
Abstract
Objective
We aimed to understand the reasons behind outpatient loss to follow-up and the views of Chinese patients with depression regarding disease diagnosis and antidepressant therapy.
Methods
Consecutive outpatients with newly diagnosed depressive disorder between September 2012 and August 2013 at the Shanghai First People’s Hospital (a tertiary hospital) were categorized into follow-up and lost-to-follow-up groups. We collected information on demographics, the Hamilton depression (HAMD) scale, Self-Rating Depression Scale (SDS), Self-Rating Anxiety Scale, and Symptom Checklist-90. Patients were routinely followed at 2, 4, 8, and 12 weeks. Any missed appointment was considered lost to follow-up.
Results
After 12 weeks of treatment, only 42.2% (70/166) of patients were continuing follow-up. Patients lost to follow-up were significantly younger (median, 42.5 vs. 56.5 years), had different marital status, higher education level, higher SDS score (43.8 ± 10.8 vs. 40.2 ± 10.9), and higher HAMD score (median, 21 vs. 19). Age (odds ratio (OR) = 0.97, 95% confidence interval (CI): 0.95–0.997), and HAMD score (OR = 1.14, 95% CI: 1.01–1.29) were independently associated with loss to follow-up.
Conclusion
Young age, higher HAMD score, and poor knowledge of depression and treatment were the main factors associated with loss to follow-up during depression management among our Chinese patients.
Introduction
In China, the lifetime prevalence of major depressive disorder is 3.3% to 3.6%. 1 Most patients do not receive antidepressant treatment in accordance with the guidelines, and their depressive symptoms relapse. 2 A main cause of relapse is non-adherence to treatment.3,4 Patients with poorly managed and relapsing depression are at higher risk of complications such as suicidal ideation, social strain, loss of workdays, reduced quality of life, cognitive impairment, and mortality. 5 Apart from non-adherence to antidepressives, loss to follow-up is another form of non-adherence to treatment as regular patient assessment and discussions with a psychiatrist are part of optimal patient management of depression.6–8
Many studies outside China have focused on antidepressant adherence.4,9,10 Sexual side effects, low self-efficacy, female sex, and low education level are the primary reasons for low treatment adherence.11,12 In China, most patients with depression are not treated according to the guidelines but instead have short treatment courses and low persistence with treatment. 13 In Chinese patients with depression, depression itself seems to be the main reason for discontinuing treatment;10,14,15 however, these results need to be refined, to improve our understanding of the factors that could predict a loss to follow-up.
In the present study, we aimed to understand the reasons behind outpatient loss to follow-up and the views of Chinese patients with depression regarding disease diagnosis and antidepressant therapy.
Methods
Study design and participants
This was a retrospective study including consecutive outpatients (age 18–75 years) with newly diagnosed depressive disorder at the Shanghai First People’s Hospital (a tertiary hospital) between September 2012 and August 2013. The diagnosis of depression was made according to the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV). 16 The inclusion criteria included Hamilton depression (HAMD) scale score ≥17. 17 The exclusion criteria were: 1) patients with bipolar depression or anxiety disorders owing to organic diseases; 2) other functional mental disorders; and 3) serious physical diseases. This study was approved by the ethics committee of the Shanghai First People’s Hospital. All patients signed an informed consent form.
Grouping
As per routine practice at this hospital, the patient and physician agreed on the date of the following appointment at each visit. Loss to follow-up was defined as failing to present to the appointment, failing to present for up to 2 weeks after the planned date, and no subsequent appointment being made. During the study period, patients who missed a single visit were categorized as the lost-to-follow-up group.
Data collection
Validated Chinese versions of the HAMD scale, 18 Self-Rating Depression Scale (SDS),12,19 Self-Rating Anxiety Scale (SAS), 20 Symptom Checklist-90 (SCL-90), 21 and depression factor (Dep factor) of the SCL-90 were administered routinely at each visit, which were at 2, 4, 8, and 12 weeks, as per routine practice. The characteristics (demographic and socioeconomic factors) of patients and their treatments were collected from the medical charts.
Survey
As per routine practice at our institution, when a patient is considered lost to follow-up, attempts are made to reach the patient and ascertain the reasons for missing follow-up appointments. Patients are told at the first visit that this is the standard procedure, in case the patient refuses follow-up visits. We developed a survey based on the feedback of 37 patients with depression (15 men and 22 women), as well as the relevant literature.11,22 Consistency among assessors was good (kappa of 0.80).
Statistical analysis
We used SPSS version 11.0 (SPSS Inc., Chicago, IL, USA) for the analysis. Continuous data are expressed as mean ± standard deviation, and categorical data are expressed as frequency. To compare data between groups, the Pearson chi-square test, Student t-test, and Mann–Whitney U test were used, as appropriate. Multivariable logistic regression was used to analyze the baseline factors affecting loss to follow-up and included the variables identified in the univariate analyses with P < 0.05. All tests were two-sided and P-values < 0.05 were considered statistically significant.
Results
Patient characteristics
During the study, 166 patients were recruited and categorized into two groups on the basis of loss to follow-up; the follow-up group included 70 patients, and the lost-to-follow-up group included 96 patients. Only 42.2% of patients completed the first 12 weeks of treatment, i.e., acute phase treatment. Table 1 presents the characteristics of participants. Patients who were lost to follow-up were significantly younger (median, 42.5 vs. 56.5 years, P < 0.001), had differing marital status (i.e., married, divorced, and widowed) (P < 0.001), and a higher education level (P = 0.02). There was no difference in the sex distribution. No patients received electroconvulsive therapy because it is not offered at our center. During the study period, no patients were declared to be in remission and discharged by their physician.
Characteristics of patients.

SCL-90: Symptom Checklist-90; Dep factor: depression factor; SDS: Self-Rating Depression Scale; SAS: Self-Rating Anxiety Scale; HAMD: Hamilton Depression Scale.
*Scores are average (range) or mean ± standard deviation.
Patients who were lost to follow-up had higher SDS scores (43.8 ± 10.8 vs. 40.2 ± 10.9, P = 0.03) and higher HAMD scores (median, 21 vs. 19, P = 0.001). There were no differences in SCL-90, Dep factor, and SAS scores.
Rates of follow-up and discontinuation at different time points
The rate of loss to follow-up for outpatients with depression increased gradually over time (Table 2). High loss to follow-up (57.8%, 96/166) was observed at the end of week 12 after the initial visit. Most patients were lost to follow-up at the second visit, with a loss to follow-up rate at week 2 of 39.2% (67.7% of the total lost-to-follow-up group (65/96)); this rate increased to 45.2% at week 4, 53% at week 8, and 57.8% at week 12.
Rate of loss to follow-up at different time points.

*Calculated as % of total cases.
**Calculated as % of cases lost to follow-up.
Univariable and multivariable analyses
Univariable analyses showed that age (P < 0.001), education (P = 0.02), marital status (P = 0.006), SDS score (P = 0.04), and HAMD score (P = 0.002) were associated with loss to follow-up (Table 3). Multivariable analysis showed that age (OR = 0.97, 95% CI: 0.95–0.997, P = 0.03) and HAMD score (OR = 1.14, 95% CI: 1.01–1.29, P = 0.03) were independently associated with loss to follow-up (Table 3).
Univariable and multivariable analyses of baseline factors associated with loss to follow-up at 3 months.
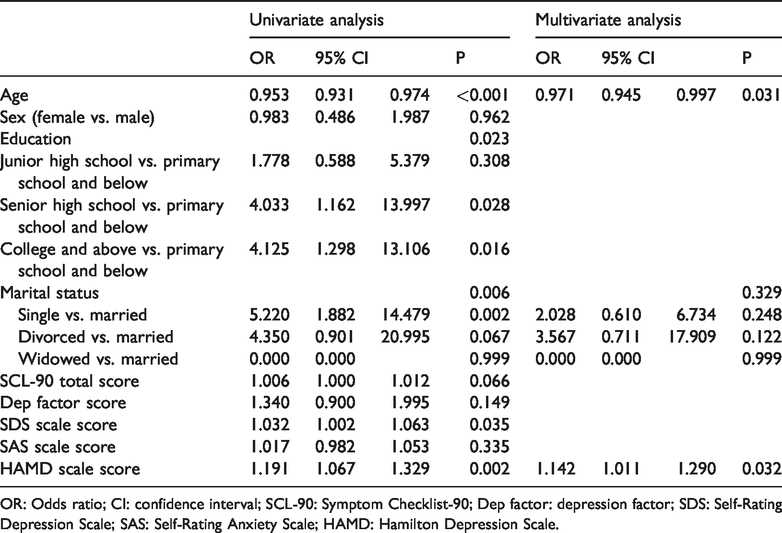
OR: Odds ratio; CI: confidence interval; SCL-90: Symptom Checklist-90; Dep factor: depression factor; SDS: Self-Rating Depression Scale; SAS: Self-Rating Anxiety Scale; HAMD: Hamilton Depression Scale.
Reasons for loss to follow-up
Table 4 presents the reasons for loss to follow-up. The main reasons given by patients were “I am worried about the side effects of the medicine” (33/96, 34.4%), “My depression is not a disease and cannot be resolved with medicine” (26/96, 27.1%), “Depression is a natural emotional reaction that does not require therapy” (21/96, 21.9%), and “The drug is effective and I do not need further treatment” (24/96, 25.0%).
Analysis of the reasons patients discontinue follow-up visits at different time points.

Reasons patients discontinued follow-up at different time points
As shown in Table 4, before and after week 2, 12.3% and 51.6% of patients, respectively, gave the reason for discontinuing follow-up as “The drug is effective and I do not need further treatment” (P < 0.001).
Discussion
In the present study, we aimed to understand the reasons behind outpatient loss to follow-up and the views of Chinese patients with depression regarding the disease diagnosis and antidepressant therapy. The results suggested that patients with high follow-up adherence were relatively older and had higher HAMD scores. Globally, the main reason for loss to follow-up was the fear of adverse effects and the belief that depression cannot or should not be cured using drugs. The main reason for loss to follow-up after 2 weeks of treatment for depression was the belief that the drug was effective and no longer needed.
Sawada et al. 23 reported that from the first visit to a doctor, the follow-up rate of people with depression was 72.5% at 1 month and 54.0% at 3 months. Vanelli et al. showed that 38.8% of patients who were not receiving antidepressant treatment stopped their follow-up within 30 days after their first visit to the hospital. In the present study, the follow-up rate at 4 weeks was 54.8% and 42.2% at 3 months, which is lower than in previous studies. This could be owing, at least in part, to Chinese cultural traditions in which family support has a very important role in disease management. In addition, depression is considered a shameful disease in China, and patients are often unwilling to seek help or consult with a physician. 24 Yau et al. 15 showed that 46% of patients were noncontinuous users when prescribed a new therapy. Lu et al. 25 showed that lower income, fewer than three episodes of depression, and anxiety were associated with better adherence.
Our results showed that patients who were lost to follow-up were younger than those in the follow-up group, which is supported by a previous study. 24 HAMD scale scores in the lost-to-follow-up group were higher, in contrast to the findings of Lee et al. 26 We found that a higher HAMD scale score results in more serious symptoms of depression and these patients are more likely to feel negatively toward therapy. Therefore, in this population, lower HAMD scores were globally associated with more positive attitudes, including attitudes toward therapy. Suicide and remission are other factors that can affect the loss to follow-up rate. Regarding the suicide rate, these data are unreliable because suicide is only recorded in the medical chart if the hospital is informed of the cause of death by the family; this results in considerable underreporting. During the study period, no patients were declared to be in remission and discharged by their physician. Therefore, those two factors did not affect the loss to follow-up rate observed here.
The most common reasons for loss to follow-up were cognitive reasons, i.e., misconceptions about depression and its treatment, as supported by the findings of a previous study. 27 Hung et al. 13 found that 19.3% of their patients did not agree with their diagnosis, 20.2% were worried about side effects, and 8.4% were not confident about medical therapy. By comparison, values for the corresponding reasons in the present study were 27.1%, 34.4%, and 13.5%, respectively. This suggests that in mainland China, insufficient information may be provided to the public about depression, and information dissemination regarding the disease may need further improvement. In China, most patients with depression are not treated according to the guidelines; they have short treatment courses and low treatment persistence. 12 Economic reasons can be a major factor for many Chinese patients, 12 but this was not the case in the present study as all patients were from the Shanghai urban area and had medical insurance. Yau et al. 15 showed that younger age, female sex, living in public housing, side effects, irregular follow-ups, and early-onset diagnosis were associated with treatment non-adherence. Therefore, the main reason affecting treatment is misconceptions about depression and antidepressants. This information should be provided to patients in the outpatient department at different time points, to correct cognitive biases and improve the rate of standardized treatment. With regard to education provided for patients, the following methods may be practical: (1) distribution of leaflets about treatments for depression, to inform the public about the availability of medical treatment; (2) increasing the number of follow-up phone calls to understand patients’ actual feelings or concerns about depression; and (3) organizing group activities to enable patients to exchange their views or feelings about their treatment. In this way, more appropriate guidance can be provided.28,29 Nevertheless, further studies are needed to determine the effectiveness of these educational tools and follow-up visits in improving medication adherence among patients with depression in China.
This study has some limitations. The study sample was from one hospital in Shanghai, and patients were assessed during 2012 to 2013. This study was conducted based on several scales, which might not be all-inclusive. The study only covered the first 3 months of treatment. Because of the retrospective nature of the study, many factors could not be evaluated, including compliance with medication. Losses to follow-up mostly occurred within 2 weeks from the first day of diagnosis. After 2 weeks, the sample size was relatively small for analysis. Patients who were lost to follow-up were contacted to assess the reasons for loss to follow-up; because they were told at their first visit that this would happen, most patients were cooperative but it is possible that some did not cooperate. The survey was not formally validated. In this study, we failed to examine the effects of different antidepressants on the follow-up rate, even though some studies have indicated that different antidepressant medications affect patients’ medication adherence. 23 In the present study, the assessors conducting the survey were blinded to treatments, which could partly overcome this limitation. Finally, not all factors were related to the patient; some factors were related to the physician and others to the patient–physician relationship. Nevertheless, in psychiatry, treatment of a patient often cannot be dissociated from the patient’s relationship with their physician.
In conclusion, patients with high follow-up adherence were relatively older and had higher HAMD scores. Globally, the main reason for loss to follow-up was fear of adverse effects and the belief that depression cannot or should not be cured using drugs. The main reason for loss to follow-up after 2 weeks of treatment for depression was feeling that the drug was effective and no longer needed.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This paper was supported by a Shanghai Municipal Health Bureau’s Subject (Subject title: An investigation on reasons for outpatient depression patient’s dropout and an evaluation of interventions targeted to control the dropout rate. Subject code: 20134147).