
Abstract
Objective
To investigate the independent risk factors and potential predictors of bladder cancer-related ischemic stroke (BCRIS).
Methods
This was a multi-center retrospective study including patients with active bladder cancer and acute ischemic stroke without traditional stroke risk factors (BCRIS group), and sex- and age-matched patients with active bladder cancer alone (control group). Data were collected between January 2006 and December 2018. Uni- and multivariate analyses were performed to identify independent risk factors for BCRIS. The predictive performance of these risk factors was assessed using receiver operating characteristic (ROC) curves.
Results
Records were retrospectively reviewed from 60 BCRIS patients and 120 bladder cancer controls. Univariate analysis revealed that serum D-dimer and carcinoembryonic antigen (CEA) levels and the platelet and neutrophil counts were significantly higher in BCRIS patients compared with controls. Multivariate analysis identified the three above-mentioned variables as independent risk factors for BCRIS. The product of all three factors gave the largest area under the ROC curve.
Conclusions
Elevated serum D-dimer and CEA levels and increased platelet count were independent risk factors for BCRIS, and the cut-off value based on the product of the three independent risk factors (≥2,640,745.29) could serve as a potential predictor of BCRIS.
Keywords
Introduction
Patients with active cancer have a higher risk of stroke, and much attention has recently been paid to cancer-related ischemic stroke (CRIS) because of the complex conditions and poor prognosis.1–3 Previous studies have shown that CRIS has various clinical features, such as multiple lesions in the brain, elevated serum D-dimer and fibrinogen levels, elevated C-reactive protein, and anti-neoplastic treatments.3–6 Therefore, identifying patients with bladder cancer who are at risk of developing ischemic stroke is a clinical challenge. We speculated that finding a method to predict CRIS in cancer patients will help clinicians develop effective strategies for CRIS prevention and treatment that will hopefully decrease the incidence and mortality rates.
Our previous studies showed that the occurrence of CRIS was related to independent risk factors that were derived from serum, and the independent risk factors for CRIS are heterogeneous because they have different pathological types.7–9 It was suggested that the characteristics of specific pathological types of CRIS risk factors may identify CRIS and may even predict its occurrence. Bladder cancer is the tenth most frequent cancer worldwide and the most common urinary tract malignancy. 10 Recently, it was found that compared with the general population, the incidence of ischemic stroke in patients with active bladder cancer was 1.9 times higher, 11 indicating that bladder cancer may be an etiology of ischemic stroke, which is called bladder cancer-related ischemic stroke (BCRIS). As tumor treatment improves and life expectancy becomes longer, the number of patients with BCRIS will increase. However, the independent risk factors of BCRIS and when BCRIS will develop in patients with bladder cancer remain unknown. In the present study, we investigated the independent risk factors for BCRIS and potential predictors that were derived from the independent risk factors for BCRIS to predict the occurrence and development of BCRIS in bladder cancer patients.
Patients and methods
This protocol was approved by the Medical Ethics Committee of the First Affiliated Hospital of Guangxi Medical University and it was conducted in accordance with the Declaration of Helsinki and current ethical guidelines. Other hospitals also agreed with the decision. Informed consent was obtained from all participants and/or their legal guardians.
Patient selection
All participants with a histopathological diagnosis of bladder cancer were eligible for the study. The BCRIS group comprised active bladder cancer and acute ischemic stroke patients who did not have traditional stroke risk factors and who were treated between January 2006 and December 2018 at six hospitals in Guangxi. Traditional stroke risk factors were defined as follows: (1) hypertension (systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg or taking antihypertensive medications); (2) diabetes (fasting blood glucose level ≥7.0 mmol/L or on antidiabetic treatment); (3) hyperlipidemia (serum total cholesterol >5.72 mmol/L or triglycerides >1.70 mmol/L or high-density lipoprotein <0.91 mmol/L or low-density lipoprotein >3.64 mmol/L, or taking lipid-lowering medications); and (4) smoking and alcohol consumption, coronary artery disease, and atrial fibrillation (history of disease, or assessed by cardiologist based on electrocardiogram and transthoracic echocardiography results at admission). We searched the medical records of Guangxi hospitals where we had collaborations, and we found 23 BCRIS patients at the First Affiliated Hospital of Guangxi Medical University (January 2006–December 2018); six at the Second Affiliated Hospital (May 2016–July 2018); 24 at the Guangxi Cancer Hospital (January 2006–December 2018); two at the Guangxi Medical University Ninth Affiliated Hospital (July 2014–July 2018); three at the Fusui County People’s Hospital (December 2014–July 2018); and two at the Wuming Hospital of Guangxi Medical University (June 2015–September 2018). Age- and sex-matched control patients had active bladder cancer but no ischemic stroke and were admitted to the same hospitals within the same period. Additionally, the BCRIS group of patients displayed various signs and symptoms of neurological deficits, and diffusion-weighted imaging (DWI) examination confirmed the presence of acute ischemic stroke. Only patients with contraindications for DWI underwent cranial non-enhanced computed tomography (CT). We excluded patients without acute ischemic stroke, with traditional stroke risk factors, who had other concomitant cancers and metastatic brain tumors, hematological cancer, cerebral hemorrhage, and incomplete medical records (Figure 1).

The patient database included 7739 bladder cancer patients. Based on the inclusion criteria, 60 patients with bladder cancer-related ischemic stroke (BCRIS) and 120 patients with bladder cancer alone (control) were included.
Definitions
Active bladder cancer was defined as bladder cancer that was newly diagnosed, treated within 6 months before the onset of ischemic stroke, or confirmed to be recurrent or metastatic. 12 Acute ischemic stroke was diagnosed based on the American Heart Association criteria. 13 Because it is difficult to identify BCRIS in clinical practice, BCRIS in the present study was defined as patients with acute ischemic stroke and active bladder cancer without traditional stroke risk factors, based on the definition of cancer-related stroke.14–16 The etiological classification of “ischemic” is an undetermined etiology, according to the Trial of ORG 10172 in Acute Stroke Treatment TOAST criteria. 17 The severity of neurological deficits was evaluated using the National Institutes of Health Stroke Scale (NIHSS), and the prognosis was evaluated using the modified Rankin scale (mRS) at 30 days after ischemic stroke. A score of 0 to 2 on mRS indicates a good prognosis; 3 to 5 indicates a poor prognosis; and 6 indicates death.
Data collection
A retrospective review of bladder cancer patients with ischemic stroke was used to identify clinical and laboratory results. Clinical data were obtained for age, sex, traditional stroke risk factors, histological types of bladder cancer, metastasis, therapeutic methods, lesion patterns in ischemic stroke, the severity of neurological deficits, time interval assessed from diagnosis of bladder cancer until ischemic stroke, and results of auxiliary examinations such as cranial non-contrast CT, CT angiography, magnetic resonance imaging (MRI), DWI, electrocardiogram, echocardiography, and transcranial Doppler ultrasound. Laboratory data, including routine complete blood count tests, blood biochemistry, prothrombin time (PT), fibrinogen, as well as serum levels of D-dimer, carcinoembryonic antigen (CEA), and cancer antigens-125, -153, and -199, were collected within 24 hours after stroke occurrence.
Statistics
Statistical analyses were performed using SPSS version 20.0 (IBM, Armonk, NY, USA). Categorical variables are presented as n (%), and continuous variables are presented as the mean ± standard deviation (SD). Inter-group differences were assessed for significance using independent-sample t-tests or the Mann–Whitney U-test for continuous data, or using the chi-squared and Fisher’s exact tests for categorical data. Uni- and multivariate binary logistic regression was used to identify clinical variables that differed significantly between BCRIS patients and cancer controls to identify independent BCRIS risk factors. The area under the receiver operating characteristic (ROC) curve (AUC) was used for each factor alone and to calculate the product of the independent risk factors as a new variable. The optimal cut-off value was determined by the Youden index. MedCalc (version 10.4.8®, Frank Schoonjans; Bvba, Ostend, Belgium; https://www.medcalc.org) was used to compare the AUC of each independent risk factor and their product. The variable with the largest AUC will be regarded as having the best predictive ability of BCRIS, and the cut-off value of the variable will be the predictor of BCRIS occurrence. All tests were two-sided. A p-value of 0.05 was considered to be statistically significant. No formal calculation of sample size was performed because of the characteristics of cancer-associated ischemic stroke.
Results
Characteristics of the study population
Sixty BCRIS patients (54 men, and 6 women; mean age, 68.30 ± 11.37 years) were enrolled, accounting for 0.78% of 7739 bladder cancer patients (Figure 1). There were 120 age- and sex-matched patients with active bladder cancer only (i.e. no ischemic stroke) in the control group. Urothelium carcinoma was the most common pathological type of bladder cancer in the BCRIS and control groups. There were no statistically significant differences between BCRIS patients and cancer controls for age, sex, type of bladder cancer pathology, cancer metastasis, or proportion of patients receiving chemoradiotherapy, surgery, or no treatment (Table 1).
Clinical characteristics of patients.

Values are expressed as the mean ± SD or n (%).
†Independent-sample t-test, Mann–Whitney U-test, chi-squared test, or Fisher’s exact test (two-tailed), as appropriate.
Abbreviations: BCRIS, bladder cancer-related ischemic stroke; BC, bladder cancer; PT, prothrombin time; APTT, activated partial thromboplastin time; ALT, alanine transaminase; AST, aspartate transaminase; INR, international normalized ratio; ALB, albumin; Cr, creatinine; UA, uric acid; CRP, C-reactive protein; CEA, carcinoembryonic antigen; CA, cancer antigen; SD, standard deviation.
BCRIS clinical characteristics and biomarkers
After a diagnosis of bladder cancer, an acute ischemic stroke was experienced by 33 (55.00%) patients within the first 6 months, 15 (25.00%) patients at 7 to 12 months, and four (6.67%) patients at >12 months. Eleven of these patients (18.33%) presented with ischemic stroke as the first presentation of occult bladder cancer, which was then diagnosed during stroke therapy. DWI lesion patterns with involvement of multiple arterial territories were observed in 35 BCRIS patients (58.33%) (Figure 2, Table 1), and 37 of 60 (61.67%) had an NIHSS score of 6 to 15 (Table 1). Among the BCRIS patients, three of 60 (5.00%) patients died within the first 30 days. Additionally, 38 (63.33%) BCRIS patients had an mRS score of 0 to 2 at 30 days and 19 of 60 (31.67%) BCRIS patients had an mRS score of 4 to 5 at 30 days. The BCRIS group showed a significantly higher ratio of areas with multiple vessels (bilateral anterior circulation, anterior circulation + posterior circulation, cortex + subcortex) compared with areas with a single-vessel supply (Table 1).

Presentation of multiple lesions in multiple arterial territories on diffusion-weighted magnetic resonance imaging in a 57-year-old man with BCRIS. This patient experienced acute ischemic stroke in the first 6 months after the bladder cancer diagnosis. Imaging shows strong signal changes in the anterior circulation on one side and posterior circulation on both sides. Echocardiography and electrocardiography results were normal.
Compared with cancer controls, BCRIS patients had significantly higher platelet and neutrophil counts, as well as higher D-dimer and CEA serum levels. Other variables were shown to have no significant differences between the two groups. Multivariate binary logistic regression analysis identified the following independent risk factors of BCRIS: elevated D-dimer level (Odds ratio [OR] 1.002, 95% confidence interval [CI] 1.001 to 1.002, P = <0.001), elevated CEA level (OR 1.032, 95% CI 1.011 to 1.054, P = 0.003), and increased platelet count (OR 1.009, 95% CI 1.002 to 1.015, P = 0.007) (Table 2).
Multivariate analysis to identify predictors of BCRIS in Chinese bladder cancer patients.

Abbreviations: CEA, carcinoembryonic antigen; PLT, platelet; NC, neutrophil count; SE, standard error; OR, odds ratio; CI, confidence interval; Df, degrees of freedom.
Predictive analysis of BCRIS
The AUCs obtained with D-dimer and CEA, D-dimer and PLT, and CEA and PLT were not significantly different. The ROC curve of the product of the independent risk factors showed the largest AUC of 0.885 (95% CI 0.836 to 0.935, P < 0.05), indicating that the product of the independent risk factors was a new variable that was a better predictor of BCRIS occurrence compared with each risk factor alone (Figure 3 and Table 3). The optimal ROC cut-off for this new variable was 2,640,745.29, with a sensitivity of 83.3% and specificity of 82.5%.

Receiver operating characteristic (ROC) curves obtained for D-dimer, carcinoembryonic antigen (CEA), and platelet count (PLT) on their own and multiplied together, to predict BCRIS. The largest area under the ROC curve of 0.885 was obtained with the three-way multiplicative product. The optimal cut-off value was 2,640,745.29, and it was associated with a sensitivity of 83.3% and a specificity of 82.5%.
Area under ROC curves for predicting BCRIS.
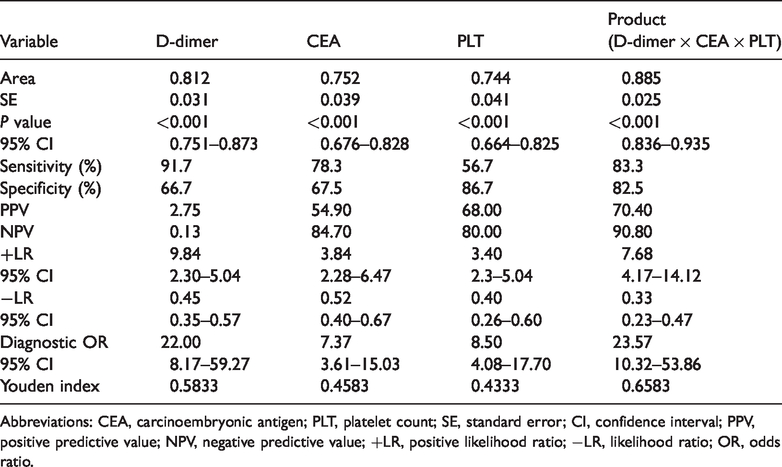
Abbreviations: CEA, carcinoembryonic antigen; PLT, platelet count; SE, standard error; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; +LR, positive likelihood ratio; −LR, likelihood ratio; OR, odds ratio.
Discussion
Cerebrovascular disease is the second most common complication in individuals with tumors. 18 The incidence of ischemic stroke in cancer patients was 3% within 6 months after a cancer diagnosis, which is significantly higher compared with the general population (1.6%).11,19 In this study, the incidence of BCRIS was 0.78% in 7739 hospitalized patients with active bladder cancer from six medical centers in China, indicating that BCRIS deserves more attention. Stroke was frequently an initial manifestation by patients with cancer, and it has also been observed by clinicians in our and other studies.20,21 In the present study, 11 (18.33%) patients without traditional stroke risk factors were initially diagnosed with bladder cancer during their hospitalization for acute ischemic stroke, suggesting that BCRIS could also be the first manifestation of bladder cancer. Additionally, the peak incidence of BCRIS occurred within the first 6 months after the bladder cancer diagnosis, which was similar to CRIS in other studies.11,19 Previous studies showed that ischemic stroke would cause deterioration and poor outcome in patients with cancer.3,22 In the present study, three (5%) BCRIS patients died of ischemic stroke within 30 days of the bladder cancer diagnosis. Therefore, predicting the occurrence of BCRIS in patients with bladder cancer is a clinical challenge.
Many studies have focused on the independent risk factors for CRIS in recent years. Some serum markers, such as elevated serum D-dimer, CA125, and fibrinogen levels were found to be associated with hypercoagulability and are independent risk factors for CRIS.5,6,8 In the present study, we found that elevated serum D-dimer and CEA levels and an increased PLT count were independent risk factors for BCRIS. There is an increasing amount of evidence for elevated serum D-dimer levels in stroke patients with active cancer. Several animal studies showed that cancer cells can release extracellular vesicles into the circulating blood, leading to an increase in D-dimer levels and further triggering the development of microthrombosis, which suggests that cancer could lead to CRIS through the hypercoagulability pathway.15,23 Previous studies showed that elevated serum D-dimer levels were associated with hypercoagulability and CRIS.5,24 Seok et al. 24 reported that the elevated D-dimer level was linearly correlated with the increase in microthrombus signals that were detected by superior and Doppler ultrasound of the internal carotid artery in stroke patients with active cancer; this further confirmed the association between hypercoagulability and CRIS. In the present study, serum D-dimer levels notably increased in BCRIS patients, which also suggested that cancer-mediated hypercoagulability and microthrombosis may play a role in the development of BCRIS.
CEA is a non-specific tumor antigen, and it is highly expressed in serum and urine in bladder cancer patients. In the present study, serum CEA levels were significantly elevated in the BCRIS group compared with the bladder cancer group. Similar results were found in our previous studies.7,9 Increased levels of serum CA125, a type of mucin that is secreted by the cancer cell, were found to be related to hypercoagulability ischemic stroke in patients with cancer. 25 Moreover, autopsy experiments confirmed that there were mucin components that were secreted by cancer cells in the blood vessels, and they were thromboembolic in patients with cancer and ischemic stroke. 11 Additionally, the mucins secreted by carcinoma cells trigger thrombosis, which was shown by reciprocal activation of platelets and neutrophils. 5 Thus, it is suggested that cancer cells could lead to hypercoagulability, which triggers thrombosis in blood vessels and eventually leads to ischemic stroke. Serum CEA is similar to CA125, which is secreted by cancer cells and has similar characteristics. In the present study, it was suggested that elevated serum CEA levels may occur via the above pathway and result in BCRIS. However, the potential mechanisms by which CEA leads to hypercoagulability need to be further investigated.
Platelets can trigger thrombosis in vessels through various pathways. Cancer cells can secrete mucins that activate platelets and endothelial cells to trigger the development of thrombosis. 26 Additionally, carcinoma mucins promote thrombosis through adhesion-dependent and bidirectional signaling in platelets and neutrophils. 27 Cancer directly stimulates neutrophils to release decondensed chromatin, leading to the formation of neutrophil extracellular traps (NETs) that promote microthrombosis.23,28 Thrombus in CRIS was also shown to be platelet-rich, which further confirmed that cancer cell may activate platelets, trigger thrombosis, and eventually lead to ischemic stroke.29,30 The present study showed that BCRIS patients had significantly higher platelets counts and triggered thrombosis by increased platelets, which played a role in BCRIS occurrence.
The above discussion suggests that each risk factor of BCRIS was involved in hypercoagulability and plays a role in BCRIS development. However, the development of BCRIS was more likely to result from the combined effects of these independent risk factors. In this study, the product of the three independent risk factors had the largest area under the ROC curve, and thus, it was the best predictor of the occurrence and development of BCRIS. This indicates that BCRIS occurrence and development may result from the combined effect of independent risk factors. The optimum cut-off value of the three independent risk factors had good sensitivity (83.3%) and specificity (82.5%), which suggests that the occurrence and development of BCRIS may be triggered when the cut-off value of the product is over 2,640,745.29.
Because the pathogenesis of BCRIS is unknown, there is no specific method for its prevention and treatment. However, previous studies showed that hypercoagulability was closely related to the occurrence of cerebral infarction in cancer patients, 24 and use of anticoagulant and antiplatelet drugs may decrease the risk of cerebral infarction in cancer patients. 31 Anticoagulation and antiplatelet drugs may also be effective for BCRIS prevention. For example, in bladder cancer patients with plasma D-dimer levels >2.785 μg/mL, 32 anticoagulants may reduce their risk of BCRIS, and in bladder cancer patients with a history of diabetes, high blood pressure, or high triglycerides, antiplatelet drugs may reduce their risk factors for BCRIS, although the most important factors need to be confirmed in future prospective studies with a large sample size. Additionally, reperfusion therapies including intravenous thrombolysis and embolectomy for acute ischemic stroke patients with active cancer seem to be safe and effective.33,34 Similarly, intravenous thrombolysis and thrombectomy are likely to be appropriate for BCRIS in the acute stage, although supporting studies have not been conducted. However, the effect of reperfusion strategies in BCRIS patients needs to be confirmed in future studies.
Because this study was retrospective and only collected data from active bladder cancer patients with acute ischemic stroke who had no traditional stroke risk factors, a relatively smaller number of cases were included. Clinical data collection that was limited by in-patient treatment requirements have restricted more in-depth discussion about the risk factors for ischemic stroke in patients with bladder cancer, such as sex and lacunar infarction. The previous study showed that there were differences in the distribution of risk factors, stroke subtype, and outcomes between men and women in the traditional stroke population. 35 Additionally, symptomatic cerebral infarcts of the lacunar type have peculiar characteristics with a favorable short-term prognosis. 36 Thus, our findings need to be confirmed by future prospective studies including all bladder cancer patients with acute ischemic stroke with or without traditional stroke risk factors, as well as sex and lacunar infarction.
Conclusions
Elevated serum D-dimer and CEA levels and increased platelet count were independent risk factors for BCRIS, and the cut-off value of the product of these three independent risk factors is ≥2,640,745.29, which could serve as a potential predictor of BCRIS. This may help to predict patients with bladder cancer who are at risk of developing ischemic stroke.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by National Key R&D Program of China (2018YFC1311305), Guangxi Natural Science Foundation (2016GXNSFAA380281), and Open project of Guangxi Key Laboratory of Cardio-Cerebrovascular Disease Prevention and Precision Medicine (GXXNXG201905).