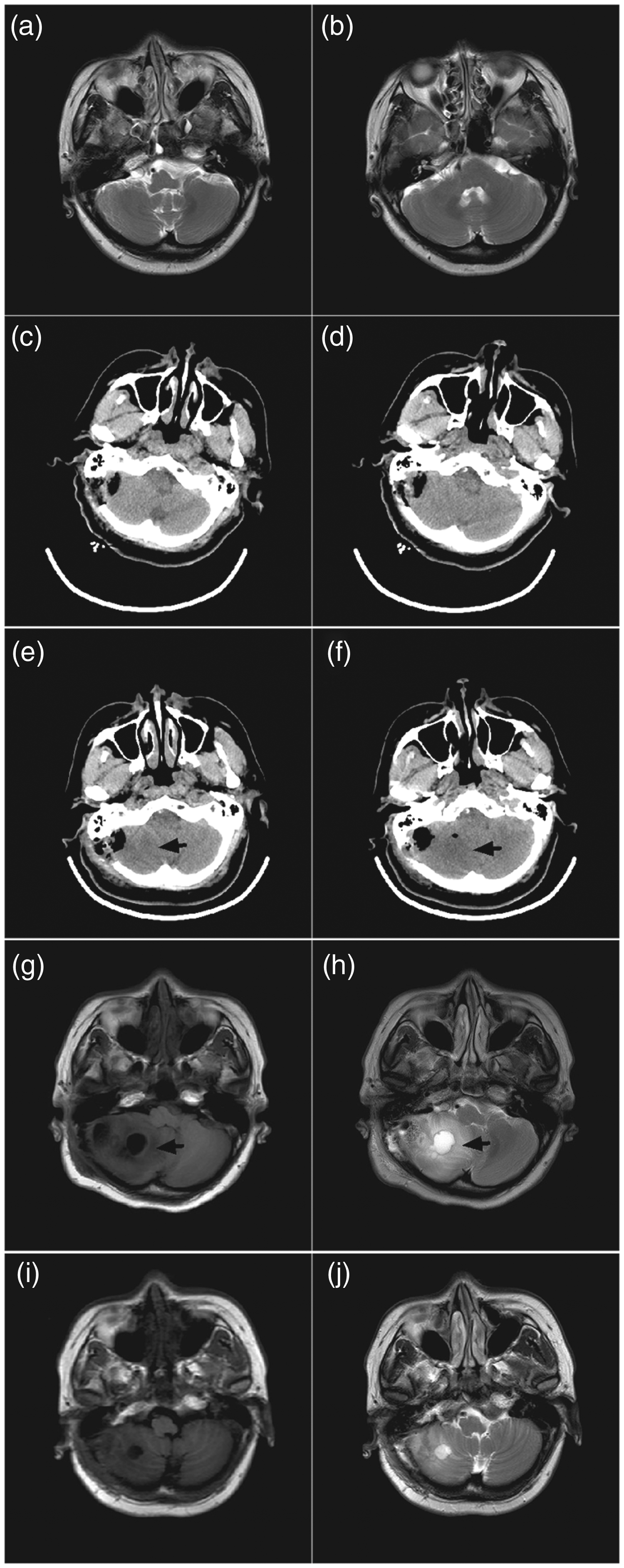
Representative radiological images from a 50-year-old male patient with hemifacial spasm (Case 1): (a) T2-weighted and (b) T1-weighted axial magnetic resonance imaging (MRI) results, obtained on hospital admission, showing normal features; (c and d) head computed tomography (CT) scan images, obtained following microvascular decompression (MVD), showing normal features, excluding postoperative haemorrhage or hydrocephalus; (e) axial and (f) coronal plane contrasted MRI T1-weighted images, obtained at 12 days following MVD, showing a round, cystic lesion measuring 3.1 cm × 2.2 cm × 2.7 cm in the right cerebellum with ring-shaped enhancement (arrow); (g and h) head CT scan images, obtained following cyst drainage surgery, showing drainage tube placement (arrow) in the cerebellar cyst and shrunken cyst; (i) axial and (j) coronal T1-weighted MRI images obtained at 45 days following MVD surgery, showing a shrunken cyst in the right cerebellum.
A craniotomy was performed via the retromastoid suboccipital approach under general intravenous anaesthesia. Induction of anaesthesia comprised single doses of each of the following: 42 mg rocuronium bromide, 140 mg propofol, 0.2 mg fentanyl, and 2 mg midazolam. Anaesthesia was maintained using 1 050 mg propofol, continuous pumping, 2.5 h; and 0.1 mg fentanyl, single dose per 0.5 h. Intraoperatively, the root exit zone of the right facial nerve was found to be compressed by the ipsilateral anterior inferior cerebellar artery (AICA). Teflon was interposed to separate the facial nerve from the AICA and intraoperative electrophysiological monitoring showed that the abnormal facial nerve responses disappeared. The ipsilateral cerebellar hemisphere remained intact, and the dura mater was closed. Postoperative analgesia comprised 0.05 mg fentanyl, single dose at 4 h following surgery in the case of pain visual analogue scale (VAS) score >4. The postoperative period was uneventful, and no immediate complication was noted. The HFS symptoms were completely resolved. Postoperative head computed tomography (CT) scanning (Philips Brilliance CT scanner) was normal, excluding postoperative haemorrhage or hydrocephalus (Figure 1c and d).
At 12 days following surgery, the patient developed serious dizziness and nausea without vomiting. His temperature was normal. MRI revealed a round, cystic lesion of 3.1 cm × 2.2 cm × 2.7 cm in the right cerebellum with ring-shaped enhancement (Figure 1e and f), and an intracerebellar abscess was suspected. After 10 days of antibiotic treatment with 4 g ceftriaxone, intravenous drip, once daily, the cystic lesion showed no significant change. Reoperation was performed via the original incision. The cyst was punctured, yielding a faint yellow liquid mimicking cerebrospinal fluid; no pus was noted. A drainage tube was then placed in the cerebellar cyst. Postoperative CT scanning showed that the cyst had reduced in size (Figure 1g and h), and the drainage tube was removed 3 days after surgery. Brain MRI at 45 days following MVD surgery demonstrated a shrunken cyst in the right cerebellum (Figure 1i and j). At the 2-month follow-up appointment, the patient was asymptomatic.
Case 2
A 44-year-old female presented at the First Hospital of Jilin University, Changchun, China in February 2017 with a 4-year history of involuntary muscle contractions on the right side of her face. Oral carbamazepine (200 mg, twice daily) was prescribed by local practitioners, however, no significant benefit was noted, and the patient then refused to continue taking oral carbamazepine. Treatment with botulinum toxin injected into the facial muscles was then recommended by local practitioners, and was initially effective, but the beneficial effects disappeared after 4 months. The patient then refused to continue with injected botulinum toxin treatment. MRI analysis performed at hospital admission revealed a normal result (Figure 2a and b). The patient was diagnosed with HFS, which was treated using MVD.
Representative radiological images from a 44-year-old female patient with hemifacial spasm (Case 2): (a and b) T2-weighted axial magnetic resonance imaging (MRI) results, obtained on hospital admission, showing normal features; (c and d) head computed tomography (CT) images following microvascular decompression (MVD) showing no postoperative haemorrhage or hydrocephalus; (e and f) CT images at 18 days following MVD showing low density (arrow) in the right cerebellum; (g) axial T1-weighted contrasted MRI image showing hypointense region (arrow) and (h) axial T2-weighted contrasted MRI image showing hyperintense region (arrow), both captured at 18 days following MVD, revealing a round, cystic lesion with a diameter of 2.7 cm (arrow) in the right cerebellum; and (i) axial T1-weighted image and (j) axial T2-weighted image from MRI performed at 1 month following readmission, revealing a shrunken cyst in the right cerebellum.
Craniotomy was performed via the retromastoid suboccipital approach, under general intravenous anaesthesia, which was induced using single doses of each of the following: 30 mg rocuronium bromide, 100 mg propofol, 0.2 mg fentanyl, and 2 mg midazolam. Anaesthesia was maintained with 750 mg propofol, continuous pumping, 2.6 h; and 0.1 mg fentanyl, single dose per 0.5 h. The root exit zone of the right facial nerve was observed to be compressed by the ipsilateral posterior inferior cerebellar artery (PICA). Teflon was interposed to separate the facial nerve from the PICA, and intraoperative electrophysiological monitoring showed disappearance of the abnormal facial nerve responses. The ipsilateral cerebellar hemisphere remained intact, and the dura mater was sutured. Postoperative analgesia comprised 0.05 mg fentanyl, single dose at 4 h following surgery in the case of a pain VAS score > 4. The postoperative course was uneventful, and the HFS symptoms were relieved. Postoperative head CT scanning showed no postoperative haemorrhage or hydrocephalus (Figure 2c and d).
At 18 days following surgery, the patient developed severe dizziness and nausea without vomiting. Her temperature was normal. CT demonstrated local hypodensity in the right cerebellum (Figure 2e and f). MRI revealed a round, cystic lesion with a diameter of 2.7 cm in the right cerebellum, which was hypointense on T1-weighted imaging (Figure 2g) and fluid attenuated inversion recovery (FLAIR) imaging and hyperintense on T2-weighted imaging (Figure 2h). Cerebellar cyst was diagnosed, and the lesion was conservatively treated with 50 g mannitol, by intravenous drip every 12 h. Ten days later, the symptoms gradually improved. One month following readmission, MRI revealed a shrunken cyst in the right cerebellum (Figure 2i and j). At the 2-month follow-up appointment, the symptoms were completely resolved.
Discussion
Intracranial cyst formation is a rare complication of MVD procedures. The PubMed and Web of Science databases were searched from inception to May 2017 for relevant studies regarding this uncommon condition, using the keywords and subject terms: ‘cyst’ or ‘complication’ in combination with ‘microvascular decompression’. The search yielded four reports describing cyst formation following MVD,9–12 and the studies involved a total of five patients (one male and four females), with a mean age of 54.4 years (range, 48–62 years; Table 1). The primary diseases requiring treatment by MVD in these previously published studies were all trigeminal neuralgia.9–12 The clinical presentation of secondary intracranial cysts included brainstem symptoms (2/5, 40%) and trigeminal neuralgia recurrence (3/5, 60%). Cyst locations included the brainstem (2/5, 40%) and the ipsilateral cerebellopontine angle (3/5, 60%). In all of the published cases, surgical drainage of the cyst was adopted as treatment, and the surgical outcomes were all favourable.9–12
Clinical features of patients with secondary intracranial cyst following microvascular decompression.
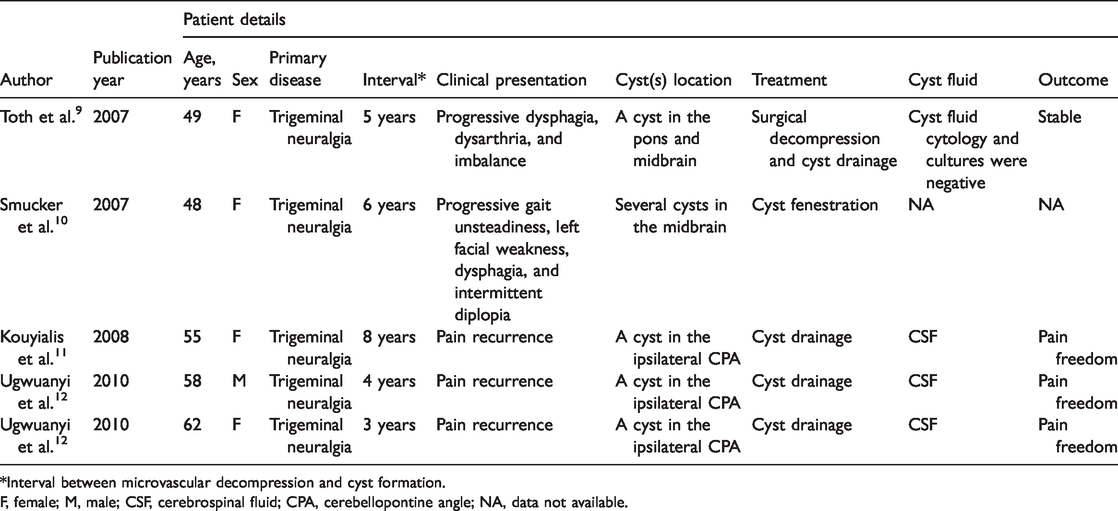
*Interval between microvascular decompression and cyst formation.
F, female; M, male; CSF, cerebrospinal fluid; CPA, cerebellopontine angle; NA, data not available.
To the best of the present authors’ knowledge, several features of the current patients were unique and have not been previously described: (a) the primary disease was HFS, and MVD was performed; (b) secondary intracranial cyst formation occurred in the ipsilateral cerebellar hemisphere; and (c) one of the patients was treated with a conservative strategy, and this yielded a favourable outcome.
A cerebellar cyst is an uncommon entity, which is most frequently congenital;13,14 those developing after cerebellar parenchyma injuries or iatrogenic interventions are extremely rare.15,16 Following review of the operative videos in the present cases, and comparison of differences with other cases, the two patients were found to have common surgery-related characteristics. In the present cases, the operation involved over-retraction of the cerebellum before sufficient arachnoid opening. In cases without this operative feature, the patients did not present with cysts. Thus, over-retraction of the cerebellum without sufficient opening of the arachnoid might be the reason for the cysts, which may be a sequela to cerebellar over-retraction. The definitive pathogenetic mechanism of secondary cyst formation remains unknown. Sharif et al. 16 hypothesized that the cyst may originate from a dural defect or a small arachnoidal/parenchymal tear during MVD surgery, and the tear may act as a unidirectional valve to permit cerebrospinal fluid accumulation. However, in the present patients, all the surgical procedures were performed outside of the cerebellar parenchyma, and the cerebellar hemisphere was confirmed to be intact before the dura mater was closed. Notably, the patient reported by Sharif et al. 16 had a previous history of high-dose radiation on the cerebellum, and previous studies have found that brain radiation therapy may cause intracranial cysts. 17 Additionally, Teflon has been proposed as a cause of intracranial cyst following MVD. 10
The exact diagnosis of a secondary cerebellar cyst is challenging, as it can be easily mistaken for more common entities occurring in this site. 18 Taking a detailed history and close radiological observation may facilitate the diagnosis. Most cerebellar cysts are benign non-neoplastic lesions, 18 but some cerebellar cysts may be associated with ganglioglioma. 19 A differential diagnosis should include cystic tumours, such as pilocytic astrocytoma, ganglioglioma, hemangioblastoma, and medulloblastoma. As the present patients had a history of MVD, a preliminary diagnosis of postoperative cerebellar abscess was also suspected; however, antibiotic treatment in case 1 provided no benefit and no pus was noted during the second operation, which excluded this suspected diagnosis.
The optimal therapeutic strategy for secondary cerebellar cysts following MVD has not been outlined. Surgical resection of the cyst may be an effective approach for relieving the compression symptoms. In case 2 of the present report, a conservative treatment strategy was attempted, and the cerebellar cyst was gradually absorbed, indicating that surgical intervention may be not necessary in some patients with good general conditions. Due to the low morbidity of this rare complication, more research is needed.
In conclusion, a cerebellar cyst is an infrequent complication following MVD. Clinicians should be aware of this rare condition, and early diagnosis and appropriate treatment should be highlighted. Surgical treatment can be effective but may not be necessary for this rare complication.
Footnotes
Acknowledgements
This manuscript has been edited and proofread by Medjaden Bioscience Limited.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.