
Abstract
His bundle pacing is a relatively new method of cardiac pacing. This method is used in patients with atrioventricular block to prevent heart failure associated with right ventricular pacing, and in patients with bundle branch block and cardiomyopathy. We report a patient with cardiomyopathy and left bundle branch block with failure of cardiac resynchronization therapy. Permanent His bundle pacing was associated with clinical improvement and improvement of parameters of cardiac function.
Keywords
Introduction
Pacing of the His bundle was first realized in humans in 1970 in an experimental study as temporary pacing. 1 Clinical series with permanent His bundle pacing were reported from 2000 in different patient populations. 2 There is a lower incidence of new-onset heart failure after His bundle pacing compared with the conventional right ventricular pacing in patients with atrioventricular blockade. His bundle pacing was also tested as an alternative to cardiac resynchronization therapy (CRT) in patients with left bundle branch block and cardiomyopathy. 3 We report a patient with cardiomyopathy and left bundle branch block with failure of CRT. His bundle pacing (HBP) was used as an alternative therapy in this patient.
Case study
We report a case of a 75-year-old woman with non-ischemic dilated cardiomyopathy and left bundle branch block with an estimated left ventricular (LV) ejection fraction of 25%. She had advanced heart failure symptoms with New York Heart Failure functional classification (NYHA) III. The patient had a history of significant comorbidities, including hypothyroidism, arterial hypertension, chronic obstructive pulmonary disease, obesity, and anemia. Despite optimal medical therapy, including the maximal tolerated dose of a beta-blocker, angiotensin receptor blocker, mineralocorticoid receptor antagonist, and loop diuretic, the patient’s symptoms remained unchanged.
The patient was indicated for CRT with an implantable defibrillator. Implantation of the lead for the LV was technically unsuccessful because of anatomical variability of the cardiac venous system. The patient was referred for surgical epicardial implantation of an LV lead and surgery was performed on 12 September 2018. On the day of the first pacemaker clinic visit, malfunction of the LV lead was found. Because of the high risk of reoperation, we decided to refer the patient for HBP. Implantation of a lead for HBP was successful (Figure 1). HBP was associated with an immediate change in QRS width on electrocardiography (Figure 2). The patient was followed and we repeated clinical, laboratory, and echocardiographic examinations after 3 months of HBP (Table 1). The NYHA functional class improved to NYHA II, N-terminal fragment of pro-brain natriuretic peptide levels were decreased by 50%, and a repeated echocardiographic study showed an increase in the LV ejection fraction as a parameter of systolic function. Diastolic LV function was also improved as shown by pulse Doppler and tissue Doppler imaging. Systolic pulmonary flow (type of acceleration time) as an indirect parameter of pulmonary hypertension was also improved.

Chest X-ray showing the position of the leads. RA, right atrium; HBP, His bundle pacing; ICD, implantable cardiac device; RV, right ventricle.
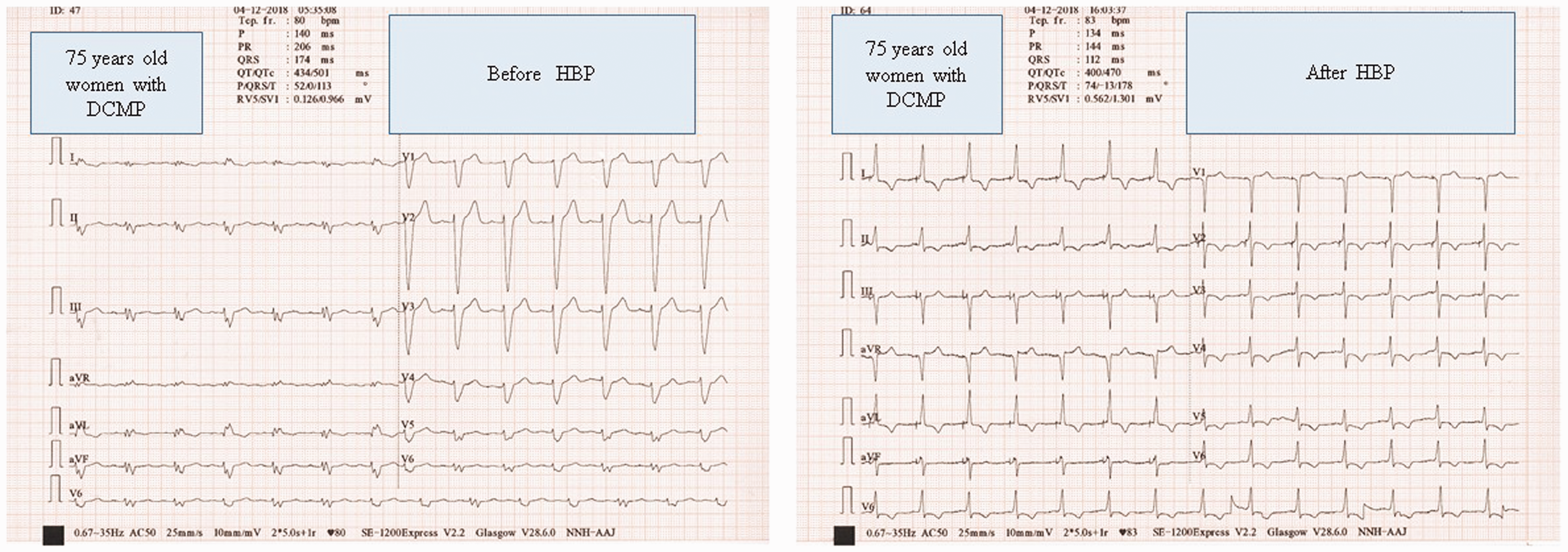
Immediate electrocardiographic change before and after His bundle pacing. QRS width: 174 ms and 112 ms. DCMP, dilated cardiomyopathy; HBP, His bundle pacing.
Changes in echocardiographic, and clinical and laboratory parameters 3 months after HBP.
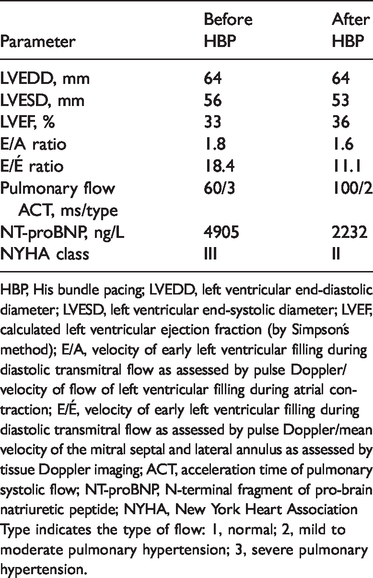
HBP, His bundle pacing; LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; LVEF, calculated left ventricular ejection fraction (by Simpson´s method); E/A, velocity of early left ventricular filling during diastolic transmitral flow as assessed by pulse Doppler/velocity of flow of left ventricular filling during atrial contraction; E/É, velocity of early left ventricular filling during diastolic transmitral flow as assessed by pulse Doppler/mean velocity of the mitral septal and lateral annulus as assessed by tissue Doppler imaging; ACT, acceleration time of pulmonary systolic flow; NT-proBNP, N-terminal fragment of pro-brain natriuretic peptide; NYHA, New York Heart Association
Type indicates the type of flow: 1, normal; 2, mild to moderate pulmonary hypertension; 3, severe pulmonary hypertension.
Approval for the study was granted by the ethics committee of Na Homolce Hospital. The patient signed an informed consent form for the procedure as per institutional guidelines. The patient also provided consent for publication.
Discussion
Our case study showed that permanent HBP may be used in patients with cardiomyopathy, left bundle branch block, and failure of CRT. Biventricular pacing is a standard method for patients with cardiomyopathy, left bundle branch block, and advanced symptoms of heart failure. Biventricular pacing was shown to reduce mortality and morbidity in randomized, clinical trials.4,5 The effect of CRT may be monitored by assessment of clinical signs and symptoms and predicted by laboratory parameters. 6 Implantation of an LV lead is not always technically successful, usually because of variability of the cardiac venous system. Another disadvantage of biventricular pacing is that it does not completely normalize intraventricular activation. HBP was introduced because of development of special leads. Recent studies have shown a positive effect of HBP in patients with left bundle branch block and chronic heart failure. HBP also produces physiological pacing in patients with right bundle branch block.
If the ventricular lead is placed on the His bundle, the QRS duration should not be changed because the His bundle is proximal to the left bundle. HBP is effective only in conduction block at the His bundle. In case of conduction block distal from the His bundle, the pacing lead should be placed in the appropriate position. An electrophysiologist is able to reveal the site of conduction block during the procedure and record an immediate effect of pacing on an electrocardiogram. In our case, the block was at the His bundle, and therefore, the effect of pacing was successful.
More studies with larger cohorts with defined clinical outcomes are required to evaluate the effect of HBP in the increasing heart failure population. 7
Conclusion
HBP is a relatively new method of physiological pacing. The indication for HBP is prevention of pacing-induced cardiomyopathy and an alternative to CRT. The possibility of HBP needs to be considered in patients with left bundle branch block and cardiomyopathy when a CRT device cannot be implanted because of anatomical issues.