
Abstract
Objective
To investigate the impact of enhanced recovery after surgery (ERAS) on the postoperative neutrophil–lymphocyte ratio (NLR) in patients with colorectal cancer.
Methods
A total of 200 patients with colorectal cancer who underwent surgery between January 2015 and November 2018 were enrolled in the study. They were divided into a traditional treatment group (n=100) and an ERAS group (n=100). The traditional treatment group underwent radical laparoscopic colorectal surgery, and the ERAS group underwent traditional treatment plus the ERAS protocol (preoperative improvement of glucose tolerance, unconventional indwelling stomach and urinary tubes, intraoperative body temperature management, fluid management, postoperative pain management, early oral feeding, and early activities). Clinical data were collected for all patients. NLR levels before and after surgery, and complications were compared between the two groups.
Results
Postoperative NLR was significantly lower in the ERAS compared with the traditional treatment group. The incidence of complications, including anastomotic leakage, pulmonary infection, urinary tract infection, and cardiopulmonary dysfunction were also significantly lower in the ERAS group.
Conclusion
Enhanced recovery after surgery can reduce the increase in postoperative NLR and reduce the occurrence of postoperative complications, which results will be of clinical value.
Keywords
Introduction
Colorectal cancer (CRC) is the third most common malignant tumor worldwide with the fourth highest mortality rate,1,2 and is ranked fifth in terms of incidence and mortality in China. 3 Surgery is currently the most effective treatment option for CRC, combined with other treatments for a comprehensive approach. However, traditional colorectal surgery has a long preoperative preparation time, and is associated with an obvious perioperative stress response, slow recovery of postoperative gastrointestinal function, and numerous complications. Kehlet and Slim 4 first proposed the concept of enhanced recovery after surgery in the late 1990s (fast track surgery), and its subsequent improvement has since led to the development of the enhanced recovery after surgery (ERAS) concept. ERAS has been practiced in the field of CRC for > 10 years. ERAS protocols have evolved from simple postoperative accelerated rehabilitation to treatment measures around the perioperative period, and the relevant diagnosis and treatment approaches can effectively aid patient recovery, reduce treatment time, and reduce medical expenses and hospital resources.
Inflammation has been identified as a carcinogenic factor, with increasing evidence of an important role for inflammation in the development of cancer. 5 Inflammation has also been associated with the occurrence and severity of surgical complications; 6 for example, the neutrophil–lymphocyte ratio (NLR) has been associated with the prognosis of multiple malignancies, with a high NLR indicating a poor prognosis.7–9 McSorley et al. 5 showed that NLR was associated with postoperative complications, confirming that inflammation could be used as a predictor of certain postoperative complications.10,11
The current study aimed to assess the impact of ERAS on postoperative NLR in patients with CRC, and to establish laboratory indicators of ERAS compared with traditional perioperative management.
Patients and methods
General information
Patients with CRC treated at The Fifth People’s Hospital of Chongqing from January 2015 to November 2018 were eligible for the study. The inclusion criteria were as follows: 1) pathologically confirmed CRC; 2) treated with one-stage radical resection (excluding Miles procedure) by the same group of doctors; 3) good nutritional status; 4) no significant heart, lung, kidney, or other important organ dysfunction; 5) no distant tumor metastasis; 6) no previous abdominal surgery; 7) no radiotherapy or chemotherapy; and 8) anesthesia ASA score < 4 points. The exclusion criteria were: 1) patients with such intestinal as obstruction or perforation requiring immediate surgery; 2) severe malnutrition; 3) poor mobility; 4) anesthesia ASA score > 4 points; and 5) mental illness.
Patients were divided into two group: a traditional treatment group collected from January 2015 to December 2016, and an ERAS group collected from January 2017, included in chronological order. Clinical data were collected and compared between the two groups, including information on age, sex, ASA grade, basic disease, tumor location, stage, and physiological index. All patients provided signed informed consent for participation in the study, and this study was approved by the Ethics Committee of The Fifth People's Hospital of Chongqing from January 2015.
Treatment
All patients underwent the usual examinations and preoperative preparations. All patients were treated by the same surgeon. The same laparoscopic instruments were used by the same group of doctors, and all patients underwent radical laparoscopic colorectal surgery according to their condition. The traditional treatment group underwent radical laparoscopic colorectal surgery, and the ERAS group underwent the same surgical procedure combined with ERAS protocol for diagnosis and treatment. The respective treatments are detailed in Table 1.
Comparison of intervention measures during the perioperative period between the ERAS and control groups.
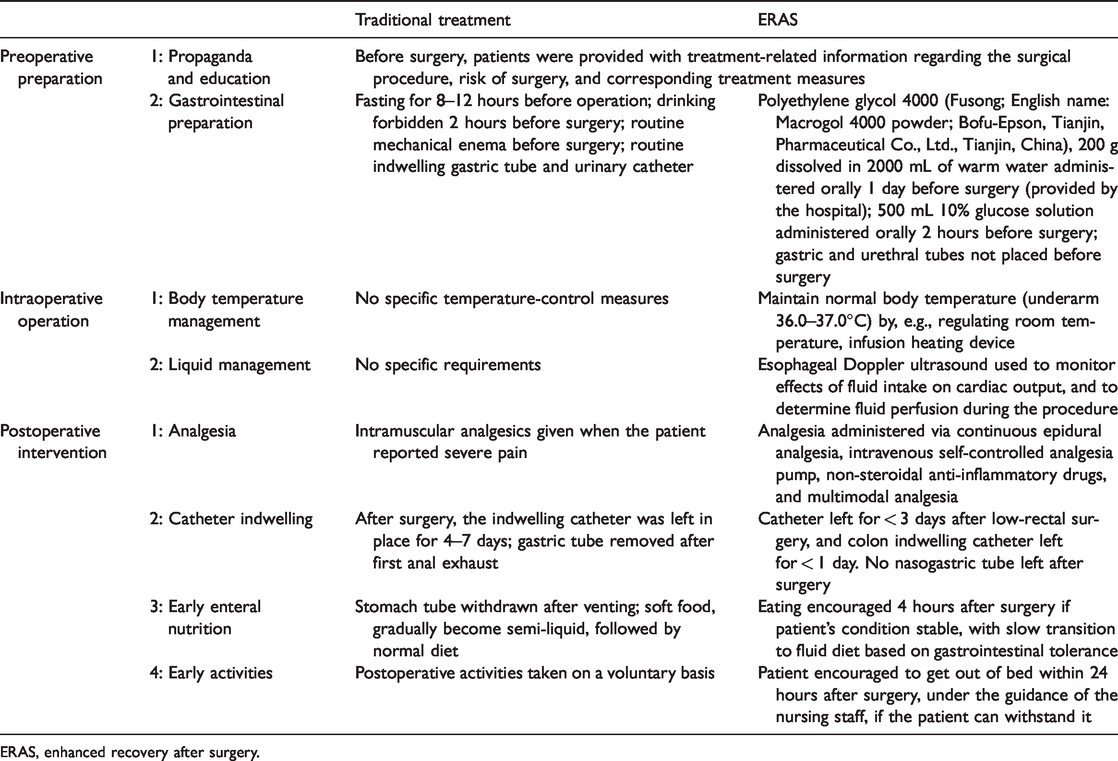
ERAS, enhanced recovery after surgery.
Observation index
Fasting peripheral blood was collected from all patients within 24 hours before surgery, and the preoperative NLR (expressed by the absolute value of neutrophils divided by the absolute value of lymphocytes) was calculated. To assess the postoperative inflammatory response, fasting peripheral blood was drawn at 9 a.m. on postoperative day 3 to calculate postoperative NLR, just as the computing method of Janez et al. 12 Complications, including anastomotic leakage and pulmonary infection, were observed in both groups during the course of treatment.
Statistical analysis
All collected information was analyzed using SPSS Statistics for Windows, version 22.0 (SPSS Inc., Chicago, IL, USA). Quantitative variables with a normal distribution were expressed as mean ± standard deviation. Differences between the two groups were compared using t-tests, and qualitative data were analyzed using χ2 tests. A value of P < 0.05 indicated statistical significance.
Results
Patient information
A total of 200 patients were enrolled according to the inclusion and exclusion criteria, including 100 patients in the traditional treatment group and 100 in the ERAS group. The patient characteristics are shown in Table 2. There was no significant difference in age, sex, body mass index, anesthesia ASA score, tumor site, or tumor TNM stage between the traditional treatment group and the ERAS group.
Comparison of preoperative clinical data between the two groups.

Data presented as mean ± standard deviation or n. ERAS, enhanced recovery after surgery; BMI, body mass index.
Postoperative complications
The postoperative complications in each group are presented in Table 3. Among the postoperative complications, the incidences of anastomotic leakage, pulmonary infection, urinary tract infection, and cardiopulmonary dysfunction were all significantly higher in the traditional compared with the ERAS group (P < 0.05), but there was no significant difference in deep vein thrombosis, wound infection, gastrointestinal bleeding, and postoperative intestinal obstruction. All patients were discharged after symptomatic treatment.
Comparison of postoperative complications between the two groups.
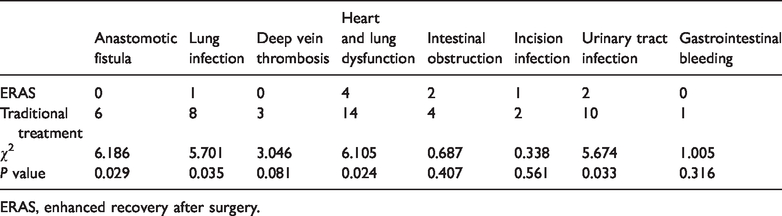
ERAS, enhanced recovery after surgery.
Postoperative recovery
Details of the postoperative recovery parameters are presented in Table 4. First exhaust time, first defecation time, length of hospital stay, and hospitalization cost were all significantly longer in the traditional compared with the ERAS group (P < 0.01).
Comparison of postoperative data between the two groups.

Perioperative laboratory data
Laboratory data for the two groups are presented in Table 5. There was no significant difference in preoperative NLR between the two groups, but postoperative NLR was significantly higher in the traditional compared with the ERAS group (P < 0.01). There was also no significant difference in preoperative total protein (TP) or preoperative albumin (ALB) between the groups, but postoperative TP and postoperative ALB were both significantly higher in the traditional compared with the ERAS group (P < 0.01).
Comparisons of neutrophil–lymphocyte ratio, total protein, and albumin during the perioperative period between the two groups.

ERAS, enhanced recovery after surgery; NLR, neutrophil–lymphocyte ratio; TP, total protein; ALB, albumin.
Discussion
Previous studies have shown that postoperative pain, surgical stress (e.g., organ dysfunction), postoperative nausea and vomiting, intestinal obstruction, restricted mobility, drainage tube, and discomfort caused by a stomach tube can all affect the rehabilitation of patients after colorectal surgery. 13 It is therefore necessary to develop appropriate intervention methods to address the source of the stress, and to explore the best postoperative management programs.14,15 Accelerated rehabilitation and recovery after surgery can be promoted by reducing postoperative pressure, rational treatment of pain, early recovery diet, and early activities.
Preoperative bowel preparation can cause dehydration and electrolyte imbalance, especially in elderly patients, 16 with a risk of intestinal bacteria-related disorders. Similarly, a previous meta-analysis 17 showed that bowel preparation was not beneficial in patients undergoing colon surgery, and may increase the risk of postoperative anastomotic leakage. However, preoperative bowel preparation is suitable for patients requiring intraoperative colonoscopy or who have severe constipation, and it may also promote postoperative gastrointestinal functional recovery. In the current study, patients in the ERAS group did not undergo preoperative mechanical bowel preparation and had significantly shorter times to first anal exhaust and defecation compared with the conventional treatment group, in accord with the results of numerous previous studies.18–20 However, both the traditional treatment group and the ERAS group had longer times to first exhaust and defecation compared with other studies. 21 This apparent discrepancy may be due to differences in marking the time to first venting and defecation; although early irregular postoperative intestinal activity can result in exhaust, only exhaust during regular gastrointestinal activity represents overall recovery of intestinal function. Furthermore, the experimental subjects in the current were relatively old, which may also have affected the results.
Surgical treatment may cause not only physiological trauma, but also a stress response, in patients with CRC, 22 characterized by increased catabolism. In the current study, TP and ALB levels decreased significantly after surgery in both groups; however, levels of ALB and TP on postoperative day 4 were significantly higher in the ERAS group compared with the traditional treatment group. This may be a direct benefit of early oral feeding, though some studies have indicated that it may promote insulin sensitivity by regulating the stress response, which reduces protein breakdown. 23
To reduce complications such as postoperative fever, atelectasis, pneumonia, and gastric retention, stomach tubes should not be placed routinely in patients undergoing rectal surgery. 24 Placement of a drainage tube can cause pain in the wound and surgical site, with negative effects on the patient. Furthermore, early out-of-bed activities and the use of an abdominal drainage tube cannot reduce the occurrence of complications such as anastomotic leakage. 25 Removing the drainage tube as soon as possible after surgery aids early patient activity, thus avoiding wound infection, pneumonia, and bed-rest complications such as gastric retention. In this study, the incidence of complications was generally lower in the ERAS group compared with the traditional treatment group, with significantly lower incidences of anastomotic leakage, pulmonary infection, urinary tract infection, and cardiopulmonary dysfunction, as seen in other studies. 26 However, there was no significant difference in the incidence of deep vein thrombosis, wound infection, gastrointestinal bleeding, or postoperative intestinal obstruction. This may have been because patients in the traditional treatment group received relevant physiotherapy during the hospitalization period; however, although this practice can be beneficial during the perioperative period, it also increases hospitalization costs. A previous study of the ERAS program in CRC patients aged > 80 years 19 showed that prolonged hospitalization was an independent risk factor for postoperative complications, consistent with the current results.
The inflammatory response occurs throughout the perioperative period in patients with CRC, resulting in an imbalance between pro-inflammatory and anti-inflammatory cytokines. Increased and prolonged inflammation has been shown to increase mortality and morbidity. 27 The NLR and platelet-lymphocyte ratio are simple peripheral blood parameters for assessing the inflammatory response and physiological stress during the perioperative period. 28 The neuroendocrine system is activated during anesthesia and surgery, leading to the release of neuroendocrine hormones and cytokines,29,30 and systemic leukocyte changes (including leukocytosis, neutropenia, and lymphopenia) may occur in response to various hormones during and after surgery, cytokines and acute phase reactants, lymphocyte apoptosis, or inhibition of neutrophil apoptosis. 31 The preoperative NLR reflects the relationship between tumor progression and the body’s immune system, with high values often indicating greater tumor proliferation and metastatic ability, and relatively low immune function. The postoperative NLR is associated with the postoperative stress response, 32 reflecting the body’s inflammatory response and potential for self-repair. In the current study, the postoperative NLR was higher than the preoperative NLR, suggesting a poor prognosis or excessive inflammatory response. A previous study evaluating the correlation between NLR and postoperative complications in patients undergoing major abdominal surgery found a cut-off NLR for postoperative complications of 5.5. 33 NLR is not only affected by surgical trauma, but also by anesthesia. 34 ERAS procedures were carried out throughout the perioperative period, including reasonable preparation before surgery, strict control during surgery, and a series of early recovery programs that have proven effective in reducing the patient’s stress and inflammatory responses, thereby reduced the occurrence of complications.
This study was limited by its long time span, and the results may therefore have been affected by any increase in surgical skills and experience throughout the course of the study.
The results of the current study showed that ERAS could effectively reduce the stress response, surgical damage due to hypothermia and excess fluid rehydration, the infection rate, and hospitalization costs, as well as shortening hospitalization time. The change in NLR can be used as a testing indicator, and suggests that ERAS is better than traditional perioperative management in terms of patient rehabilitation.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.