
Abstract
Objectives
To investigate the ability of matrix metalloproteinase (MMP)-2 and CD44 variant 6 (CD44v6) protein levels to diagnose papillary thyroid cancer (PTC), compared with routine diagnostic methods using tissue sections; to explore the relationship between MMP-2 and CD44v6 protein levels and lymph node metastases (LNM) in PTC.
Methods
Archival PTC specimens from patients with PTC, with or without lateral cervical LNM, were included in this retrospective immunohistochemical study. MMP-2 and CD44v6 protein levels were analysed immunohistochemically using routinely prepared tissue sections.
Results
Specimens from 66 patients with PTC were reviewed retrospectively (35 patients with lateral cervical LNM; 31 patients without LNM). The percentages of samples with cells that demonstrated positive protein staining differed significantly between PTC specimens, benign thyroid nodules and adjacent normal follicular epithelium (MMP-2: 86.4%, 60.0%, and 25.7%, respectively; CD44v6: 80.3%, 37.1% and 22.9%, respectively). The level of CD44v6 protein staining was found to be significantly and positively correlated with the level of MMP-2 protein staining in PTC specimens.
Conclusions
Both MMP-2 and CD44v6 might be useful tumour markers for predicting risk of lateral cervical LNM in patients with PTC.
Keywords
Introduction
Papillary thyroid carcinoma (PTC) is the most common type of differentiated thyroid carcinoma.1,2 The incidence of thyroid cancer has increased dramatically in the USA, with a 240% rise observed between 1972 and 2002. 1 Between 1996 and 2008, an increasing incidence of PTC was reported in Denmark, with age-standardized incidence rates increasing from 1.43 per 100 000 per year in 1996 to 2.16 per 100 000 per year in 2008. 3 Compared with other malignancies, PTC has excellent 5- and 10-year survival rates (93–96% and 86–90%, respectively).4,5 Regional lymph node metastases (LNM) are present at the time of primary diagnosis in 20–60% of patients with PTC.6,7 A comprehensive review of the literature suggests that the presence of macroscopic metastases of PTC in cervical lymph nodes results in a higher recurrence rate and increased death rate. 8 The combination of surgery, radioactive iodine treatment and thyroid hormone suppression is the mainstay of treatment for PTC.4,6 The optimal combined treatment for PTC with LNM requires a better understanding of the underlying molecular mechanisms involved, but it is still not possible to predict cervical LNM in patients with PTC.
Observations from other nonthyroid experimental models and clinical studies have illustrated the critical role of matrix metalloproteinase (MMP)-2 in tumour progression, angiogenesis, metastasis and recurrence.9,10 Several studies have reported the upregulation of MMP-2 in PTC and have suggested an important role for this enzyme in the progression of PTC.11,12 CD44 variant 6 (CD44v6) is expressed only in proliferating thyroid cells and is upregulated in carcinomas; in addition, its upregulation is related to more aggressive behaviour in carcinomas, and to the occurrence of metastasis.13–19
This current retrospective study used immunohistochemical analysis to compare protein levels of MMP-2 and CD44v6 in PTC tumour specimens from patients with PTC with lateral cervical LNM, and from patients with PTC without LNM in order to: (i) determine the significance of MMP-2 and CD44v6 protein levels in the differential diagnosis of PTC; (ii) analyse the relationship between MMP-2 and CD44v6 protein levels and lateral cervical LNM in patients with PTC; (iii) explore the potential role of MMP-2 and CD44v6 protein levels in predicting patients with PTC who are at heightened risk of lateral cervical LNM.
Patients and methods
Patient population
This retrospective study analysed surgical specimens excised from consecutive patients with surgically and histologically confirmed PTC between April 2010 and October 2011, in the Department of General Surgery, Huashan Hospital, Fudan University, Shanghai, China. All patients with PTC who received PTC radical surgery and central and/or lateral cervical lymph node clearance were enrolled in the study. Surgical specimens were retrieved from the archive of the Department of Pathology, Huashan Hospital. Surgical modalities used to treat the patients were also retrieved from the patients’ medical records. Benign thyroid nodules from other patients, which were stored in the archive of the Department of Pathology for use in research, and adjacent normal follicular epithelium specimens collected from the same patients during surgery, were analysed for comparison.
The study complied with the Declaration of Helsinki and was approved by the Science and Technology Committee and the Ethics Committee of Baoshan District, Shanghai, China (no. 11-E-13). As only routine procedures were used on archived surgical specimens and no treatment interventions were investigated, patients who provided samples for the study were not required to provide written or verbal informed consent.
Immunohistochemical analysis
All surgical specimens were subjected to routine pathological examination and immunohistochemical staining for MMP-2 and CD44v6 proteins. Tissue samples were fixed in 30% formalin, dehydrated in ethanol and embedded in paraffin wax. For routine pathological examination, all specimens were sliced continuously into 4-µm-thick sections, stained with haematoxylin and eosin and examined by two independent pathologists (Z. Z. and Feng Tang, Department of Pathology, Huashan Hospital), both of whom were experienced in evaluating thyroid pathology. These examinations were conducted blindly and independently, and the pathologists did not know each patient’s original histological diagnosis. All specimens were classified according to the published diagnostic criteria for thyroid tumours. 20
Immunohistochemical staining was performed using the streptavidin-peroxidase method as described previously and 4-µm sections prepared as described above.12,21 After the sections had been deparaffinized and rehydrated in a descending series of alcohol dilutions, they were heated in an 800 -W microwave oven at maximum power for 5 min in 0.01 mol/l citrate buffer (pH 6.0) for antigen retrieval, then cooled to room temperature. After blocking with goat serum (Invitrogen, Carlsbad, CA, USA), the sections were incubated with primary mouse antihuman antibodies to MMP-2 (1: 1000 dilution; Santa Cruz Biotechnology, Santa Cruz, CA, USA) or CD44v6 (1: 1000 dilution; Santa Cruz Biotechnology) for 20 min at room temperature. Then, the slides were washed three times using 0.1 M phosphate-buffered saline (PBS; pH 7.4) and incubated with a biotinylated horseradish peroxidase goat antimouse secondary antibody (1: 500 dilution; Invitrogen) for 20 min at 37℃. Slides were washed three times after incubation with the secondary antibody using 0.1 M PBS (pH 7.4). Immunolabelling was visualized with 0.05% diaminobenzidine (Invitrogen) in 0.01 M PBS (pH 7.4) for 5 min at room temperature and the slides were then rinsed for 2 min under running tap water. The immunohistochemical staining was examined and photographed (at × 100 and × 400 magnification) using an Olympus BX51 light microscope (Olympus Optical, Tokyo, Japan). The percentage of positive cells was evaluated semiquantitatively by counting the number of labelled cells in 10 randomly selected high-power fields for each specimen, at × 400 magnification. MMP-2 immunostaining was located in the cytoplasm; CD44v6 immunostaining was located in the cytoplasm and cell membranes. Breast-cancer specimens were provided by the Department of Pathology, Huashan Hospital to act as positive control samples for CD44v6 and MMP-2 immunostaining. For negative control slides, the primary antibody was replaced with 0.1 M PBS (pH 7.4).
An ‘immunohistochemical score’ (IHS) was calculated for MMP-2 and CD44v6 for each specimen. This score took into account the percentage of cells (0–100%) as well as the staining intensity category (− to +++). The scoring system used for both MMP-2 and CD44v6 proteins was similar to previously published methods.22–24 The extent of positively stained cells was estimated and classified on a five-point scale as follows: grade 0, < 10%; grade 1, ≥ 10% and ≤ 25%; grade 2, > 25% and ≤ 50%; grade 3, > 50% and ≤ 75%; grade 4, > 75%. The intensity of the positive staining was categorized into three groups: weak (1); moderate (2); strong (3). A final IHS score was obtained by multiplying the score for the extent and the score for intensity as follows: 0, negative (−); 1–4, weakly positive (+); 5–8, moderately positive (++); 9–12, strongly positive (+++).
Statistical analyses
All statistical analyses were performed using the SPSS® statistical software package, version 11.5 (SPSS Inc., Chicago, IL, USA) for Windows®. Two-tailed two-independent samples test or χ2-test were used to determine the difference between groups. Pearson’s contingency coefficient (C) was used to test for any associations between the levels of MMP-2 and CD44v6 proteins. A P-value of < 0.05 was considered statistically significant for all tests.
Results
Surgical resection specimens from patients with PTC were retrieved from the archive of the Department of Pathology, Huashan Hospital. Surgical modalities that were used to treat the patients were as follows: PTC radical surgery + central lymph node clearance (level VI) (n = 55 with LNM; n = 28 without LNM; PTC radical surgery + lateral cervical lymph node clearance (levels II–VI) (n = 35 with LNM; n = 3 without LNM). Immunohistochemical staining for MMP-2 and CD44v6 proteins was undertaken on 35 patients with PTC with lateral cervical LNM and 31 patients with PTC without cervical LNM. Therefore, these 66 patients were included in the present analysis. A total of 35 benign thyroid nodules and 35 adjacent normal follicular epithelium specimens were collected, for comparison. The 66 patients with PTC (19 males and 47 females) had a mean age of 43.6 years (range 26–73 years). The 35 patients with PTC with lateral cervical LNM (14 males and 21 females) had a mean age of 42.8 years (range 26–61 years) and the 31 patients with PTC without cervical LNM (5 males and 26 females) had a mean age of 44.5 years (range 26–73 years). The 35 patients with benign thyroid nodules (9 males and 26 females) had a mean age of 41.7 years (range 21–69 years).
Immunohistochemical scores for matrix metalloproteinase (MMP)-2 protein staining in surgical specimens of thyroid cancer tissue, taken from patients with papillary thyroid carcinoma (PTC) with or without lymph node metastases (LNM) (n = 66) compared with benign nodules and normal tissue specimens.

Data presented as n specimens with the following immunohistochemical scores: − negative; + weakly positive; ++ moderately positive; +++ strongly positive.
PTC tissue versus benign nodules, Z = −4.762; two-tailed two-independent samples test.
PTC tissue versus normal tissue, Z = −6.306; two-tailed two-independent samples test.
LNM positive versus LNM negative, Z = −4.051; two-tailed two-independent samples test.
LNM negative versus benign nodules, Z = −2.634; two-tailed two-independent samples test.
Immunohistochemical scores for CD44 variant 6 (CD44v6) protein staining in surgical specimens of thyroid cancer tissue, taken from patients with papillary thyroid carcinoma (PTC) with or without lymph node metastases (LNM) (n = 66) compared with benign nodules and normal tissue.
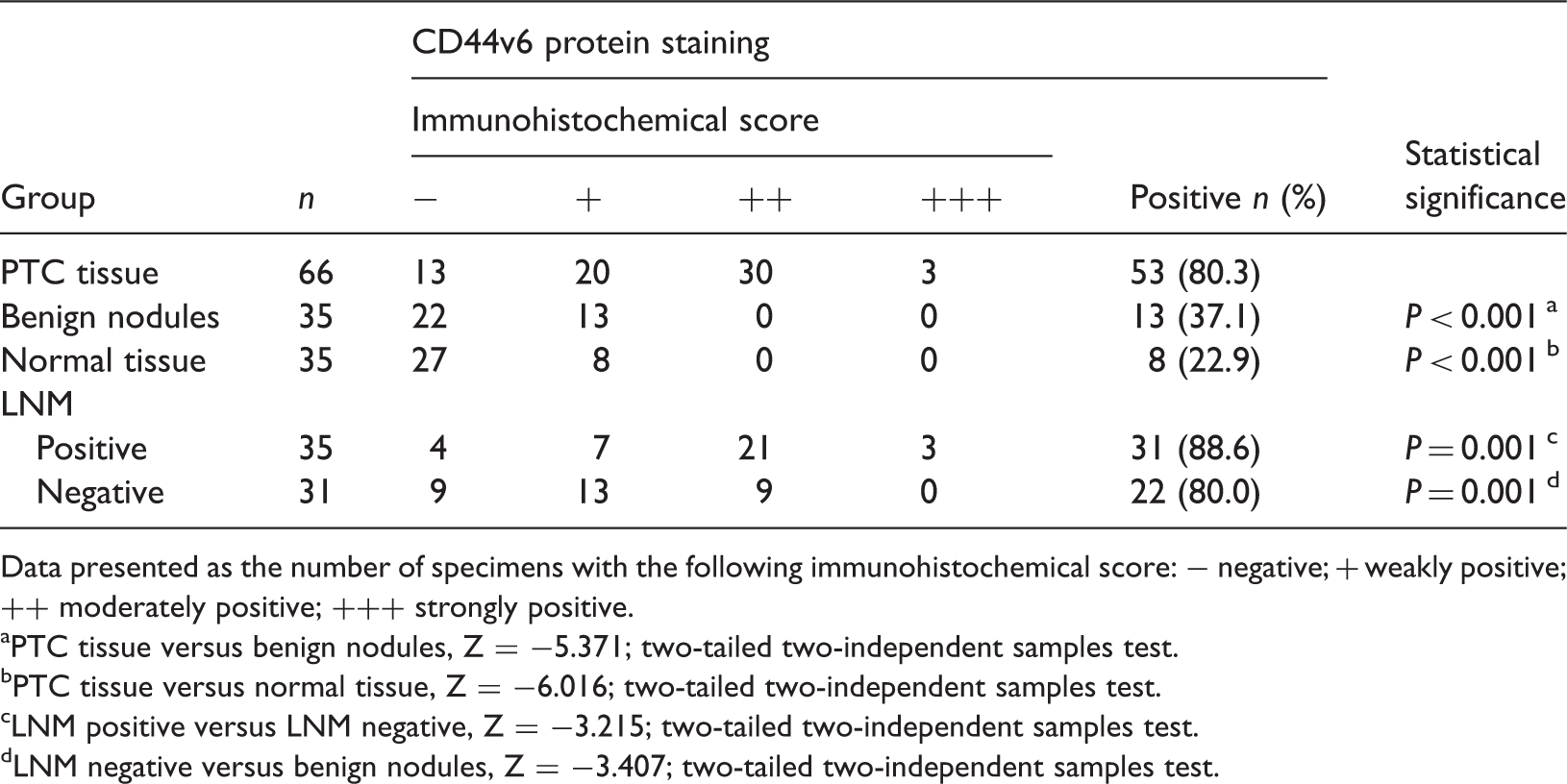
Data presented as the number of specimens with the following immunohistochemical score: − negative; + weakly positive; ++ moderately positive; +++ strongly positive.
PTC tissue versus benign nodules, Z = −5.371; two-tailed two-independent samples test.
PTC tissue versus normal tissue, Z = −6.016; two-tailed two-independent samples test.
LNM positive versus LNM negative, Z = −3.215; two-tailed two-independent samples test.
LNM negative versus benign nodules, Z = −3.407; two-tailed two-independent samples test.
Pearson’s contingency coefficient analysis of the association between the level of immunohistochemical staining of matrix metalloproteinase (MMP)-2 and CD44 variant 6 (CD44v6) proteins in surgical specimens of thyroid cancer tissue, taken from patients with papillary thyroid carcinoma (n = 66).
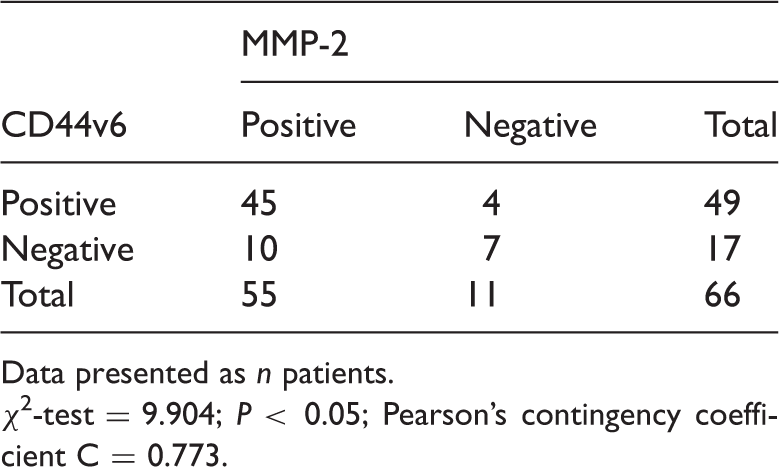
Data presented as n patients.
χ2-test = 9.904; P < 0.05; Pearson’s contingency coefficient C = 0.773.
Discussion
The incidence of malignant tumour of the thyroid (MTT) has increased significantly and it has now become the most common malignant tumour of the neck.1,25,26 PTC is the most frequently observed MTT, accounting for approximately 94.8% of all MTT cases. 27 A comprehensive review of the literature suggests that, compared with their absence, the presence of macroscopic metastases of PTC in cervical lymph nodes results in a higher recurrence rate and increased death rate. 8 Regional LNM are present at the time of primary diagnosis in 20–60% of patients with PTC.6,7 Therefore, it is important to find biological factors that affect the development of LNM and the survival of patients with PTC. Currently, there is a lack of markers that can predict which patients have a higher risk of lateral cervical LNM, or distinguish between patients with a low or high risk of a poor outcome. 8
Matrix metalloproteinases are zinc-dependent endopeptidases involved in degradation of the extracellular matrix that play an important role in tumour progression, by providing a permissive microenvironment for tumour invasion and metastasis. 9 MMPs are categorized as collagenases (MMP-1, -8, and -13), gelatinases (MMP-2 and -9), stromelysins (MMP-3, -10, and -11), membrane-type MMPs (MMP-14 to MMP-17, -24, and -25), or matrilysins (MMP-7 and -26), according to their substrate specificities. 28 Observations from other nonthyroid experimental models and clinical studies have illustrated the critical role of MMP-2 in tumour progression, angiogenesis, metastasis, recurrence and immune surveillance.9,10,12 As a result of such activities, upregulated levels of MMP-2 protein in cancer are predictive of a poor prognosis. 10
Studies have reported that PTC specimens have upregulated levels MMP-2 protein, and suggest an important role for this enzyme in the progression of PTC.11,12 In this current study, there was a significant difference in the immunohistochemical score for MMP-2 protein staining, not only among PTC specimens, benign thyroid nodules and normal thyroid tissue, but also between PTC specimens from patients who developed lateral cervical LNM and those who did not develop LNM. The results of this current study showed that the increased level of MMP-2 immunohistochemical staining in PTC specimens was related to the frequency of lateral cervical LNM. These current results were in accordance with previous studies that reported that levels of MMP-2 protein were associated with LNM in thyroid cancer.11,12
The cell surface receptor for hyaluronic acid, CD44, exists as a standard isoform (CD44s) and as multiple variant isoforms generated by the alternative splicing of up to 10 variant exons (v1–v10). 18 Among them, CD44v6 is expressed only in proliferating thyroid cells and is upregulated in carcinomas; its expression is related to more aggressive behaviour of carcinomas and metastasis.13–19 Many studies have sought to clarify the role of CD44v6 in human neoplasms including pancreatic cancer, gastric cancer, transitional cell carcinoma of the bladder and oesophageal carcinoma.16,18,19,29 The CD44v6 level is closely related to the grade, stage, infiltration, invasion and metastasis of cancer, and it may play a vital role in predicting the prognosis and therapeutic effect of anticancer agents.16,30,31
This current study showed that the percentages of samples with cells that demonstrated positive CD44v6 protein staining in PTC specimens, benign thyroid nodules and normal thyroid tissues were 80.3%, 37.1%, and 22.9%, respectively. The immunohistochemical score for CD44v6 protein staining was significantly higher in PTC specimens than in benign thyroid nodules and adjacent normal thyroid tissue. None of the benign thyroid nodules or normal thyroid tissue samples had cells that demonstrated moderate (++) to strong (+++) CD44v6 staining. There were significant differences in the immunohistochemical scores for CD44v6 protein staining, especially for the percentage of samples with cells that demonstrated moderate (++) to strong (+++) CD44v6 staining, between PTC specimens from patients who developed lateral cervical LNM and those who did not develop LNM. Zhang et al. 32 observed the regulatory action of the polo-like kinase 1 (PLK1) gene in the invasion of anaplastic thyroid carcinoma cells and suggested that CD44v6, MMP-2 and MMP-9 were likely to be involved in the regulation of cell invasion induced by PLK1.
In conclusion, protein levels of MMP-2 and CD44v6, as measured by immunohistochemical staining of tissue specimens in this current study, may play important roles in the progression of PTC and the development of LNM. The detection of high levels of MMP-2 and CD44v6 protein in PTC specimens may aid in the prediction of disease progression in patients with early stage PTC. MMP-2 and CD44v6 levels have the potential to be used as predictive markers for patients with PTC who are at heightened risk of LNM, so that individualized treatment can be initiated as early as possible in the disease course. This study was a retrospective study with a small sample size, so these data will need to be confirmed in larger, prospective, multicentre studies in future.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.