
Abstract
Objective
To investigate the practicality of a new method using anatomical spaces for performing standard laparoscopic radical hysterectomy (LRH) without ureteral injury in patients with cervical cancer.
Methods
Clinicopathological characteristics and perioperative complications were retrospectively analysed in 440 patients with stages IB1 to IIB cervical cancer. The patients were assigned to two of the following groups: LRH by our method of using anatomical landmarks (anatomical space group, n = 217) and the traditional method (traditional group, n = 223).
Results
The mean operative duration and time of vesicouterine ligament (VUL) dissection were significantly shorter (173.87 ± 30.39 vs. 210.83 ± 44.55 minutes; 32.75 ± 7.23 vs. 43.48 ± 11.22 minutes), and blood loss was less in the anatomical space group compared with the traditional group. The rate of the intraoperative complication of ureteral injury was also significantly lower in the anatomical space group compared with the traditional group (0 vs. 5).
Conclusions
LRH by the anatomical method, using the axillary space and other potential spaces as anatomical landmarks, results in less blood loss and reduced ureteral injury compared with the traditional method. This method is safe and practical for separating the ureter from the VUL in patients with cervical cancer.
Keywords
Introduction
Cervical cancer is the fourth most common cancer among women in the United States, with an estimated 61,880 new cases and 12,160 deaths in 2019. 1 The advanced stage of cervical cancer has a relatively high prevalence in China. Currently, radical hysterectomy combined with pelvic lymphadenectomy is the primary therapy for early-stage cervical cancer. 2 The first radical hysterectomy with laparoscopic pelvic and para-aortic lymphadenectomy was performed in 1989 by Nezhat et al. 3 and this procedure was published in 1992. Type C is an enlarged hysterectomy, as described by Querleu and Morrow, and is performed in patients with stages IB1, IB2, IB3, and IIA cervical cancer, according to the classification by the International Federation of Gynecology and Obstetrics (FIGO 2018). 4 Minimally invasive approaches for radical hysterectomy have gained popularity over the last decade in the treatment of cervical cancer. However, the complex anatomy of the plexus encompassing the parametrial tissue renders its separation technically challenging.
The vesicouterine ligament (VUL) is composed of the anterior leaf and posterior leaf. In the anterior leaf of the VUL, the cervicovesical blood vessels are the main vascular bundles. In the posterior leaf, the middle vesical vein and inferior vesical vein draining into the deep uterine vein run from the urinary bladder to the lower cervix or vagina. There are vascular communicating branches of the middle vesical and inferior vesical veins, which have no regular pathways. Identification of these vessels is important for performing dissection of the VUL to ensure safe outcomes of laparoscopic radical hysterectomy (LRH). However, comprehensive understanding of the anatomy and management of the vascular plexus in the VUL are difficult. Management of bleeding from the venous communicating branch of the VUL is also difficult.
Many researchers have attempted to find a practical and safe procedure for clinical application of radical hysterectomy. Yabuki et al. 5 , 6 and Fujii et al. 7 focussed on description of the anatomy of the VUL. However, precise anatomy of the veins remains to be determined and there is no consensus on the optimal landmarks. Knowledge of the precise anatomy is important for surgical treatment of cervical cancer. Four anatomical spaces associated with the VUL are the paravesical space, 8 the paravaginal space, 9 the fourth space of Yabuki, 5 and the “axillary space”. We propose naming the axillary space as the entrance of the ureteral space, which is inferior to the uterine artery, between the ureter and lower cervix. The aim of exposing the axillary space is to separate the ureteral space. The fourth space of Yabuki is also important, which is a loose and avascular area in the anterior lateral aspect of the ureterovesical junction. This space is the area of insertion of the ureter into the bladder. The paravaginal space is located medial to the posterior leaf of the VUL and lateral to the vagina, while the paravesical space is the lateral margin of the posterior leaf of the VUL.
The present study aimed to investigate a feasible dissection method, using the axillary space and other potential spaces as landmarks, under laparoscopy. The ureteral spaces were developed to reduce the amount of blood loss and prevent ureteral injury. The practicality and safety of this approach were investigated by comparing the outcomes with those of the traditional method.
Materials and methods
The Ethics Committee of International Peace Maternity and Child Health Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, China approved the present study. The requirement for informed consent was waived because of the retrospective nature of the study.
Patients
Patients with cervical cancer underwent Type C LRH and pelvic lymphadenectomy at the International Peace Maternity and Child Health Hospital in Shanghai between August 2014 and October 2019. One group of patients (anatomical space group) (FIGO 2018 stages: IB1, 97; IB2, 66; IB3, 29; IIA1, 19; IIB, 6) underwent LRH by an anatomical space dissection technique by surgeon A. In this method, the axillary space, the fourth space of Yabuki, and the paravesical space along with the paravaginal space were used as landmarks. The second group included patients (FIGO 2018 stages: IB1, 101; IB2, 75; IB3, 24; IIA1, 23; IIB, 0) who underwent LRH by the traditional method (traditional group) by surgeon B. Surgeons A and B had the same surgical experience. Patients with stages IB3 and IIB who refused radiotherapy underwent LRH.
This study was a single-centre retrospective cohort study. Data of the operative duration, time of VUL dissection, estimated blood loss, and perioperative morbidities, especially ureteral injury, were recorded. The operative time was recorded from the beginning of the skin incision to completion of operative wound closure. The time of the VUL dissection ranged from ligation of the uterine artery to transection of the posterior leaf of the VUL. Blood loss was recorded at two time points during separation of the VUL and after removal of the uterus. Blood loss was estimated from the amount collected in a suction device. Complications were defined as any event that required an additional surgical procedure and rehabilitation therapy. Ureteral injury was defined as either implantation of a ureteral stent during the operation or obstruction, ligation, transection, crushing, stretching, and thermal injury of the ureter.
We used the cumulative sum analytical method, which is similar to that described by Bokhari et al. 10 The cumulative sum method is the running cumulative sum of differences between measured individual values and the target. The mean operative time for each surgeon was considered as the target. We used the decision interval of 4 standard deviations and a reference value of 0.5. The learning curve was evaluated for surgeons A and B.
LRH
The traditional method of LRH involved blind separation of the ureter from the parametrial tissue along the ureteral course. To divide the anterior leaf of the VUL, an ultrasonic knife was insinuated into the ureteral space by pushing the ureter laterally from the cervix. Injury to the vessels running near the ureter can occur when blind placement of the instrument fails to identify the vascular bundles. During treatment of the posterior leaf of the VUL, a connective tissue triangle was created by the upper vagina/cervix and the ureter draining into the bladder. In this triangle, an avascular loose connective tissue plane was developed avoiding bundles of the upper vagina. An ultrasonic knife in this space was used to penetrate the loose connective tissue of the posterior leaf of the VUL. A considerable amount of blood loss may ensue in cases of injury to these blood vessels.
Operative procedure for determining anatomy of the VUL
Only the operative steps necessary to determine the anatomy of the VUL have been described.
Step I: Surgical anatomy of the anterior leaf of the VUL
After separating the uterine artery and superficial uterine vein from the ureter, the uterine artery was unroofed to the uterine side and the ureter was lifted outward with a grasper. Subsequently, the axillary space was exposed. The axillary space is inferior to the uterine artery, between the ureter and lower cervix, which is the entrance of the ureteral space.
The bladder was separated completely from the cervix down to the level of the trigone and then the fourth space of Yabuki 5 was separated, which is the insertion point of the ureter into the bladder and the terminal part of the ureteral space (Figure 1). The ureteral space, which is beneath the anterior leaf (upper side) and above the posterior leaf (bottom side) of the VUL, is actually a potential avascular space along the medial side of the ureter and the lateral side of the lower cervix or vaginal wall. Between the axillary space and the fourth space of Yabuki, several small blood vessels in the anterior aspect of the VUL that cross over the ureteral space were managed by developing several vertical shafts, called Karez, into the ureteral space (Figure 2). Subsequently, coagulation and transection of the small blood vessels were performed with an ultrasonic knife (Figure 3).

Schematic diagram of the ureteral space beneath the anterior leaf of the vesicouterine ligament. (a) The axillary space (initial part of the ureteral space); (b) the fourth space of Yabuki (terminal part of the ureteral space); and (c) the ureteral space.

Schematic diagram of Karez in the anterior leaf of the vesicouterine ligament. (a) The axillary space (initial part of the ureteral space) and (d) Karez (vertical shafts, which are avascular spaces between vessels and vessels).

Schematic diagram of the ureteral space between the ureter and the cervix/upper vagina. (a) The axillary space (initial part of the ureteral space); (b) the fourth space of Yabuki (terminal part of the ureteral space); and (c) the ureteral space.
Step II: Surgical anatomy of the posterior leaf of the VUL
The posterior leaf of the VUL is abundant in vascular bundles between the paravesical space and paravaginal space (Figure 4). After developing the paravesical space (lateral margin of the posterior leaf of the VUL) and paravaginal space (medial margin of the posterior leaf of the VUL), we coagulated and transected the whole posterior leaf with Ligasure (Covidien, Boulder, CO, USA). The bladder and ureter were completely separated from the lower cervix and upper vaginal wall (Supplementary video).
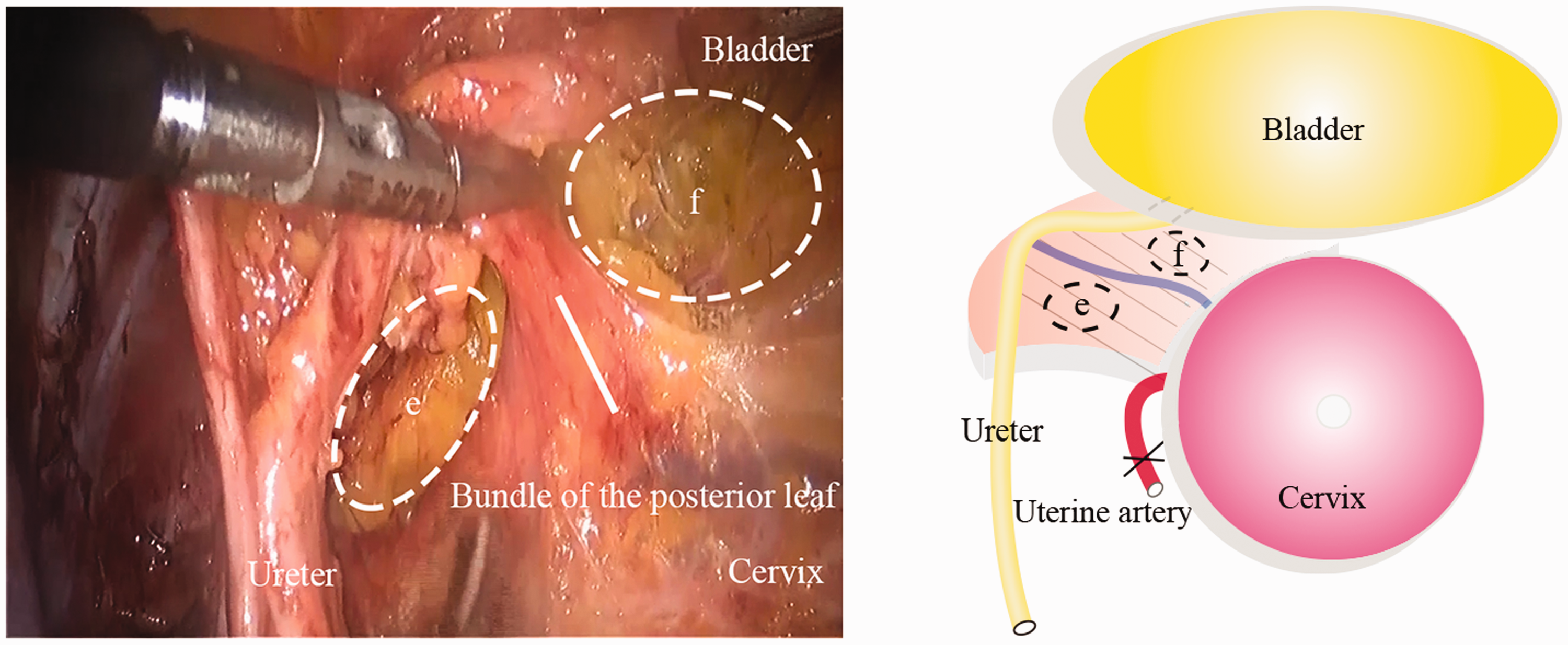
Schematic diagram of anatomical spaces in the posterior leaf of the vesicouterine ligament. The posterior leaf of the vesicouterine ligament incorporating vascular bundles between the paravesical space (e) and paravaginal space (f) is managed by Ligasure. (e) The paravesical space (lateral margin of the posterior leaf of the vesicouterine ligament) and (f) the paravaginal space (medial margin of the posterior leaf of the vesicouterine ligament).
Statistical analysis
Data are shown as mean ± standard deviation. Comparisons were performed using the unpaired Student’s t-test for normally distributed continuous variables and the Mann–Whitney U test for non-normally distributed variables. The chi-square test was used to compare categorical data. Regression analysis was used to analyse the relations of the operation time and different methods. Statistical analyses were performed using IBM SPSS Statistics version 19.0 (IBM Corp., Armonk, NY, USA). P < 0.05 was considered statistically significant. Analyses for the cumulative sum method were performed using R 3.6.2 software with package ‘qcc’ (https://cran.r-project.org/web/packages/qcc/index.html).
Results
General information of the patients
A total of 440 patients were included in the study. Of them, 217 patients underwent LRH by the anatomical space method by surgeon A and 223 patients underwent LRH by the traditional method by surgeon B. There were no significant differences in the patients’ characteristics between the groups. The clinical and pathological characteristics of the two groups are shown in Table 1.
Clinical and pathological characteristics.

Values are mean ± standard deviation or number.FIGO, International Federation of Gynecology and Obstetrics; RCTX, radiochemotherapy.
Comparison of the intraoperative and postoperative outcomes
LRH was completed successfully and was conducted safely in all patients. There were no morbidities associated with a transfusion requirement or ureteral or bladder injury. Table 2 shows the intraoperative and postoperative outcomes of both groups. The mean operative duration and time of VUL dissection in the anatomical space group were significantly shorter than those in the traditional group (both P < 0.01). Blood loss during separation of the VUL and after LRH in the anatomical space group was significantly less than that in the traditional group (both P < 0.01). The rate of the intraoperative complication of ureteral injury was significantly lower in the anatomical space group than in the traditional group (P = 0.03).
Intraoperative and postoperative outcomes.

Values are mean ± standard deviation or number. VUL, vesicouterine ligament.
Supplementary Video: Video shows the anatomical space method for dissection of the vesicouterine ligament in laparoscopic radical hysterectomy.
Analysis of learning curves
For the subgroup of stage IB1 in the first 50 cases, regression analysis showed that the operative time steeply decreased in the anatomical space group with surgery performed by surgeon A (β coefficient = −1.1160). However, surgeon B who performed the traditional method, showed a gentle slope in the learning curve (β coefficient = −0.5188) (Figure 5a). Nonetheless, some variations in the learning process were observed. Surgeon A required approximately 24 cases to achieve surgical proficiency of the anatomical space method. The learning curves for LRH using cumulative sum charts are shown for surgeon A using the anatomical space method (Figure 5b) and surgeon B using the traditional method (Figure 5c).
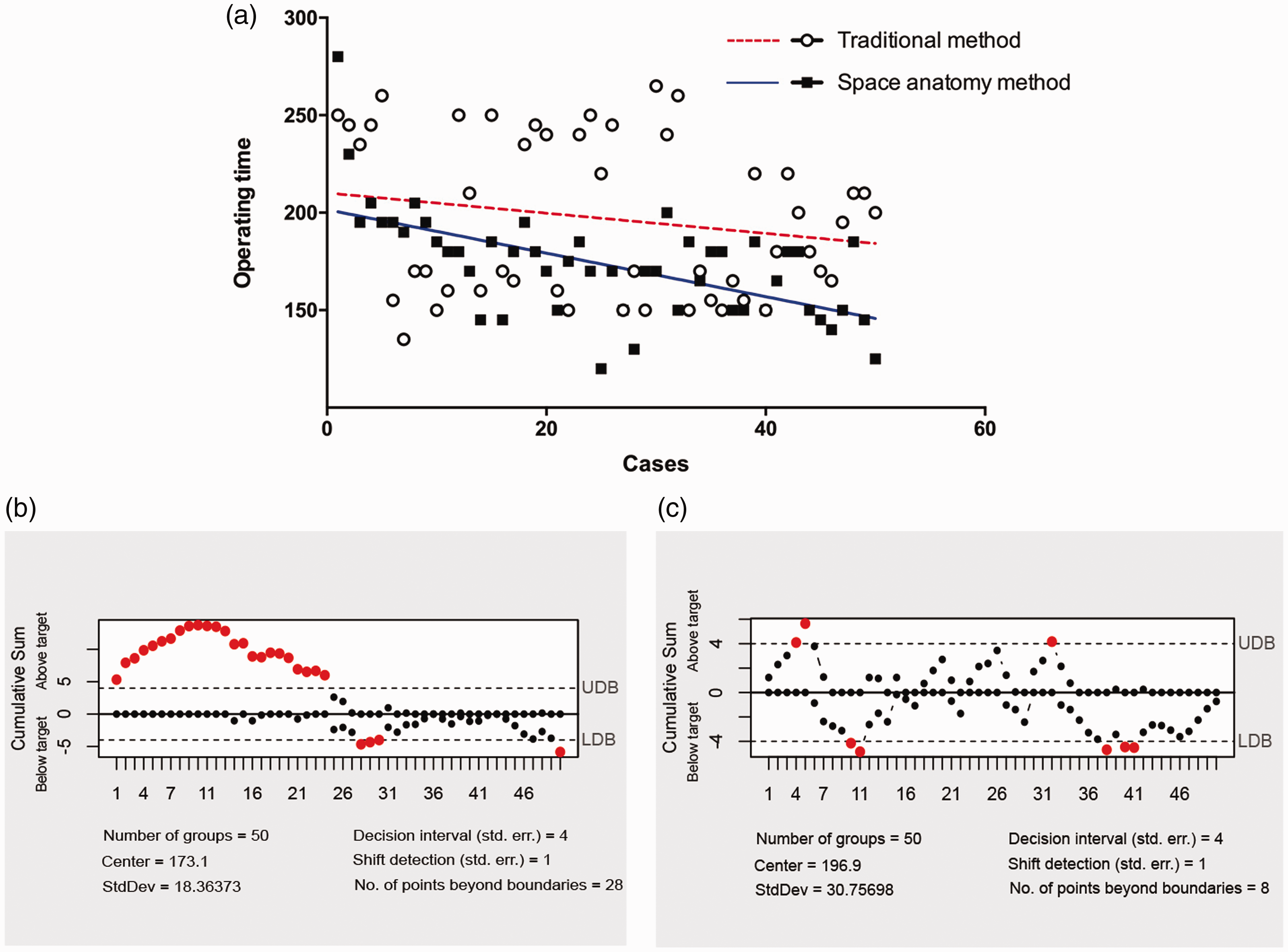
(a) Regression analysis of the operative time in laparoscopic radical hysterectomy by the anatomical space method (n = 50, β coefficient = −1.1160) and the traditional method (n = 50, β coefficient = −0.5188). (b, c) Learning curve for laparoscopic radical hysterectomy by the anatomical space and traditional methods using cumulative sum charts.
Follow-up data
The median follow-up period was 28.5 months (range: 3–51 months). No patients had local recurrence or metastasis. However, long-term follow-up and more studies are required to confirm our data on the oncological outcome.
Discussion
Knowledge of the precise anatomy is important for surgical treatment of cervical cancer, which contributes to complete removal of the tumour and avoidance of injury to the ureter and bladder. The theoretical basis of this treatment is the conception of anatomical space proposed by surgeons. Potential spaces, such as the axillary, paravesical, and paravaginal spaces, and the fourth space of Yabuki, are located at relative fixed positions along the ureteral space. The fourth space of Yabuki was developed during dissection of the VUL in our proposed surgical method. The ureteral space is different from the so-called ureteral tunnel. The ureteral tunnel refers to the course of the ureter through the VUL and into the bladder. The ureteral space is a potential avascular space along the medial side of the ureter and the lateral side of the cervix and upper vagina. Therefore, the term “ureteral space” is reasonable and practical.
The Karez water system is an aquatic system that was developed under severe arid climatic conditions of the Turfan oasis in Xinjiang Uygur Autonomous Region in western China. 11 The melting snow water from the Tianshan mountains forms the groundwater. Vertical shafts (called Karez) were dug along an underground channel (similar to the ureteral space) to determine the location of groundwater (similar to the ureter). The theoretical basis of the anatomical space method is that several potential avascular spaces (vertical shafts) could be developed during dissection of the anterior and posterior leaves of the VUL, thereby reducing blood loss and avoiding injury to the ureter.
Based on the potential surgical spaces, we developed a dissection procedure for management of the VUL during LRH in this study. In the parametrium, the ureter is covered by the VUL, which is defined as a peritoneal fold from the cervix to the bladder. Within the parametrial connective tissue, the superficial uterine vein runs parallel to the uterine artery. After separating the uterine artery and superficial uterine vein from the ureter, we exposed the axillary space (the starting portion of the ureteral space). After complete separation of the bladder, the fourth space of Yabuki (the ending portion of the ureteral space) was exposed. Between the two spaces, we developed several avascular areas near the vascular bundles, and subsequently coagulated and transected the cervicovesical blood vessels. Similarly, the paravaginal space and the paravesical space were developed into Karez, and almost all of the vascular bundles in the posterior leaf of the VUL were isolated between the two spaces. Following these steps, the connective tissue containing the vascular bundles was completely transected by Ligasure with minimal blood loss. We found less blood loss and a shorter operative time in our anatomical space method compared with previous studies. 12 , 13 Moreover, no intraoperative complications were observed. Therefore, the method for dissection of the VUL proposed in this study is safe and effective.
A recently published prospective, randomized trial showed that minimally invasive radical hysterectomy (MIRH) was associated with a higher long-term recurrence rate and lower overall survival than open radical hysterectomy in patients with early-stage cervical cancer. 14 , 15 The high recurrence rate in the MIRH group may be attributed to an improper surgical technique or carelessness of the operator, and not the surgery itself. Future trials evaluating safety of MIRH should focus on modification of the technique. 16 Increasing evidence has shown that MIRH is as effective as open radical hysterectomy in terms of surgical and oncological outcomes in the treatment of early-stage cervical cancer (FIGO stage IB1). 17 , 18 Robotic and laparoscopic approaches to radical surgery in patients with early-stage cervical cancer have similar perioperative and postoperative outcomes. 19 Additionally, THUNDERBEAT is associated with a shorter operative time and less postoperative pain than the standard technique in patients with cervical cancer. 20 Nonetheless, irrespective of the technique, the main goal of treatment for cervical cancer is complete removal of the tumour if possible. Moreover, surgeons should be aware of the Laparoscopic Approach to Carcinoma of the Cervix trial, and the results of this trial should be discussed with patients with cervical cancer who are scheduled for radical hysterectomy.
Our study has several limitations. This study was retrospective in nature and data were obtained from a single centre. Therefore, our study may have biases associated with selection and incomplete data collection, which could have greatly interfered with interpretation of the oncological outcomes. Moreover, patients had a relatively short follow-up period. However, despite these limitations, the current study showed that the surgical technique of LRH was improved and the safety of this technique was evaluated in patients. Furthermore, the proposed method could be used in laparoscopic and open surgeries.
The surgical method based on anatomical spaces is safe and practical for separation of the ureter from the VUL during LRH, and is helpful for improving surgical efficiency and reducing intraoperative complications. As the starting point of the ureteral space, exposure of the axillary space contributes to effective dissection of the ureteral space between the ureter, cervix, and upper vagina. Because our retrospective study was subject to bias, future large-scale, multicentre studies are required to confirm the effectiveness of this method in overall survival of patients.
Footnotes
Authors’ contributions
JW and LLS were responsible for writing the manuscript. TN, YH, and LHW participated in recruitment of the patients and collection of data. JJY and QF conducted statistical analyses. YDW and YHL designed and supervised the study.
Data availability
The datasets analysed during the current study can be made available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Shanghai Municipal Key Clinical Specialty (shslczdzk06302), the National Natural Science Foundation of China (Nos. 81172477, 81402135), the Project of the Science and Technology Commission of Shanghai Municipality (No. 17441907400), Shanghai Jiao Tong University Medicine-Engineering Fund (No. YG2017MS41), and the Youth Scientific Research Project of Shanghai Municipal Commission of Health and Family Planning (20184Y0211).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.