
Abstract
Objective
We evaluated clinical performance of the T-SPOT.TB test for detecting tuberculosis (TB) infection in Meizhou, China.
Methods
We enrolled 2,868 patients who underwent T-SPOT.TB, smear, and TB-DNA at the same time. The tests’ sensitivity and specificity were evaluated and compared in different groups, and in pulmonary TB (PTB) and extrapulmonary TB (EPTB) subgroups. Receiver operator characteristic (ROC) curve analysis was used to evaluate T-SPOT.TB’s diagnostic value and determine its cutoff value.
Results
T-SPOT.TB, TB-DNA, and sputum smear sensitivity was 61.44%, 37.12%, and 14.02%; and specificity was 76.49%, 99.20% and 99.60%, respectively. The T-SPOT.TB positive rate was higher in the PTB and EPTB subgroups than in patients with other pulmonary diseases (61.38% and 61.76% vs. 23.34%). The T-SPOT.TB test had better diagnostic accuracy and sensitivity when the positive cutoff value of marker ESAT-6 was 2.5 [area under ROC curve = 0.701, 95%CI 0.687–0.715] and marker CFP-10 was 6.5 [area under ROC curve = 0.669, 95%CI 0.655–0.683].
Conclusion
T-SPOT.TB sensitivity was higher than that of TB-DNA or sputum smear, but the specificity was lower. T-SPOT.TB had moderate sensitivity and specificity for diagnosing TB. T-SPOT.TB’s new positive cutoff value may be clinically valuable according to ROC analysis.
Introduction
Tuberculosis (TB) is a major risk to human health security in the world.1,2 Worldwide, TB infects millions of people every year and is one of the most common infectious diseases leading to death.3–5 Overall, 90% of cases are adults (age ≥15 years) and two-thirds are in southern Africa and Southeast Asia, including China. 6
Clinically, the diagnosis of TB is based on clinical and radiographic characteristics and on microbial or pathological evidence.7,8 Sputum smear microscopic examination is one of the most common and simplest methods to diagnose pulmonary TB. This method is quick and easy, but its sensitivity is low.9–11 In clinical practice, culture to detect the causative pathogen, Mycobacterium tuberculosis, is the reference standard for TB diagnosis. 12 However, culture has high requirements for technical skill of operators, and it takes 4 to 8 weeks for detection of the pathogen.
With progress in the study of the Mycobacterium tuberculosis genome and the human host response, new diagnostic tests for TB have been developed. Early secretory antigenic target-6 (ESAT-6) and culture filtrate protein 10 (CFP-10) are secreted antigens encoded by region of deletion 1 (RD1) of Mycobacterium tuberculosis.13–16 The T-SPOT.TB test stimulates T cells to secrete cytokines in vitro by using ESAT-6 and CFP-10 as specific antigens, and the results are examined using the enzyme-linked immunospot (ELISpot) method.17,18
Studies have indicated that the T-SPOT.TB test may be a more accurate method compared with culture and sputum smear for detecting suspected latent TB19–21 and active TB22–24 infections. Some studies have explored the clinical diagnostic value and limitations of T-SPOT.TB in areas with a high incidence of TB in China through stratification and comparative analysis.25–27 Meizhou is located in northeast Guangdong Province, and most of its residents are Hakka Chinese people. 28 In this study, we aimed to study the clinical performance of sputum smear microscopy, T-SPOT.TB, and TB-DNA analysis for detection of TB infection in Meizhou, China.
Materials and methods
Study subjects
This retrospective study was approved by Human Ethics Committees of Meizhou People’s Hospital (Huangtang Hospital), Meizhou Academy of Medical Sciences, Meizhou Hospital Affiliated to Sun Yat-sen University, Guangdong Province, China (approval number: 2016-4-33).
Prior to sample collection, written informed consent was obtained from the patients or their guardians, and patient/participant privacy was carefully protected.
We enrolled 2,868 participants who simultaneously underwent T-SPOT.TB, sputum smear, and TB-DNA between May 2016 and October 2018. These patients and volunteers were classified into pulmonary TB (PTB) (n = 813) and extrapulmonary TB (EPTB) subgroups (n = 170) and a control group (n = 1,885) of hospitalized patients without TB infection. Patients were diagnosed as having TB infection based on auxiliary examinations (bacteriological examination, chest radiography, chest computed tomography, pleural biopsy, electronic bronchoscopy, pathological examination), medical history, and clinical manifestations.
The sensitivity and specificity of the three tests was evaluated and compared in different groups and subgroups. Receiver operator characteristic (ROC) curve analysis was used to evaluate the diagnostic value of T-SPOT.TB and to determine cutoff values for T-SPOT.TB.
T-SPOT.TB test
A peripheral venous blood sample of about 6 mL was collected from participants and placed in a test tube of heparin anticoagulant. Peripheral blood mononuclear cells were isolated within 4 hours using Lymphocyte Separation Medium (MD Pacific Biotechnology Co. Ltd., Tianjin, China). The T-SPOT.TB test was performed according to the instructions of the kit (Oxford Immunotec Ltd., Abingdon, UK). In brief, the peripheral blood mononuclear cells were added to 96-well plates precoated with anti-IFN-γ antibody. Plates were incubated for 16 to 20 hours at 37°C with 5% CO2, washed with phosphate-buffered saline, and developed using an anti-IFN-γ antibody conjugate and substrate to detect the presence of secreted IFN-γ. Spot-forming cells (SFCs) were counted with an automated spot reader. The criteria for a negative test were as follows: the number of spots ranged from 0 to 5. The criteria for a positive test were as follows: (1) the number of spots in negative control holes was ≥6 and the number of spots in detection holes was ≥2 times the number of spots in negative control holes; (2) the number of detection holes in antigen A and B minus the number of negative holes was ≥6. If either or both ESAT-6 and CFP-10 were positive, the results were read as positive.
Sputum smear test
A sputum sample was collected in a clean container in the morning and smeared on a slide. The smear was naturally dried and fixed, stained with carbol-fuchsin solution for 5 minutes, washed with water, decolorized with acid alcohol solution for 1 to 2 minutes, washed with water, stained with methylene blue solution for 30 seconds, washed, and dried. After staining, the slide was placed under a microscope for observation and counting. The result was positive for TB when >3 acid-fast bacilli were found in every 100 fields of view under the microscope.
TB-DNA test in sputum and blood
These specimens included sputum and blood. TB DNA was detected by real-time fluorescence quantitative PCR (DAAN Gene Co. Ltd., Guangzhou, China). The kit had a detection limit of 5.0 × 102 copies per mL and a linear range of 5.0 × 102 to 5.0 × 108 copies per mL. Target DNA detected by real-time TaqMan PCR with the LightCycler 480 real-time PCR system (Roche Diagnostics, Mannheim, Germany). The PCR for detection of TB DNA was performed as follows: initial denaturation at 93°C for 2 minutes and 10 cycles of first round of amplification (45 seconds at 93°C, 1 minute at 55°C), followed by 30 cycles of the second round of amplification (30 seconds at 93°C, 45 seconds at 55°C). The fluorescence signals were collected at elongation in the second round of amplification.
TB-DNA test in formalin-fixed and paraffin-embedded slices
Formalin-fixed and paraffin-embedded slices included lung biopsy samples, lymph node biopsy samples, and gastrointestinal tissue samples. After the formalin-fixed and paraffin-embedded slices were deparaffinized, DNA was extracted using AmoyDx Tissue DNA Kit according to the manufacturer’s instructions (Spin Column; Amoy Diagnostics, Xiamen, China). After the quantity and quality of DNA were determined by NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA) to meet the requirements, the DNA was stored at −20°C until use. The TB-DNA test was carried out according to the manufacturer’s protocol for TB-DNA PCR Kit (DAAN Gene Co. Ltd.) with the LightCycler 480 system.
C-reactive protein
An immunochemical method was used to detect C-reactive protein (CRP), and specific anti-CRP antibody was used to react with and determine the CRP content of the samples tested according to the results of immune response. The reference range of CRP is 0 to 6 mg/L; a value >6 mg/L indicates an increase in CRP.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation and analyzed by ANOVA between groups. The chi-square test was used for the comparison of rates of positive cases, sensitivity, and specificity. P < 0.05 was considered statistically significant.
Results
Study subjects
This retrospective analysis was conducted on 2,868 cases who underwent the T-SPOT.TB, sputum smear, and TB-DNA tests at the same time; participants were aged from 3 months to 98 years. The participants included 2,161 (75.35%) males and 707 (24.65%) females, with a mean age of 63.74 ± 16.85 and 57.95 ± 21.03 years in males and females, respectively. The CRP value of the pulmonary TB patients was lower than that of patients with extrapulmonary TB or other pulmonary diseases (P < 0.001). The information of participants is shown in Table 1.
Clinical characteristics of study participants.

TB, tuberculosis; CRP, C-reactive protein.
Results of T-SPOT.TB, smear, and TB-DNA tests
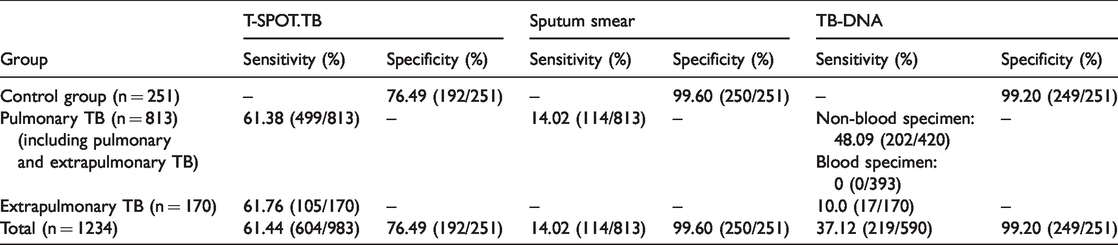
The sensitivity and specificity of the three methods were compared in 1,234 patients who were tested for T-SPOT.TB, sputum smear, and TB-DNA at the same time. The sensitivity of T-SPOT.TB, sputum smear, and TB-DNA was 61.44%, 14.02%, and 37.12%, and the specificity was 76.49%, 99.60%, and 99.20%, respectively. The sensitivity of T-SPOT.TB was higher than that of TB-DNA and sputum smears in patients with PTB and EPTB. Among patients with PTB (n = 813), 499 had a positive T-SPOT.TB and the sensitivity was 61.38%. Among patients with EPTB, 105 of 170 had a positive T-SPOT.TB and the sensitivity was 61.76%, similar to that of the PTB group. The overall sensitivity of T-SPOT.TB in patients with TB (the PTB and EPTB groups) was 61.44% (604/983). Among 251 patients who did not have TB (control group), specificity was 76.49% (192/251), with negative results in 192 controls (Table 2).
Sensitivity and specificity (%) of T-SPOT.TB, sputum smear, and TB-DNA for tuberculosis-infected subjects.
T-SPOT.TB distributions of sex, age, and subgroup
The positive rates of T-SPOT.TB in the PTB and EPTB groups were significantly higher than those of patients with other pulmonary diseases (61.38% and 61.76% vs. 23.34%, respectively; P < 0.001). The results of the subgroup analysis are shown in Table 3.
The distribution of ESAT-6 and CFP-10 in males and females in different groups.

ESAT-6, early secretory antigenic target-6; CFP-10, culture filtrate protein 10; TB, tuberculosis.
There was no significant difference in ESAT-6- and CFP-10-specific T-cell frequencies between males and females in the PTB, EPTB, and other pulmonary diseases groups. The mean counts of ESAT-6 for T-SPOT.TB were 9.12 ± 20.51 and 8.62 ± 20.08 SFCs in males and females, respectively. The mean counts of CFP-10 were 9.74 ± 25.69 and 9.34 ± 26.16 SFCs in males and females, respectively. The number of spots for ESAT-6 and CFP-10 decreased with increasing age of patients (Figure 1).
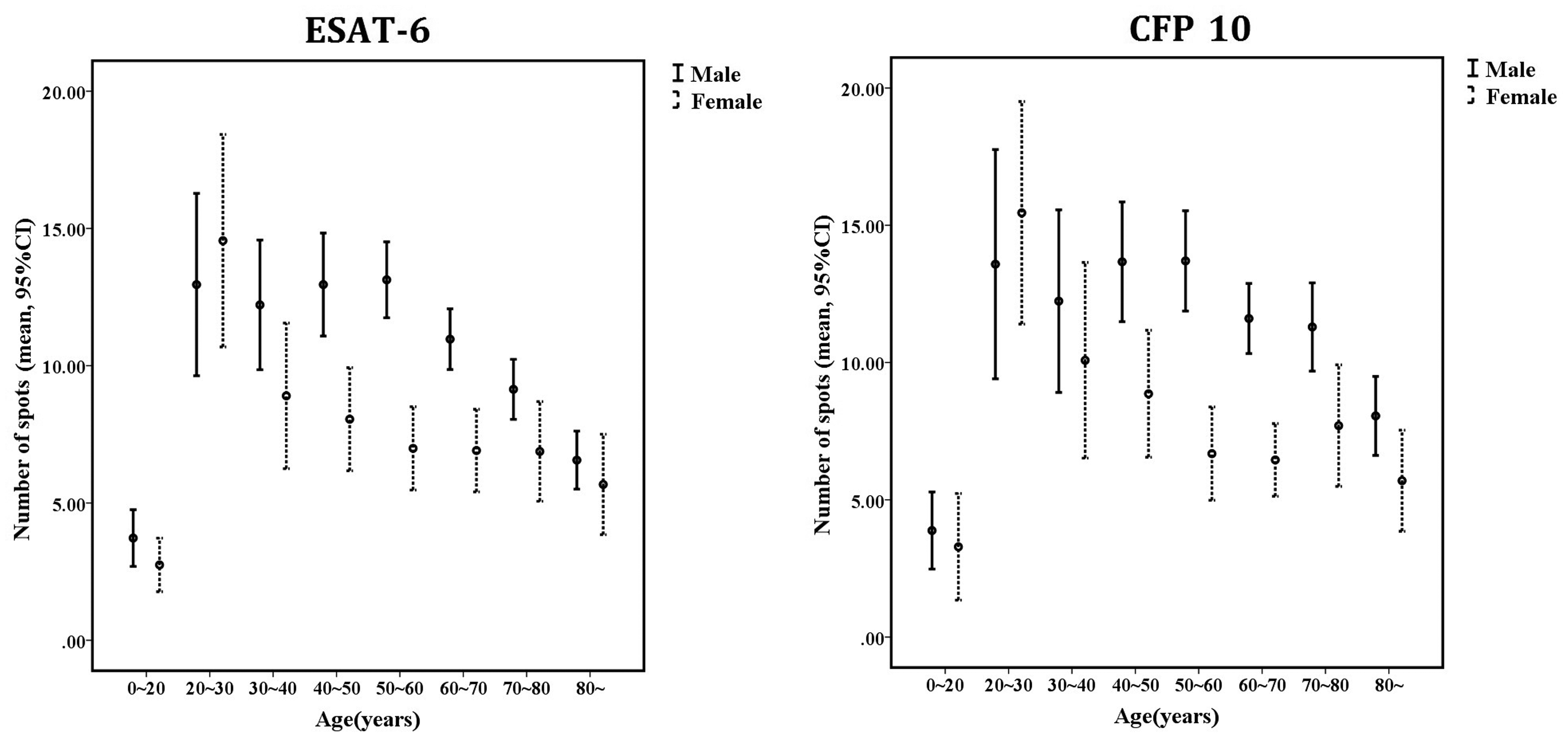
The net spot number of ESAT-6 (left) and CFP-10 (right) in different age groups. The net spot numbers of ESAT-6 and CFP-10 were calculated by subtracting the background spot number in negative control wells from the spot number in ESAT-6/CFP-10 wells. The net spot number was expressed as the mean with 95% confidence intervals in different age groups. Black circles represent the means and error bars represent 95% confidence intervals.
ROC analysis of T-SPOT.TB
The area under the ROC curve (AUROC) was used to evaluate diagnostic value. The T-SPOT.TB test had better diagnostic accuracy and sensitivity when the positive cutoff value of ESAT-6 was 2.5 (AUROC = 0.701, 95% CI 0.687–0.715) and that of CFP-10 was 6.5 (AUROC = 0.669, 95% CI 0.655–0.683). These new positive cutoff values of the T-SPOT.TB may be clinically valuable (Figure 2).

Receiver operating characteristic (ROC) curve analysis of T-SPOT.TB test for diagnosing tuberculosis
Discussion
Mycobacterium tuberculosis can invade many organs in the body, but most commonly infects the lungs. Currently, the cure rate of tuberculosis is improving, but long-term use of drugs can lead to drug resistance. The most reliable method to achieve a cure is early detection and treatment. Culture is the gold standard for tuberculosis diagnosis, but routine culture takes a long time because of the effect of bacterial content of samples and the culture cycle. 29 However, sputum smear cannot be used to diagnose extrapulmonary tuberculosis, and it cannot be used to effectively differentiate non-tuberculous Mycobacterium or dead tuberculosis bacteria. Thus, this method has low application value. Clinically, the diagnosis of tuberculosis patients depends mainly on clinical manifestations, imaging changes, and response to anti-tuberculosis drugs.30,31 When the body is infected with Mycobacterium tuberculosis, specific effector T lymphocytes are detectable in vivo. The T-SPOT.TB test can detect latent infections of Mycobacterium tuberculosis and assist in early diagnosis.
The sensitivity and specificity of diagnosing TB using T-SPOT.TB in the current study were 61.44% and 76.49%, lower than values reported by Qiu et al. (78.2% and 91.1%) 32 and by Wang et al. (85% and 85.1%). 33 The positivity rate of T-SPOT.TB was 18.9% in rural China according to a multicenter epidemiological study. 34 In this study, the number of spots responding to ESAT-6 and CFP-10 decreased with age, in contrast to the results of Hu et al. in a study conducted in Shanghai, China. 35 This may be related to differences in the populations studied, and because a large number of samples must be tested to study the relationship between ESAT-6, CFP-10, and age. The positive rates of T-SPOT.TB in the PTB and EPTB groups were significantly higher than that in patients with other pulmonary diseases. The sensitivity of TB-DNA in the PTB group was significantly higher than that of the EPTB group. Compared with TB-DNA, T-SPOT.TB had higher sensitivity for the diagnosis of EPTB.
The sensitivity of T-SPOT.TB was significantly higher than that of sputum smear or TB-DNA. The T-SPOT.TB test has been used in the detection of Mycobacterium tuberculosis infection for many years and has achieved a good clinical effect; the test does not rely on the patient shedding bacteria or on the type or quantity of bacteria shed. The T-SPOT.TB method allows for fast detection of TB and high accuracy, which is important in the accurate and efficient diagnosis of TB. Therefore, T-SPOT.TB is an effective test method for early diagnosis of tuberculosis.
This study had some limitations. The numbers of participants with latent TB infection was small, which may result in low validation of the evidence. Additionally, because there is no gold standard method for diagnosis of latent TB, we could not evaluate the performance of T-SPOT.TB for the diagnosis of latent TB infection.
T-SPOT.TB detection is a sensitive and specific method, but it cannot distinguish active from latent TB infection. The consistency of results from T-SPOT.TB with those of acid-fast smear, direct sputum smear, or TB-DNA was low. The diagnostic value of T-SPOT.TB method should be evaluated in further studies.
Conclusions
The positive rate of diagnosis using the T-SPOT.TB test in patients with pulmonary and extrapulmonary TB was significantly higher than that in other patient groups. The sensitivity of T-SPOT.TB was higher than that of TB-DNA or sputum smear, but the specificity was lower. According to our ROC analysis, new positive cutoff values of the T-SPOT.TB test may make the test more clinically valuable.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520923534 - Supplemental material for Clinical evaluation of the T-SPOT.TB test for detection of tuberculosis infection in northeastern Guangdong Province, China
Supplemental material, sj-pdf-1-imr-10.1177_0300060520923534 for Clinical evaluation of the T-SPOT.TB test for detection of tuberculosis infection in northeastern Guangdong Province, China by Hua Zhong, Heming Wu, Zhikang Yu, Qunji Zhang and Qingyan Huang in Journal of International Medical Research
Footnotes
Author Contributions
Heming Wu conceived and designed the experiments. Hua Zhong, Qunji Zhang, Qingyan Huang and Zhikang Yu recruited subjects and collected clinical data. Heming Wu and Zhikang Yu conducted the laboratory testing. Zhikang Yu and Hua Zhong helped to analyze the data. Heming Wu and Hua Zhong prepared the manuscript. Heming Wu reviewed the manuscript.
Acknowledgements
The authors would like to thank colleagues of the Center for Precision Medicine, Meizhou People’s Hospital (Huangtang Hospital), Meizhou Hospital Affiliated to Sun Yat-sen University for their helpful comments on the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by Science and Technology Planning Program of Meizhou City, Guangdong Province, China (Grant No.: 2015B037 to Dr. Hua Zhong).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.