
Abstract
Objective
Autoantibody-related congenital heart block (ACHB) is a passively acquired autoimmune disease. This study aimed to examine the pathogenesis, clinical manifestations, and treatment of ACHB.
Method
The clinical data of two fetuses with first-degree ACHB were retrospectively analyzed.
Results
Two pregnant women were strongly positive for anti-Sjögren’s syndrome-related antigen A (SSA) antibody. Among these two cases, one had a prolonged atrioventricular (AV) interval at 28+3 weeks in utero, while the other had a prolonged AV interval at 24+6 weeks in utero. After prenatal intervention, one patient recovered to normal, while one fetus continued to have ACHB after treatment with dexamethasone and intravenous immunoglobulin. Furthermore, the two neonates were positive for anti-SSA antibody and were diagnosed with ACHB.
Conclusion
The pathogenesis of ACHB is closely correlated with anti-SSA/Ro antibody and anti-SSB/La antibody from the mother, and is affected by fetal susceptibility. Early screening and early intervention for ACHB are important.
Keywords
Introduction
Autoantibody-related congenital heart block (ACHB) is a type of disease in which the fetus passively obtains maternal autoantibodies (anti-Sjögren’s syndrome-related antigen A [SSA]/Ro antibody and anti-SSB/La antibody) and these interfere with cardiac conduction in the process of growth and development. 1 Almost all occurrences of ACHB are correlated with maternal autoantibodies (anti-SSA/Ro antibody and anti-SSB/La antibody), but there is no cardiac structural abnormality. Furthermore, the perinatal mortality rate can be up to 20% to 30%. The mortality rate of ACHB is higher with endocardial fibroelastosis or cardiomyopathy, and more than two thirds of children need to be implanted with permanent cardiac pacemakers. 2
At present, the pathogenesis of ACHB is thought to mainly include inflammation and electrophysiology. SSA/Ro antigen is a ribonucleoprotein complex that comprises Ro52 and Ro60 polypeptides. In the inflammatory hypothesis for the pathogenesis of ACHB, the anti-Ro60 antibody binds to apoptotic cardiomyocytes, and induces phagocytosis of apoptotic products by conditioning of macrophages, leading to inflammatory reactions and induction of more apoptosis. 3 Additionally, macrophages produce cytokines that promote inflammation and fibrosis, which in turn promotes myocardial fibrosis. 4 In the electrophysiology for ACHB, anti-Ro antibody acts on some calcium channels that regulate the electrophysiological activity of the atrioventricular (AV) node. 5 The Ro52 antibody combines with cardiac muscle cells and leads to accumulation of intracellular calcium ions because of imbalance of calcium homeostasis. Cardiac muscle cells then overload and lose their contraction function, which eventually lead to myocardial apoptosis, 6 thereby causing AV block.
ACHB often occurs in utero, and starts in the second or third trimester of pregnancy. ACHB is a type of progressive disease with incomplete retardation of conduction and gradual progression to third-degree complete retardation of conduction. Once complete heart block occurs, the damage is often irreversible.7,8
To date, no therapy has been found to be effective in preventing progression of heart injury and reversing autoantibody-associated congenital heart block in large case studies. Recently, combined therapies have been proposed and attempted, and appear to be promising. In the present study, two pregnant women with fetuses with first-degree congenital heart block were treated and followed up, and both women received combined therapies in a different order. The women had different outcomes.
Cases
Case 1
A 28-year-old female patient, who was strongly positive for anti-SSA antibody and anti-Ro52 antibody, was pregnant for 20+1 weeks and was diagnosed with connective tissue disease in Beijing Anzhen Hospital, Capital Medical University. She underwent fetal echocardiography to monitor the AV interval. Eleven fetal echocardiographic examinations were performed (Table 1). This was the patient’s first pregnancy, which was a natural pregnancy, and the pregnant woman had no history of heart disease. Furthermore, the patient was under the guidance of the doctor while the condition was stable. The fetus was well, and biometric measurements were consistent with the gestational weeks. Furthermore, there were no cardiac structural abnormalities.
Monitoring of the atrioventricular interval and medication of case 1 during pregnancy.
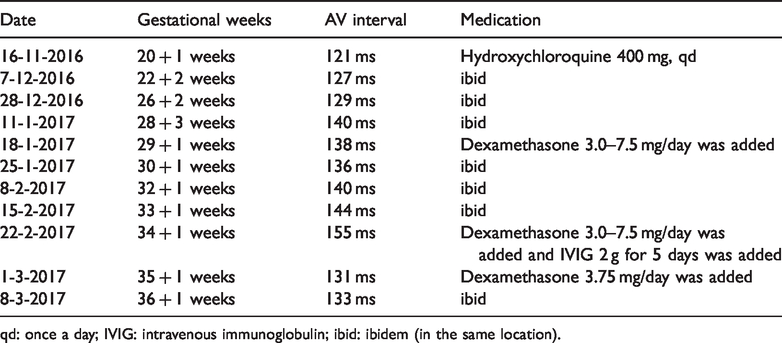
qd: once a day; IVIG: intravenous immunoglobulin; ibid: ibidem (in the same location).
The patient received hydroxychloroquine 400 mg once a day during pregnancy. She received her first fetal echocardiography at 20+1 weeks of gestation, with an AV interval of 121 ms, which was in the normal range. However, at 28+3 weeks of gestation, the AV interval was prolonged to 140 ms, which was first-degree AV block. Dexamethasone was added at a dose of 3.0 to 7.5 mg/day, and the AV interval decreased to the normal range. However, the AV interval lengthened again at 32+1 weeks of gestation, and was found to be aggravated after 1 week. Therefore, human immunoglobulin was added at 20 g/day for 5 days, and the AV interval was reduced to the normal range and maintained to full term. The patient underwent cesarean section at 37+2 weeks, and gave birth to a girl with a birth weight of 3300 g. The amniotic fluid was clear at birth, the Apgar score was 10 points, and echocardiography at 55 days after delivery showed a normal range of the AV interval.
Case 2
A 26-year-old female patient, who was strongly positive for anti-SSA antibody, was pregnant for 18+6 weeks and was diagnosed with connective tissue disease in Beijing Anzhen Hospital, Capital Medical University. She underwent fetal echocardiography to monitor the AV interval. Eight fetal echocardiographic examinations were performed (Table 2). This was the patient’s first pregnancy, which was a natural pregnancy, and the patient had no history of heart disease. The patient was under the guidance of the doctor while the condition was stable. The fetus was well, and biometric measurements were consistent with the gestational weeks. There were no cardiac structural abnormalities.
AV interval monitoring and medication of case 2 during pregnancy.
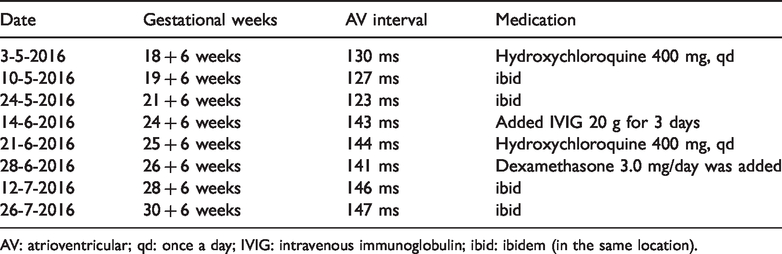
AV: atrioventricular; qd: once a day; IVIG: intravenous immunoglobulin; ibid: ibidem (in the same location).
This pregnant woman received hydroxychloroquine 400 mg once a day during pregnancy, and received her first fetal echocardiography at 18+6 weeks of gestation, with an AV interval of 130 ms, which was in the normal range. However, at 24+6 weeks of gestation, the AV interval was prolonged to 143 ms, which was first-degree atrioventricular block. Therefore, human immunoglobulin at 20 g/day was added, and the patient was rechecked after 3 days. The AV interval was 144 ms, which was still prolonged. Therefore, dexamethasone was added at a dose of 3.0 mg/day. However, the AV interval still remained >140 ms, and continued up to full term. The patient underwent cesarean section at 37 weeks, and gave birth to a male neonate, with a birth weight of 2700 g. The amniotic fluid was clear at birth, the Apgar score was 10 points, and the neonate underwent echocardiography and an electrocardiogram (Figure 1) at 15 days after delivery. All results showed first-degree congenital heart block.

Postpartum electrocardiogram of the child of case 2.
After delivery, the two neonates were examined and confirmed to be positive for anti-SSA antibody. These data had been recorded in the medical records. The need for study approval was waived because measurements were taken during routine examinations for the pregnant women. The patients provided verbal informed consent.
Discussion
ACHB is a type of passively acquired autoimmune disease. However, autoantibodies are not the only factors that can cause this disease. The incidence of ACHB in the fetus during a first pregnancy is approximately 2% and that during a second pregnancy is approximately 19%. 9 Therefore, the role of fetal susceptibility in this disease cannot be ignored. Recent studies have suggested that major histocompatibility complexes are involved in regulating fetal susceptibility and determining fetal disease results in anti-Ro52 antibody-positive pregnancies. 10 ACHB is usually found by fetal echocardiography at 18 to 24 weeks of gestation, and it initially manifests as first-degree or second-degree AV block, or even as third-degree AV block. An AV interval (P-R interval) of >140 ms can be diagnosed as first-degree AV block in fetal echocardiography. The occurrence of fetal AV block is a gradual process, and it usually manifests as first-degree and second-degree conduction block in the early stage. Without intervention and treatment, this may gradually worsen, leading to occurrence of a complete AV block. Therefore, intervention of prenatal and postnatal treatment can improve some first-degree and second-degree AV blocks, and even return to normal. 11 Furthermore, this degree of block can stabilize third-degree AV block, increase the ventricular rate, improve cardiac function, and prevent complications, such as cardiomyopathy or fetal edema. According to a study by Sonesson et al., 12 even if the clinical significance of fetal AV conduction delays remains to be determined, a fetal AV interval of >150 to 155 ms may be a marker of permanent disruption of AV conduction pathways, especially when observed in two consecutive examinations.
Although ACHB may be detected as early as the middle stage of pregnancy, there is still no uniform clinical guideline for reference in terms of prenatal intervention and postnatal treatment. The scientific statement for the diagnosis and treatment of fetal cardiovascular diseases of the American Heart Association in 2014 13 is shown in Table 3. When fetuses have second-degree AV block or first-degree AV block with heart inflammation, dexamethasone is administered to prevent congenital heart block-related death and cardiomyopathy. Dexamethasone treatment for fetuses with established congenital heart block and no heart failure may also be considered, with the goal of improving survival or reducing the incidence of dilated cardiomyopathy. However, the usefulness of dexamethasone has not been established because previous studies were retrospective and nonrandomized, and they reported incomplete follow-ups.
Intrauterine treatment of atrioventricular block. 12

CHB: congenital heart block; SSA/SSB: Sjögren’s syndrome-related antigen A/B.
The present intervention methods for ACHB include hormones (non-fluorinated hormones and fluorinated hormones), immunoglobulins, plasma exchange, and other methods. Some studies have shown that plasma exchange and the combined use of immunoglobulin and steroid hormones significantly improve heart rate at birth and reduce the implantation rate of pacemakers within 1 year after birth. 11 Other studies have reported that plasma exchange can stabilize and significantly decrease antibody levels of antibody-positive pregnant women, and subsequently reverse the fetal congenital heart block. 14 This is important for stability of the developmental process of fetal congenital heart block to complete block. Although some treatment schemes have shown some benefits, more large-scale studies are required to confirm the timing and effectiveness of intrauterine intervention through the placenta.
In summary, ACHB is closely correlated with anti-SSA/Ro antibody and anti-SSB/La antibody from the mother, and is affected by fetal susceptibility. Although autoantibody-associated congenital heart block may initially be detected as a first- or second-degree AV block, most of the affected pregnancies present with fetal bradycardia with third-degree (complete) AV block, and the ventricular rates are typically between 50 and 70 beats per minute. Therefore, choosing methods to accurately measure the AV conduction time, and carry out early screening and early intervention for AV blocks is clinically important. However, at present, the prenatal treatment scheme of fetal ACHB is not well defined. Some studies have suggested that prenatal and postnatal combined treatment may help to improve the severity and prognosis of fetal ACHB.15,16 However, confirmation of new treatment methods for this condition requires large clinical, randomized, controlled trials and general medical evidence to be finally applied in the clinic.
In the present study, two fetuses with ACHB were treated with combined therapies and followed up. The mothers had different outcomes. Dexamethasone and intravenous immunoglobulin were clinically added when the AV interval was prolonged, but the order of use and dosage were not the same in each woman. This finding indicated that there is a lack of standard guidance for clinical medication in this situation. Therefore, more attention should be paid to ACHB and to early establishment of standard treatment.