
Abstract
Objective
Measurement of positive end-expiratory pressure (PEEP)-induced recruitment lung volume using passive spirometry is based on the assumption that the functional residual capacity (FRC) is not modified by the PEEP changes. We aimed to investigate the influence of PEEP on FRC in different models of acute respiratory distress syndrome (ARDS).
Methods
A randomized crossover study was performed in 12 pigs. Pulmonary (n = 6) and extra-pulmonary (n = 6) ARDS models were established using an alveolar instillation of hydrochloric acid and a right atrium injection of oleic acid, respectively. Low (5 cmH2O) and high (15 cmH2O) PEEP were randomly applied in each animal. FRC and recruitment volume were determined using the nitrogen wash-in/wash-out technique and release maneuver.
Results
FRC was not significantly different between the two PEEP levels in either pulmonary ARDS (299 ± 92 mL and 309 ± 130 mL at 5 and 15 cmH2O, respectively) or extra-pulmonary ARDS (305 ± 143 mL and 328 ± 197 mL at 5 and 15 cmH2O, respectively). The recruitment volume was not significantly different between the two models (pulmonary, 341 ± 100 mL; extra-pulmonary, 351 ± 170 mL).
Conclusions
PEEP did not influence FRC in either the pulmonary or extra-pulmonary ARDS pig model.
Keywords
Introduction
The use of positive end-expiratory pressure (PEEP) is a routine practice in mechanically ventilated patients with acute respiratory distress syndrome (ARDS). The net effect of PEEP in certain patients may depend on recruitability,1,2 which has demonstrated extreme variability in ARDS patients and a significant correlation with the response to PEEP. 1 An estimation of the recruitment volume may be the first step for the individualized setting of PEEP in ARDS patients. 3
Recruitment volume can be easily measured at the bedside by quasi-static respiratory system pressure–volume (P–V) curves using passive spirometry. 4 This technique can be further simplified by measuring the difference between the real and the minimal predicted increase in lung volume induced by PEEP. 5 These measurements are based on the assumption that the functional residual capacity (FRC), which is also called the end-expiratory lung volume (EELV) during mechanical ventilation without the application of PEEP,6,7 is not modified by PEEP changes.5,8 To date, a few studies have reported various methods to measure the lung volume related to the impact of PEEP on FRC, but the results were contradictory.5,8,9 Using respiratory inductive plethysmography, Valta et al. 8 identified the same EELV after expiration from different PEEP levels in ARDS patients. Dellamonica et al. 5 also confirmed the same FRC at either 5 or 15 cmH2O of PEEP using a nitrogen wash-in/wash-out technique and release maneuver. However, Patroniti et al. 9 used the helium dilution method and found that EELV at zero end-expiratory pressure increased after application of high PEEP levels in mechanically ventilated ARDS patients. If passive spirometry is used for measurement, the recruitment volume would be underestimated if the FRC increases at higher PEEP levels.
The clinical and biological features were found to be different between ARDS from direct (pulmonary) and indirect (extra-pulmonary) causes.10,11 Gattinoni et al. 10 discovered a significantly higher recruitability induced by PEEP in extra-pulmonary ARDS patients compared with those with pulmonary causes of ARDS. Theoretically, augmentation in FRC might contribute to the increase in recruitment volume. 7 Therefore, we speculated that the influence of PEEP on FRC might be different in pulmonary and extra-pulmonary causes of ARDS.
In the present study, we primarily aimed to investigate whether there was a difference in FRC between low and high PEEP in different types of lung injuries.
Materials and methods
The study was approved by the Ethics Committee for Experimental Studies (No. 201803001) at Beijing Neurosurgical Institute, Beijing, China.
Animal preparation
Twelve healthy Bama pigs with a median (25th to 75th percentile) weight of 42 (40, 44) kg and aged 12 (11, 14) months were sedated with an intramuscular injection of ketamine hydrochloride (0.3 mL/kg) and xylazine hydrochloride (0.3 mL/kg). The animal was intubated and mechanically ventilated using an Engström Carestation ventilator (GE Healthcare, Madison, WI, USA). Propofol (1 to 5 mg/kg/hour) and fentanyl (0.4 μg/kg/hour) were continuously infused to provide sedation and analgesia. Vecuronium (0.3 mg/kg/hour) was used to eliminate respiratory efforts as needed.
The preparation included femoral arterial catheterization, a Swan-Ganz catheterization, and epicystostomy. A 7.0 Fr flow-directed thermodilution fiberoptic pulmonary artery catheter (Edwards Lifesciences, Irvine, CA, USA) was inserted for pulmonary arterial pressure, pulmonary arterial wedge pressure, central venous pressure, and cardiac output measurements as well as mixed venous blood sampling. Cardiac output was measured in triplicate using the pulmonary artery catheter. Arterial and mixed venous blood gases were analyzed. The femoral artery was cannulated with a 7.0 Fr pediatric jugular catheter (ES-04150, Arrow International Inc., Shanghai, China) for arterial blood sampling and arterial pressure monitoring. Continuous electrocardiogram (ECG) monitoring was performed. Additionally, a hemodynamic monitor (BeneView T5, Mindray, Shenzhen, China) was used.
During the experiment, the animal was placed in the supine position on a thermo-controlled operation table to maintain the rectal temperature of approximately 36 to 38°C. Normal saline was intravenously infused at a rate of 100 mL/hour. A fluid bolus was administered when the heart rate exceeded 120 beats/minute. Hypotension that persisted despite fluid replacement was treated with intravenous norepinephrine (10 μg bolus or continuous infusion at 0.05 to 0.5 μg/kg/minute). The mean arterial pressure was maintained above 65 mmHg.
The airway pressure was measured using a pressure transducer (KT 100D-2, Kleis TEK di CosimoMicelli, Monopoli, Italy, range: ±100 cmH2O). The flow was measured at the airway opening using a heated Fleisch pneumotachograph (Vitalograph Inc., Lenexa, KS, USA). Pressure and flow signals were displayed continuously and saved (ICU-Lab 2.5 Software Package, ICU Lab, Kleis TEK Engineering, Bari, Italy) on a laptop for further off-line analysis, at a sample rate of 200 Hz. 12
Lung injury models and experimental protocol
After collecting the baseline data, two lung injury models were induced. The experimental animals were randomly assigned to the pulmonary ARDS model or extra-pulmonary ARDS model, each with six pigs.
We used an instillation of hydrochloric acid (HCl, 0.1 N, 4 mL/kg) to induce pulmonary ARDS. 13 Mechanical ventilation was not discontinued during the HCl instillation. The HCl solution was instilled into the main trachea. The model was considered to be successfully established when the ratio of partial pressure of oxygen in the arterial blood to inspired oxygen fraction remained below 200 mmHg for at least 30 minutes. An additional 2 mL/kg of HCl solution was instilled into the trachea if the criterion was not met.
Oleic acid (0.1 mL/kg) in combination with 20 mL saline was injected into the right atrium via a Swan-Ganz catheter over 30 minutes to induce extra-pulmonary ARDS. 14 The criterion for model establishment was the same as that for the pulmonary ARDS model. An additional 0.05 mL/kg of oleic acid was injected if the criterion was not met.
During lung injury modeling, mechanical ventilation was set in the volume-controlled mode with constant flow, a tidal volume of 6 mL/kg, and a respiratory rate of 15 to 25 breaths/minute to maintain a partial pressure of carbon dioxide in the arterial blood value within the range of 35 to 45 mmHg, and an inspiratory/expiratory ratio of 1:2 with a 0.3-second inspiratory pause, PEEP of 5 cmH2O, and an inspired oxygen fraction of 0.4.
After establishing either the pulmonary or extra-pulmonary model, two PEEP levels (5 and 15 cmH2O) were applied in a random order. Throughout the study procedure, all the ventilator settings were left unchanged except for the PEEP levels.
Measurements
EELV was measured using the wash-in/wash-out method that was integrated into the ventilator, which used a continuous measurement of end-tidal carbon dioxide and oxygen concentrations to calculate the nitrogen concentration. The continuous measurement of end-tidal carbon dioxide and oxygen concentrations during a relatively small change in inspired oxygen fraction (10% to 20%) allowed for the calculation of the aerated lung volume during wash-in/wash-out maneuvers. The mean of the wash-in and wash-out data was calculated automatically if the difference between the two measurements was less than 20%.15,16
Before and after the establishment of the lung injury model and after at least 60 minutes at each PEEP level, measurements were conducted in the following order:
Gas exchange and hemodynamic parameters were measured and derived using standard formulas.
17
EELV at PEEP level of 5 or 15 cmH2O was measured using the wash-in/wash-out method, as described above. End-inspiratory and end-expiratory airway occlusion were performed, each for 5 seconds. Airway driving pressure and respiratory system compliance were calculated using standard formulas.
17
During end-expiratory occlusion, a release maneuver was performed by disconnecting the animal from the ventilator with the pneumotachograph remaining on the tracheostomy tube until the flow tracing reached zero, which indicated a completed expiration to the relaxed state of the respiratory system without a positive static elastic recoil pressure.9,18 To guarantee that the relaxed state of the respiratory system had been reached, the end of the endotracheal tube was manually occluded at the end of expiration, and the pressure tracing was observed. No increase in airway pressure after airway occlusion indicated that the relaxed state was reached without intrinsic PEEP. The volume that was passively exhaled during the release maneuver was integrated by flow tracing and defined as the lung volume change induced by PEEP. FRC was calculated as the difference between EELV and lung volume change induced by PEEP.
5
Then, the animal was reconnected to the ventilator. At this moment, mechanical ventilation was delivered at zero end-expiratory pressure, and EELV was immediately measured (EELV0). Finally, a low-flow inflation P–V curve (constant flow at 6 L/minute, inflation volume of 3,000 mL, and starting pressure at 0 cmH2O) was performed at zero end-expiratory pressure to exclude airway closure.
19
The recruitment volume between the high and low PEEP levels was measured using the wash-in/wash-out method, as previously reported. 5 Briefly, recruitment volume equals the change in EELV (which is equal to the difference between EELV at 15 and 5 cmH2O of PEEP) minus the minimal predicted increase in lung volume (which is equal to the product of the respiratory compliance at low PEEP and the change in PEEP).
Statistical analysis
Continuous data are presented as the mean ± standard deviation (SD). The comparisons of parameters before and after lung injury modeling, as well as between high and low PEEP levels, were performed using paired t-tests. Recruitment volume from low to high PEEP in different ARDS models were compared using t-tests. The correlation between FRC and EELV0 was tested using a linear regression analysis. Additionally, p < 0.05 (two-tailed) was considered to be statistically significant. Statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA).
Results
Lung injury modeling
ARDS was successfully induced in all experimental animals. The data collected before and after lung injury modeling are shown in Table 1. The ratio of partial pressure of oxygen in the arterial blood to inspired oxygen fraction was 155 ± 13 and 155 ± 20 after the establishing the pulmonary and extra-pulmonary ARDS models, respectively. Respiratory compliance and EELV at 5 cmH2O PEEP decreased significantly after modeling. There was no airway closure in any of the animals based on the P–V curve at zero end-expiratory pressure.
Data collected before and after lung injury modeling*.

Data are shown as the mean ± standard deviation. * Parameters were determined at 5 cmH2O of positive end-expiratory pressure.
Abbreviation: ARDS, acute respiratory distress syndrome; PaO2/FiO2, the ratio of arterial partial pressure of oxygen to fraction of inspiration oxygen; MAP, the mean arterial pressure; HR, heart rate; VD/VT, dead space ratio; MPAP, mean pulmonary arterial pressure; PAWP, pulmonary arterial wedge pressure; CVP, central venous pressure; CO, cardiac output; Pplat, plateau airway pressure; EELV, end-expiratory lung volume; CRS, compliance of respiratory system.
Lung volume measurements
No significant differences were found in FRC or EELV0 between 5 and 15 cmH2O of PEEP in either pulmonary or extra-pulmonary ARDS (Figure 1).

Comparison of functional residual capacity (FRC) and end-expiratory lung volume at zero end expiratory pressure (EELV0) at 5 and 15 cmH2O of positive end-expiratory pressure (PEEP).
EELV0 correlated linearly with FRC in both the pulmonary (R2 = 0.967, p < 0.001) and extra-pulmonary ARDS (R2 = 0.595, p = 0.003, Figure 2). EELV0 (267 ± 112 mL) measured at zero end-expiratory pressure was significantly lower compared with FRC (311 ± 136 mL) measured by the release maneuver (p = 0.001).
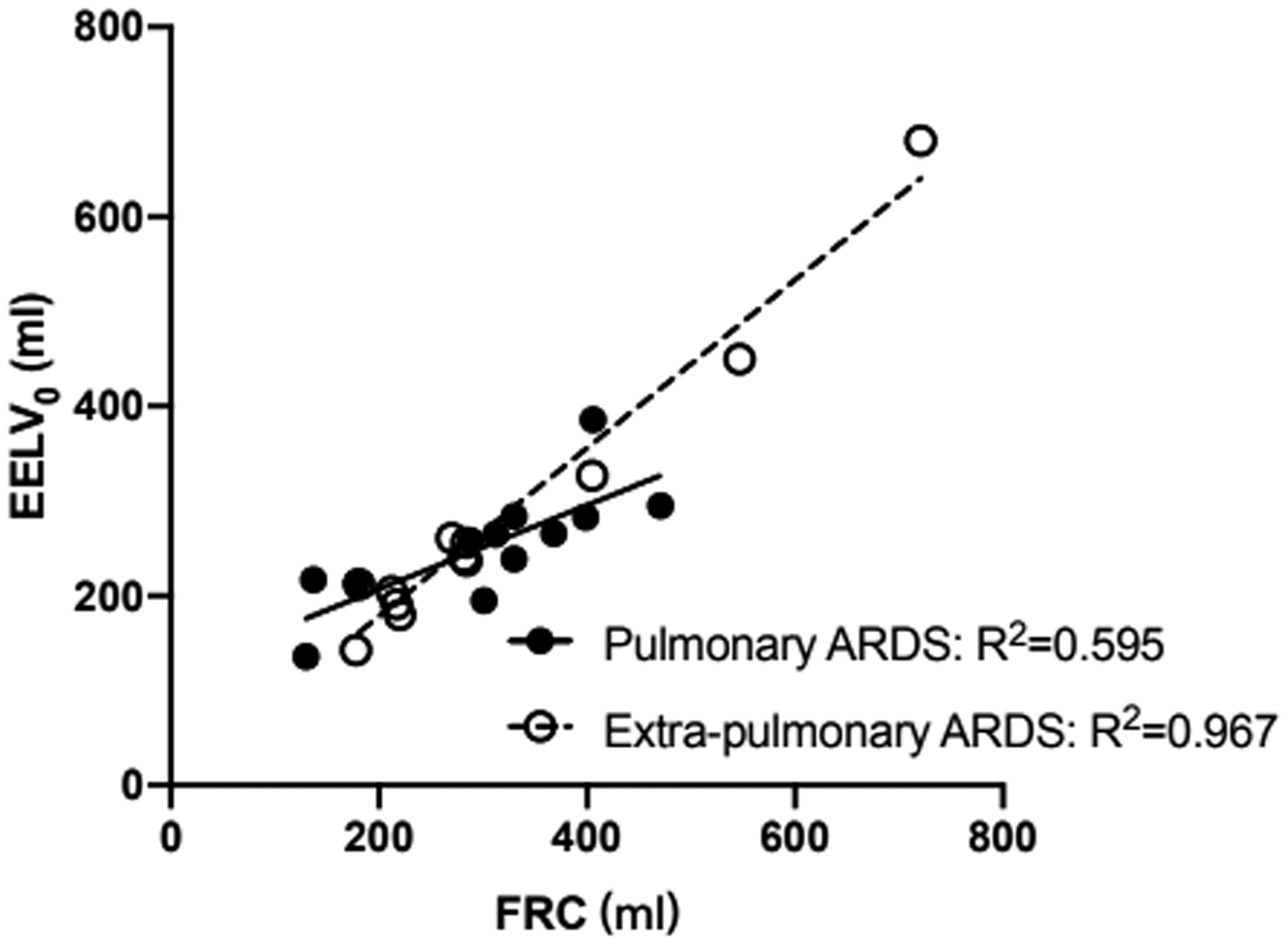
End-expiratory lung volume at zero end expiratory pressure (EELV0) correlated linearly with functional residual capacity (FRC) in either pulmonary or extra-pulmonary ARDS.
There was no significant difference in recruitment volume between pulmonary (341 ± 100 mL) and extra-pulmonary (351 ± 170 mL) ARDS.
Respiratory mechanics, gas exchange, and hemodynamic parameters
The respiratory mechanics, gas exchange, and hemodynamic parameters at low and high PEEP levels are shown in Table 2. The ratio of the partial pressure of oxygen in the arterial blood to the inspired oxygen fraction, respiratory system compliance, pulmonary arterial wedge pressure, and central venous pressure were significantly higher, while the dead space was significantly lower at high PEEP compared with low PEEP in both the pulmonary and extra-pulmonary ARDS models.
Respiratory mechanics, gas exchange, and hemodynamic parameters at low and high positive end-expiratory pressure (PEEP).

Data are shown as the mean ± standard deviation.
Abbreviation: ARDS, acute respiratory distress syndrome; PaO2/FiO2, the ratio of arterial partial pressure of oxygen to fraction of inspiration oxygen; MAP, the mean arterial pressure; HR, heart rate; VD/VT, dead space ratio; MPAP, mean pulmonary arterial pressure; PAWP, pulmonary arterial wedge pressure; CVP, central venous pressure; CO, cardiac output; CRS, compliance of respiratory system.
Discussion
In the present study, we used the nitrogen wash-in/wash-out technique and release maneuver to determine FRC at low and high PEEP in pulmonary and extra-pulmonary ARDS pig models. There was no significant difference in FRC at different PEEP levels, which suggested that FRC was not affected by PEEP. Our result was in agreement with the common assumption for recruitment volume measurement using passive spirometry. This assumption was derived from previous studies in ARDS patients, which showed that the same FRC was verified at different PEEP levels using respiratory inductive plethysmography, 8 standardized multiple P–V curves, 6 and the nitrogen wash-in/wash-out technique. 5 However, using the helium dilution method, Patroniti et al. 9 found that EELV after removal of PEEP, which is physiologically similar to FRC, increased at high PEEP levels. If FRC was modified by PEEP, recruitment volume would be underestimated using the commonly employed bedside methods, such as multiple P–V curves 20 and release maneuvers.5,18
During positive-pressure ventilation with PEEP, EELV contains an increase in lung volume that was induced by PEEP and FRC.7,21 The definition of FRC is the lung volume without a positive static elastic recoil pressure.7,21 There are several methodological differences between Patroniti’s study 9 and our study. Patroniti et al. 9 used the helium dilution method to measure EELV after removal of PEEP. In the present study, we measured FRC using the release maneuver that was introduced by Ranieri et al.,8,22 Dellamonica et al., 5 and Chiumello et al. 18 Our experimental protocol is consistent with the standard method for recruitment volume measurement using passive spirometry at the bedside. Additionally, we used several procedures to guarantee the accuracy of the FRC measurement. First, flow tracing was carefully inspected during passive exhalation after the release maneuver. Second, we performed airway occlusion at the end of expiration to the atmosphere to exclude intrinsic PEEP, which might result in an overestimation of the FRC measurement. 6 Third, we also recorded a low-flow inflation P–V curve at zero end-expiratory pressure to exclude airway closure, which was reported to be highly prevalent in ARDS patients 19 and might also result in an overestimation of the FRC measurement. These procedures supported the accuracy of the FRC measurement. Finally, consistent with most recruitment studies,4,5,9 we maintained each of the two PEEP levels for at least 60 minutes to stabilize the PEEP effect.
We also identified PEEP-induced recruitment in our ARDS models. However, a similar FRC at low and high PEEP indicated that lung volume returned to the previous level after removal of PEEP. Our results suggested that the recruitment might represent the short-term effect of PEEP on the respiratory mechanics. This was in accordance with the results reported by Pelosi et al. 23 in an animal study with oleic acid and by Crotti et al. 24 in ARDS patients. During positive pressure ventilation with PEEP, alveolar collapse increased significantly when superimposed pressure was elevated over PEEP.
In contrast to our speculation, differences in FRC and recruitment volume were not found between the pulmonary and extra-pulmonary ARDS models. Although studies have shown that the effect of PEEP on alveolar recruitment was smaller in patients with pulmonary ARDS compared with those with extra-pulmonary ARDS,10,25 the results were not consistent. Thille et al. 26 reported similar alveolar recruitment in pulmonary and extra-pulmonary ARDS in a large sample of patients. Recently, Coppola et al. 11 demonstrated that pulmonary ARDS presented as a higher lung recruitability in the early stage compared with extra-pulmonary ARDS. The identification of clinical phenotypes represents personalized medicine for ARDS patients in the future. 27
There are some limitations to our study. First, CT is the gold standard for measuring the lung volume. We did not acquire CT scans. However, we used a modified nitrogen wash-in/wash-out technique, which correlates well with CT scans and can be easily used in clinical practice. 28 Second, we did not perform pathological examination to verify pulmonary and extra-pulmonary ARDS. However, an instillation of hydrochloric acid and infusion of oleic acid are the standard methods for inducing pulmonary and extra-pulmonary ARDS. 29 Oleic acid is directly toxic to endothelial cells, causing some areas to show interstitial edema, which is the main pathologic mechanism in extra-pulmonary ARDS. Instead, consolidation and alveolar edema are expected in pulmonary ARDS. Hydrochloric acid aspiration is a lung injury that is characterized by airway and alveolar epithelium injury, which causes impairment in the alveolar epithelial fluid transport function. Third, the study was conducted in animals. Further studies are needed in the clinical setting.
In conclusion, modification of PEEP on FRC was not found in either pulmonary or extra-pulmonary ARDS pig models, which supports the use of passive spirometry for recruitment measurement at the bedside.
Footnotes
Declaration of conflicting interest
Jian-Xin Zhou received an Engström Carestation ventilator from GE Healthcare, Madison, WI, USA for the present experimental use. Other authors declare that there is no conflict of interest.
Funding
The study was supported by a grant from the National Natural Science Foundation of China (No: 81871582). The sponsor had no role in the study design, data collection, data analysis, data interpretation, or writing of the report.