
Abstract
Isolated coronoid process fractures are uncommon, and iatrogenic isolated fractures are extremely rare. This case describes a displaced fracture of an isolated coronoid process thought to be due to excessive force applied by a dentist that had been overlooked and left untreated for about a month. The patient was a woman in her late 50’s and she had undergone a molar extraction. Her dentist had confused her symptoms of trismus, pain, and facial oedema with the complex tooth extraction procedure. Following a cone-beam computed tomography (CBCT) scan we showed that the mandibular coronoid process on her right side had suffered a longitudinal fracture, and the fractured fragment had rotated upwards and inwards. Following successful surgical elimination of the fragmented coronoid process, the patient received targeted physiotherapy sessions that yielded excellent results. At the five-month follow-up, the ability of the patient to open her mouth had improved enormously, and her facial appearance almost recovered to its original state.
Background
Third molar extraction, is the most commonly executed surgical procedure performed by oral surgeons. 1 However, it is not always risk-free and may lead to complications, both intraoperatively or postoperatively. These may include: nerve impairment; bacteraemia; bleeding from ruptured blood vessels; trismus; fractures of the mandibular bony structures.2–5 Of all the facial bones, the mandible is the only robust bone capable of repositioning.6,7 The mandibular ramus subsumes an anteriorly continuous bony eminence on its superior aspect, termed the coronoid process. 8 Two of the four primary masticatory muscles (i.e., masseter and temporalis) are attached to the coronoid process, and some fundamental actions, such as chewing, gulping, and uttering, are facilitated by these muscles thus emphasizing the importance of the coronoid process in morpho-functional dependence. Most common locations of mandibular fractures, include, the condylar process, symphysis, and mandibular angle and rasmus.9,10 However, because the coronoid process is located deep beneath the zygomatic complex and is protected by muscle fibres, rarely does a fracture occur in this location.11,12
Fractures of the coronoid process often occur in conjunction with other bone fractures, primarily zygomatic arch fractures and most result from auto accidents, violence, falls, or sports injuries.12,13 Although extremely rare, 14 iatrogenic isolated coronoid fractures can occur following surgical procedures such as jaw cyst removal, sagittal split ramus osteotomy, or third molar extraction.15–17 Importantly, they can lead to severe outcomes, such as lateral crossbite, Jacob’s disease, pseudo-ankylosis, persistent pain, swelling, and limited mouth opening.
Due to the limited published data on the management and treatment of mandibular coronoid process fracture, oral surgeons have differing views over the methods for treating such fractures. 11 In some circumstances, surgery may be required, particularly for displaced coronoid fractures and for cases that are not eligible for extended maxillo-mandibular fixation. Therapeutic management typically involves intraoral or extraoral surgical approaches, with the former being the preferred method because of its associated low risk of damaging facial nerves and lack of visible scarring. However, limited surgical exposure puts the plexus of the pterygoid and internal maxillary artery at risk of injury. We report here, a case of a displaced fracture of an isolated coronoid process due to excessive force applied by the dentist that was overlooked and left untreated for about a month in a female patient who had undergone a mandibular molar extraction.
Case report
A female patient in her late 50s sought medical attention at Hebei Medical University Hospital of Stomatology in 2021, complaining of trismus, facial oedema on the right side, and severe discomfort. The patient was a non-smoker with no specific medical history and she drank alcohol 2–3 times a week. The patient reported that she had undergone a minor surgical operation to extract her lower right third molar at a private dental clinic a month previously. The surgery had lasted for approximately three hours. Since the operation, she had taken anti-inflammatory drugs prescribed by her dentist to help minimise any swelling in soft tissues. After finding no relief from the medication, she had returned to the dentist for a consultation. The dentist reasoned that it was not uncommon to experience this level of discomfort following a complex procedure and assured her that her symptoms would abate and she would recover within a couple of weeks. She reported that the dentist had not conducted any radiographic examinations following her tooth removal.
During the oral examination conducted by maxillofacial surgeons, her right cheek exhibited significant oedema, and approximately 2 cm of tenderness was observed in the front of her right tragus. Orthopantomographic investigations showed a fracture of the coronoid process on the right side of the mandible, and a slight degree of mobility was observed during intraoral palpation. A cone-beam computed tomography (CBCT) scan showed the coronoid process on the right side had suffered a longitudinal fracture, and the fractured fragment had rotated upwards and inwards (Figure 1(a), 1(b) &1(c)). The patient’s mouth opening was limited to about 1.5 cm (Figure 1(d)). Following collective discussions, our oral surgeons suggested two possible treatment options for the patient:
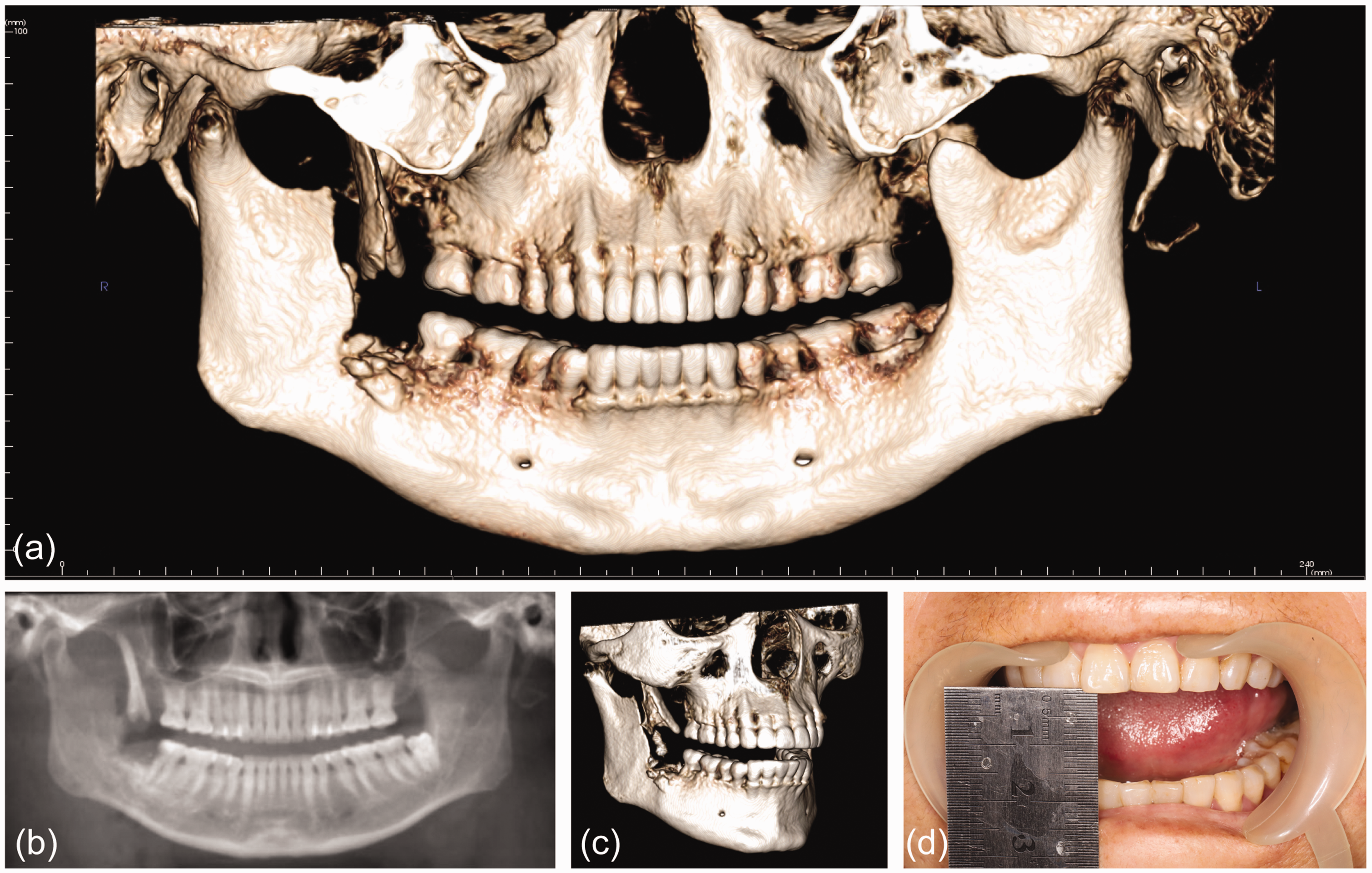
(a & c) Cone-beam computed tomography (CT) images showing the fractured fragment of the coronoid process had rotated upwards and inwards. (b) A panoramic radiographic image shows the coronoid process on the right side had suffered a longitudinal fracture and (d) photograph of the patient’s mouth showing the opening was limited to approximately 1.5 cm.
To achieve an almost normal mandible shape the fractured segments must be reconstructed, and conventional rigid internal fixation must be performed. However, there would be a slight risk of unstable fixation and a potential impact on the trismus.
Removal of the fractured segment. However, this procedure could result in a deviation from the standard mandible shape.
After considering expenses linked to removal of the fixation plates and the significance of preserving her ability to open her mouth, the patient opted for the second treatment option. Due to the significant displacement of the fractured segment, our surgical team made the wise decision to employ an intraoral incision using a pre-ramus approach. During general anaesthesia, before the fracture particle was removed, the patient’s mouth could be opened passively up to 2.5 cm (Figure 2(c)). To access the coronoid component, we made an intraoral pre-ramus incision, removed the detached bone fragment, which had caused temporalis muscle fibrosis and impaired movement, and excised the surrounding temporalis muscle (Figure 2(a) & 2(b)). Following successful surgical elimination of the fragmented coronoid process and achieving adequate haemostasis, under anaesthesia the patient’s mouth could be opened to 4 cm (Figure 2(d)).

(a &b) Images showing that the terminal of the coronoid fragment was made visible during the surgery through an intraoral pre-ramus incision. (c) Before the fracture particle was removed, the passive mouth opening was recorded at 2.5 cm and (d) under general anaesthesia following successful surgical elimination of the fragmented coronoid process and achieving adequate haemostasis, the patient’s mouth was widened to 4 cm.
Postoperative CBCT scans and radiographs confirmed successful surgical elimination of the fragmented coronoid process (Figure 3(a) & 3(b)). For the next month, the patient underwent training and physiotherapy encouraging her to open and close her jaw and at the end of this period her mouth could be opened to 2.5 cm (Figure 3(c)). After five months, there was further progress, with the opening size expanding to 3 cm (Figure 3(d)). Moreover, her ability to clench and chew remained unaffected by the current mouth opening. The patient was free from recurrent trismus, chronic pain, and jaw movement problems and her facial appearance almost recovered to its original state.

(a) Postoperative cone beam computed tomographic (CT) image shows successful surgical elimination of the fragmented coronoid process. (b) A panoramic radiographic image shows that the fractured particle of the coronoid process has been eliminated successfully. (c) One-month post-surgery, the patient’s mouth was able to open to 2.5 cm and (d) after five months post-surgery, the patient’s mouth was able to open to 3 cm.
The reporting of this study conforms to CARE guidelines. 18 The patient provided consent for publication of her anonymised data. Ethical committee approval was not required for this case report.
Discussion
Coronoid process fractures of the lower jaw are uncommon. With estimates ranging from around 2.8% in USA, 1.9% in China and 1.43% of all mandibular fractures in Iran.19–21 Furthermore, isolated coronoid process fractures of iatrogenic origin are even rarer. 10 To our knowledge, there have only been three instances of previously reported cases in the literature.22–24 Our case describes a fourth occurrence. Although, we did not have any pre-extraction radiographic scans, the patient presented to our centre approximately one month after tooth extraction, and so we were able to obtain a reasonably recent orthopantomogram to examine the tooth’s position. As indicated by the alveolar socket image, the tooth’s position was not shallow.
The mandibular angle is the most frequent location for iatrogenic jaw fractures. 9 The cause of these fractures is typically the result of uncontrolled force being applied to teeth during a tooth extraction. 25 This is particularly the case when mandibular-impacted third molars are involved. Due to the third molar occupying the bone space, the angle region of the mandible is susceptible to fractures as it is comparatively weak, and the risk of fracturing the mandibular angle is increased when the third molar is in a deep position. 17 Based on our patient’s history of a mandibular third molar extraction, we diagnosed an iatrogenic fracture of the coronoid process. 14 However, we could not determine the exact direction and strength of the force that had caused the coronoid process fracture. The patient was not able to recall details of the dental procedure she had undergone, and her dentist was not forthcoming with information. Therefore, we were unable to analyse the precise cause of the fracture. However, based on the hypothesis that acute temporalis contraction can cause coronoid process fractures, we had reason to believe that her dentist may have applied excessive force, which had led to an uncontrollable contraction of the temporalis muscle and ultimately resulted in a fracture of the coronoid process. 17
Based on our experience and a literature review, we are of the opinion that treatment for coronoid fractures is influenced by three main factors which are: the fracture’s duration (essential in determining if there is a fibrous connection between the coronoid process and the zygomatic arch); the surgical procedure’s complexity; the patient’s preference. 17 A classification system of mandibular fractures which differentiates between intramuscular and submuscular types, is often used for reference; 26 though to date, there is no consensus on the classification of coronoid process fracture pattern. 17 As a consequence, there is a divergence of opinion on its treatment. 17 For intramuscular fractures, when the coronoid process within the temporalis attachment is fractured and not displaced due to the temporalis muscle traction, the patients exhibit symptoms of limitation or restrictions in their mouth opening or movements that may be overlooked or confused with fractures that can occur in combination with other maxillofacial bones. Some surgeons believe there is no need for surgery in these cases and that conservative treatment such as short maxillomandibular immobilisation, passive exercises, a soft diet, and physiotherapy are sufficient. 27 By contrast, in submuscular fractures, a fracture fragment with superior and medial displacement is a common characteristic; the fragment can be pulled into the infratemporal fossa by the temporalis muscle. In these cases, trismus and facial swelling are common signs, and surgery is the recommended treatment and includes the removal of the fracture fragment, open reduction, and internal fixation. 17 In our case, CBCT scans showed an obvious fracture segment of the coronoid process. Considering the patients other symptoms of trismus and facial oedema we determined that the fracture belonged to the submuscular type, as confirmed during her surgery. For our patient, the degree of temporalis muscle fibrosis and fibrous union between the coronoid process and zygomatic arch were unavoidable due to the duration of the fracture (i.e., four weeks). In addition, she opted for surgery. We removed the fracture fragment, and the patient underwent a consistent passive mouth-opening exercise. At five months post-surgery, the patient had improved mouth opening and masticatory movement. We successfully preserved her bite occlusion, although we did not perform an intermaxillary ligation.
In summary, dental extractions requires precise control over the amount and direction of force the dental surgeon applies. Importantly, any unnecessary force applied to a patient’s jaw could result in a fracture. However, the risk can be minimised if the procedure is performed correctly and confidently. Due to its protected location, fractures of the coronoid process during dental extraction are extremely rare. Nevertheless, it is essential to recognise, that although uncommon, this possibility may occur and dentists should examine patients thoroughly, following surgery. Our case study shows that removal of a fractured coronoid process through an intraoral pre-ramus incision is an efficacious approach for recovery from trismus caused by a displaced bone fragment. Following the operation, physiotherapy and mouth-opening training can significantly relieve muscle spasms caused by the trauma or surgery.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241257446 - Supplemental material for Isolated fracture of the coronoid process following a molar extraction: A rare case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605241257446 for Isolated fracture of the coronoid process following a molar extraction: A rare case report by Anas Ameer Khan, Xiaoyan Zhang, Yue Wang, Xudong Zhang, Xiao Zhang and Xiangjun Li in Journal of International Medical Research
Footnotes
Acknowledgements
We thank the patient and her family for their support of the publication and Prof. Dr. Mei Shuang for her professional opinion on the report.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This study was supported by a grant-in-aid from the Hebei Provincial Health Commission Youth Science and Technology Project (No. 20191082).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.