
Abstract
Objective
To investigate the effectiveness of combining the 8-isoprostane and nitric oxide (NO) levels in exhaled breath condensate (EBC) with the clinical pulmonary infection score (CPIS) to assess ventilator-associated pneumonia (VAP) in patients on mechanical ventilation.
Methods
Thirty-two patients with VAP served as the observation group and 32 patients without VAP served as the control group. The correlations of 8-isoprostane and NO levels in EBC with CPIS, chest X-ray score, oxygenation index, and lung injury score (LIS) were analyzed. The area under the curve (AUC) was compared with experimental data using the receiver operating characteristic curve (ROC) to predict VAP.
Results
The 8-isoprostane and NO levels in EBC of VAP patients on mechanical ventilation were positively correlated with CPIS, chest X-ray score, and LIS, but negatively correlated with oxygenation index. The AUC of simplified CPIS combined with 8-isoprostane and NO levels in EBC for predicting VAP was 0.914, which suggests that this is a highly effective for making a diagnosis.
Conclusions
The simplified CPIS combined with the 8-isoprostane and NO levels in EBC of patients on mechanical ventilation is effective for evaluating and diagnosing VAP. 8-Isoprostane and NO levels in EBC could be used as biomarkers to evaluate VAP.
Keywords
Introduction
Ventilator-associated pneumonia (VAP) is defined as pneumonia that occurs 48 hours after mechanical ventilation and 48 hours after withdrawal or extubation in patients with tracheal intubation or tracheotomy. Ten to twenty percent of patients who receive invasive mechanical ventilation have VAP, 1 which is a common and serious complication that is related to mechanical ventilation in the intensive care unit (ICU). The diagnosis is mainly based on clinical manifestations, laboratory data, imaging changes, and etiological diagnosis. However, the acquisition of these data is often delayed, and thus, early diagnosis and monitoring of VAP are difficult.
To improve the diagnostic efficiency of VAP, researchers tried to identify serum biomarkers that were related to infection, such as C-reactive protein and procalcitonin,2–4 while less attention has been paid to the biomarkers in exhaled breath condensate (EBC). EBC is formed by the lower airway lining fluid, and it contains many potential biomarkers. By analyzing EBC, we can directly monitor pulmonary oxidative stress and inflammation under mechanical ventilation. This method is safe, non-invasive, repeatable, and especially suitable for critical patients on mechanical ventilation. 5 In this study, we measured the 8-isoprostane and nitric oxide (NO) levels in EBC of VAP patients on mechanical ventilation and investigated the effectiveness of combining their levels with other clinical measurements in the diagnosis of VAP. We found that combining 8-isoprostane and NO levels in EBC with clinical pulmonary infection score (CPIS) is effective in diagnosing patients with VAP.
Material and methods
Sample size estimation
We set α equal to 0.05 and β equal to 0.8, and the AUC was estimated to be 0.8 and 0.9. Power analysis and sample size (PASS; www.ncss.com/software/pass) was used to calculate the sample size. The results were as follows: the overall sample size was 56; the sample size for the VAP-positive group was 28; and the sample size for the VAP-negative group was 28. Based on 10% missing visits, the overall sample size was 64, with 32 patients per group.
Subjects
A cross-sectional study was conducted with 64 patients on mechanical ventilation in the ICU. There were 32 patients in the VAP group. A VAP diagnosis was based on the American CDC-NHSN 2013 “Ventilator-Associated Pneumonia Event” standard, 6 as follows: met the diagnostic criteria for pneumonia, where the patient is on mechanical ventilation for >2 calendar days on the date of the event, with Day 1 as the day of the ventilator placement, and the ventilator had been in place on the date of the event or the day before. Pneumonia was diagnosed based on the following criteria for more than one specific site during the infection window period: (1) Two or more serial chest imaging test results with at least one of the following: 1) New and persistent or progressive and persistent infiltration; 2) consolidation; or 3) cavitation; (2) At least one of the following: 1) fever (>38.0°C); 2) leukopenia (white blood cells [WBCs] <4 × 109/L) or leukocytosis (WBC >12 × 109/L); or 3) for adults >70 years old, altered mental status with no other recognized cause; and (3) At least two of the following: 1) New onset of purulent sputum or change in the character of the sputum, increased respiratory secretions, or increased suctioning requirements; 2) New onset or worsening cough, dyspnea, or tachypnea; 3) Rales or bronchial breath sounds; or 4) Worsening gas exchange (for example: O2 desaturations such as PaO2/FiO2 < 240), increased oxygen requirements, or increased ventilatory demand, together with laboratory evidence such as bacteria or fungal pathogens based on a clinical diagnosis of pneumonia.
There were 32 patients in the non-VAP group, and these patients were on mechanical ventilation, but during the same period, these patients did not meet the clinical standard for VAP. Exclusion criteria included severe bacterial or fungal pulmonary infections that were identified at admission, and patients who were on mechanical ventilation for less than 5 days.
This clinical study was approved by the hospital ethics committee. All patients provided written informed consent.
Methods
Samples collection and measurement
Samples were collected on days 5 and 6 of mechanical ventilation. Before EBC collection, the ventilator pipe was replaced with a dry threaded pipe, and the humidifier was not connected. The improved EcoScreen condenser (Eric Jaeger, Würzburg, Germany) was connected in series at the exhaust end of the ventilator pipe. About 2 mL of EBC specimens were collected every 20 minutes. 7 The environment of the ICU was controlled at 20 to 25°C and kept below 45% to 50% humidity. The microorganism samples from the respiratory tract were collected using bronchoalveolar lavage, and the samples were collected and qualitatively cultured twice. Bacterial culture was determined to be positive when the bacterial concentration in alveolar lavage fluid was ≥104 cfu/mL.
The enzyme immunoassay (EIA) enzyme labeling method (Cayman Company, Ann Arbor, MI, USA) was used to determine 8-isoprostane. NO was determined using the colorimetry method (BioVision Research Products Company, Milpitas, CA, USA).
Clinical assessment
The following clinical indicators were observed: (1) Arterial blood gas analysis was conducted within 2 hours before and after specimen collection, and 1 mL of arterial blood (radial artery, femoral artery, or dorsal pedal artery) was collected and measured within 1 minute; (2) Simplified CPIS score, 8 which included body temperature (0–2 points), WBC count (0–2 points), characteristics and quantity of aspirates (0–2 points), oxygenation index (PaO2/FiO2 points), and chest X-ray infiltration (0–2 points). The maximum total score was 10. The simplified CPIS system did not include the semi-quantitative culture of the airway secretions, which simplified the assessment of airway secretions for clinical application; and (3) Lung injury score (LIS), 9 which included the chest X-ray score, oxygenation index, positive end-expiratory pressure, and lung compliance.
Statistical methods
Statistical analysis was performed using MedCalc 15.0 (MedCalc Software Ltd, Ostend, Belgium). Measured data were expressed as the mean ± standard deviation (SD). Intergroup comparisons were performed using a t-test or non-parametric Mann–Whitney U-test. Correlation analysis was performed by Pearson’s or Spearman’s correlation. The predictive power of the detection method was determined using the receiver operating characteristics (ROC) curve, and the probabilistic predictive power was calculated using binary logistic regression combined with multivariate regression. ROC curve analysis was then performed. The predictive power was low when the area of the ROC curve was 0.5 to 0.7, medium when the area of the ROC curve was 0.7 to 0.9, and high when the area of the ROC curve was >0.9. 10 The χ2 test was used for AUC comparison. P < 0.05 was considered to be statistically significant.
Results
Patients
Sixty-four patients were enrolled into the study, with 32 patients per group. In the VAP group, there were 20 males and 12 females, with an average age of 60.9 ± 16.6 years (range, 23 to 85 years). In the non-VAP group, there were 22 males and 10 females, with an average age of 60.9 ± 16.6 years (range, 23 to 85 years).
General clinical data
A total of 110 bacterial isolates were detected in 32 patients with VAP. Among them, the 48 (43.6%) isolates of Gram-negative bacilli were mainly Acinetobacter baumannii, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Escherichia coli. The 43 (39.1%) isolates of Gram-positive cocci were mainly Staphylococcus aureus, Staphylococcus epidermidis, and Staphylococcus hemolyticus. The 19 (17.3%) isolates of fungi were mainly Candida albicans (Table 1).
Composition of pathogenic bacteria in patients with VAP.

VAP, ventilator-associated pneumonia.
8-Isoprostane and NO levels in EBC and clinical indicators in the two groups
The elevated 8-isoprostane and NO levels in EBC from 64 patients on mechanical ventilation were positively correlated with the CPIS (r = 0.468; P < 0.05), LIS (r = 0.335; P < 0.05), and chest X-ray scores (r = 0.279; P < 0.05) and were negatively correlated with the oxygenation index (r = −0.285; P < 0.05) (Table 2).
Correlation between 8-isoprostane and NO levels in EBC of patients undergoing mechanical ventilation and clinical indicators.

NO, nitic oxide; WBC, white blood cell; EBC, exhaled breath condensate; CPIS, clinical pulmonary infection score; LIS, lung injury score; N.S., not significant.
Further analysis showed that the 8-isoprostane and NO levels in EBC, CPIS, LIS, chest X-ray scores, and oxygenation index in the VAP group were significantly higher compared with the non-VAP group (P < 0.05 for all). There was no significant difference in the WBC count between the two groups (Table 3).
Comparison of EBC and clinical indicators of VAP and non-VAP group.
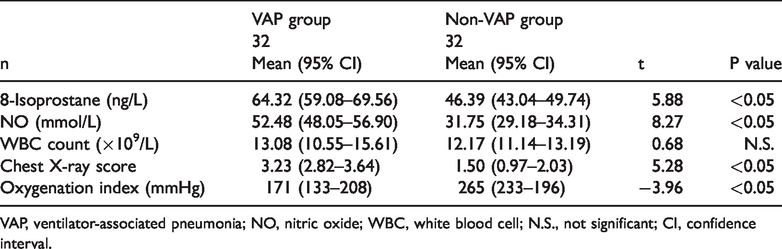
VAP, ventilator-associated pneumonia; NO, nitric oxide; WBC, white blood cell; N.S., not significant; CI, confidence interval.
The ROC curve in evaluating the diagnostic effectiveness of each VAP detection index
The ROC curves of CPIS, 8-isoprostane, NO, CPIS + 8-isoprostane, CPIS + NO, and CPIS + 8-isoprostane + NO to predict VAP were analyzed (Table 4). For CPIS, the sensitivity and specificity were 71.87% and 90.62%, respectively, with a positive threshold of ≥5; for 8-isoprostane, the sensitivity and specificity were 93.75% and 71.87%, respectively, with a positive threshold of ≥54 ng/L; and for NO, the sensitivity and specificity were 56.25% and 96.87%, respectively, with a positive threshold ≥40 mmol/L. For the combined multiple indices, the AUC predicted by CPIS + 8-isoprostane + NO for VAP was 0.914, and the diagnostic power was the highest compared with the other single and multiple indexes (Table 4). The positive threshold of the combined prediction probability was ≥0.44, and the sensitivity and specificity were 90.00% and 87.50%.
Predictive power of 8-isopronstane and NO in CPIS and EBC for predicting VAP.

NO, nitic oxide; CPIS, clinical pulmonary infection score; EBC, exhaled breath condensate; VAP, ventilator-associated pneumonia; AUC, area under the curve; CI, confidence interval; SE, standard error.
The AUC of CPIS+8-isoprostane+NO and CPIS was plotted and calculated. The difference between the AUC was 0.0869, and the 95% confidence interval was 0.016 to 0.157. The Z statistic value was 2.431 (P < 0.05), suggesting that the difference was statistically significant (Figure 1).

Comparison of ROC curves, with a difference in AUC of 0.0869 and a Z score of 2.431 (P < 0.05).
Discussion
Timely and accurate evaluation of VAP during mechanical ventilation is essential for a better patient prognosis. However, the sensitivity and specificity of the clinical criteria for diagnosing VAP are low. Studies have shown that CPIS is helpful for diagnosing VAP, but the diagnostic effectiveness is moderate. 11 In recent years, biomarkers in EBC were found to be helpful in evaluating VAP.12–14 This study showed that the 8-isoprostane and NO levels in the EBC from VAP patients were significantly higher compared with non-VAP patients during mechanical ventilation, and the increase was correlated with the severity of the pulmonary infection. Simplified CPIS combined with 8-isoprostane and NO levels in EBC increased the AUC for predicting VAP, which improved the effectiveness of VAP assessment.
Elevated 8-isoprostane and NO levels in EBC may reflect the severity of pulmonary infection in patients on mechanical ventilation. 8-Isoprostane is a new group of prostaglandins. Hypoxia can activate phosphatidic acid A2 to hydrolyze phospholipids on the cell membrane and to release arachidonic acid. It may also activate phospholipase C, which can decompose inositol triphosphate and release arachidonic acid. It is produced by a non-cyclooxygenase pathway. As an inflammatory medium, its concentration increases during oxidative stress, but it is stable in vivo under normal conditions. It is a reliable indicator of lipid peroxidation and oxidative stress response. 15 NO is produced from L-arginine, which is catalyzed by NO synthase in vivo. Cytokines are produced in large quantities during the pulmonary inflammatory response, which induces the increase of NO synthase synthesis in alveolar macrophages, neutrophils, and airway epithelial cells, and leads to increased NO production. 16 Recently, 8-isoprostane and NO have been widely studied as airway biomarkers for oxidative stress and inflammation in the lungs, which can be detected reliably in EBC. The elevation of 8-isoprostane and NO can be detected in the EBC of patients with bronchial asthma,17,18 chronic obstructive pulmonary disease, 19 acute respiratory distress syndrome (ARDS),20,21 and other pulmonary diseases, which are closely related to the severity of the respiratory function injury. This study showed that 8-isoprostane and NO levels in EBC of VAP patients were significantly increased, and that the CPIS, oxygenation index, LIS, and chest X-ray score correlated with lung lesion deterioration, suggesting that 8-isoprostane and NO levels in EBC were related to the severity of pulmonary infection, and that they could be used as biomarkers of pulmonary infection in VAP patients.
Simplified CPIS combined with 8-isoprostane and NO levels in EBC can improve the diagnostic effectiveness of VAP. The CPIS was proposed by the American Thoracic Association (ATS) and the Infectious Diseases Association in their VAP guidelines as a factor that can evaluate the degree of pulmonary infection objectively and comprehensively. However, there are limitations to the clinical implementation, for the following two reasons: the change in the chest imaging could be delayed compared with the clinical conditions, and repeated chest imaging is difficult; and etiological diagnosis needs 3 to 5 days. Thus, dynamic assessment of VAP is difficult. Simplified CPIS does not require etiological results of pulmonary infection, but its diagnostic efficiency may be lower compared with CPIS. Recently, researchers found that the combination of procalcitonin and CPIS can improve the diagnostic efficiency of VAP. 22 However, serum procalcitonin is not a specific indicator of pulmonary infection. Serum inflammatory markers are more responsive to systemic infection. Similarly, Table 2 shows that the peripheral WBC count does not effectively differentiate between VAP and non-VAP. EBC inflammation factors mainly originate from lung airway lining fluid, but they may just reflect the changes in lung inflammation, which is different from serum indicators that have a higher specificity. The combined CPIS score can better evaluate pulmonary infection and improve the diagnosis of VAP together with the patient’s medical history. This study demonstrated that the AUC of simplified CPIS for predicting VAP was 0.827, and the simplified CPIS combining with 8-isoprostane and NO levels in EBC increased the AUC to 0.914 for predicting VAP. The difference was statistically significant, and an AUC of >0.9 is a more effective clinical diagnostic value.
A limitation of this study is that the biomarkers in EBC are not specific biomarkers for infection. Biological factors in EBC can reflect pulmonary inflammation and oxidative stress, but the etiology may be pulmonary infection23,24 or non-infectious factors such as asthma, ARDS, and other pulmonary inflammatory damage. Currently, there is no evidence that a biochemical factor in EBC can be used as an infectious biomarker with a high specificity and sensitivity. This study showed that the elevation of 8-isoprostane and NO levels in EBC was positively correlated with CPIS and LIS in all mechanical ventilation patients, regardless if the patient had VAP, and it was associated with worsening of the disease. VAP can be combined with lung parenchymal cell injury, and the interpretation of EBC results needs to be combined with clinical evidence. EBC detection is safe and feasible for mechanical ventilation patients, 25 and it can be repeated at any time. The detection of biomarkers in EBC is different from serum detection in clinical significance and provides a new way to study the mechanism of pulmonary inflammation in critical patients who are on mechanical ventilation.
In conclusion, the elevated 8-isoprostane and NO levels in EBC reflect the severity of pulmonary infection in patients on mechanical ventilation. The simplified CPIS is helpful to diagnose and assess patients with VAP. 8-Isoprostane and NO levels in EBC can serve as a biomarker for VAP assessment. EBC detection technology can be used to monitor pulmonary inflammation in patients on mechanical ventilation and provide a new approach to assess VAP.