
Abstract
Objectives
The aim of this study was to investigate the accuracy of electrocardiographic imaging (ECGI) in localizing the origin of outflow tract ventricular arrhythmias (OTVAs) and compare its performance with that of seven published 12-lead electrocardiography (ECG) algorithms.
Methods
Patients with OTVAs who were undergoing catheter ablation were prospectively investigated. The OVTA origins were localized using both ECGI and seven 12-lead ECG algorithms, with the successful ablation site set as the gold standard. The performance of the ECGI and 12-lead ECG algorithms were compared.
Results
Twenty-seven patients were enrolled into the study. The ECGI system correctly identified the chamber of OTVA origin in 27/27 (100%) patients and the sublocalization within the right ventricular outflow tract (RVOT) in 21/22 (95.5%) patients. However, the ECG algorithms correctly diagnosed the chamber and sublocalization in only 21/27 (77.8%) patients and 13/22 (59.1%) patients, respectively, which was significantly lower compared with the ECGI system.
Conclusions
Non-invasive ECGI can accurately predict the origin of OTVAs in a manner that is superior to that of conventional 12-lead ECGs in differentiating the RVOT from the left ventricular outflow tract (LVOT) and septum from free wall in the RVOT. This provides a useful tool to guide catheter ablation.
This trial has been registered in the Chinese Clinical Trial Registry (Registration number: ChiCTR1900025527).
Keywords
Introduction
Idiopathic outflow tract ventricular arrhythmias (OTVAs), which are mainly premature ventricular contractions (PVCs) and ventricular tachycardia (VT), are the most common types of arrhythmias and are usually present without structural heart disease. 1 Frequent OTVA may cause left ventricular dysfunction and even heart failure. 2 Radiofrequency catheter ablation (RFCA) is a safe and effective therapy for idiopathic OTVA. 3 Therefore, it is important to precisely predict the origin of OTVA to define the appropriate strategy and approach before the ablation procedure.
Conventional 12-lead electrocardiograms (ECGs) have been a useful tool for analyzing cardiac arrhythmias, and numerous ECG algorithms for predicting the origin of OTVA have been reported.4–12 However, because of the limited number of electrodes on the body surface, accurate localization of the OTVA origin is limited. This limitation may influence the efficiency and outcome of ablation therapy.
Electrocardiographic imaging (ECGI) is a novel three-dimensional, non-invasive technique for mapping the epicardial electrical activity of the heart. 13 It has the advantage of being able to provide global chamber mapping in a single PVC beat, which suggests its potential role in exploring various cardiac arrhythmias.
The objectives of our study are as follows: first, to compare the accuracy of non-invasive ECGI in estimating the origin of OTVAs with that of conventional ECG algorithms; and second, to directly compare the efficiency of all the proposed 12-lead ECG algorithms in the localization and sublocalization of the OTVA origin.
Methods
Study population
Patients with symptomatic or asymptomatic but frequent (>10,000 per 24 hour) monomorphic PVCs/VT and who were undergoing catheter ablation were prospectively recruited. The exclusion criteria were as follows: (1) failure or abandonment of the ablation procedure; (2) severe cardiac dysfunction; (3) patients with complications including other severe diseases (e.g., hepatic and renal dysfunction, malignant tumor) or contraindications for ablation; and (4) pregnancy. Informed consent was obtained from each participant who was included in the study. All procedures that involved human participants were conducted in accordance with the ethical standards of the institutional research committee (Approved by the Ethic Committee of the First Affiliated Hospital of Zhejiang Chinese Medical University, 15 May 2018) and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Electrocardiographic imaging methods
The computational methods that are used for ECGI have already been described and validated.13,14 Briefly, a 64-electrode vest was applied in our study to the patient’s torso for 5 minutes to record surface potentials, and this was followed by a thoracic computed tomography (CT) scan to construct the three-dimensional heart model from the outline of the heart surface that was extracted from the CT slices. The torso model was created by matching the 64-electrode positions to a standard torso template with 235 triangles of Delaunay triangulation. 15 The mathematical method of the ECGI procedure was also described in our previous study. 15 Briefly, a novel framework based on low-rank and sparse decomposition (LSD) + total variation (TV) was proposed to reconstruct the cardiac electrical activity of PVCs/VT based on the surface potential data and geometrical information. The origin of the PVCs/VT was then prospectively localized via the reconstructed cardiac potential maps.
Twelve-lead ECG algorithms
Seven 12-lead ECG algorithms were selected to compare the accuracy of predicting the origin of OTVAs. All the proposed 12-lead ECG algorithms are summarized in Table 1. Briefly, all the algorithms localize the origin to either the left ventricular outflow tract (LVOT) or the right ventricular outflow tract (RVOT), and the algorithms published by Zhang et al. 12 and Ito et al. 7 provide additional criteria for further sublocalization within the RVOT (septum vs. free-wall). The analysis was retrospectively performed by two electrophysiologists using each of the proposed algorithms to identify the origin. Both the examiners were blinded to the previously established diagnosis, ECGI data, and ablation outcomes. Disagreements between the two examiners were resolved by a third electrophysiologist based on the majority rule principle. The interobserver variability was also tested. To directly compare the performance between ECGI and 12-lead ECG, the exclusive diagnosis for each patient in whom there was a differentiation between the RVOT and the LVOT was also established based on the seven ECG algorithms and the majority rule principle. To compare the sublocalization values within the RVOT between the two ECG algorithms and ECGI, only patients who were diagnosed as having the origin in the RVOT using an electrophysiological (EP) study were further analyzed.
Published 12-lead ECG algorithms to localize the origin of OTVAs.

RVOT, right ventricular outflow tract; LVOT, left ventricular outflow tract; OTVA, outflow tract ventricular arrhythmia; PVC/VT, premature ventricular contraction/ventricular tachycardia; LBBB, left bundle branch block; ASC, aortic sinus cusps.
Electrophysiological study and ablation
All patients underwent an invasive EP procedure. Antiarrhythmic drugs were discontinued at least 48 hours before the invasive EP study. The invasive EP study was guided by the Ensite NavX/Velocity mapping system (St. Jude Medical, Saint Paul, MN, USA). Depending on the suspected location of the OTVAs (RVOT or LVOT), one 7F vascular sheath was inserted into the right femoral vein or 8F vascular sheath was inserted into the right femoral artery after local anesthesia. A standard irrigated-tip therapy Cool Path Duo ablation catheter (St. Jude Medical) was applied. Power delivery ranged from 30 to 40 W with a maximum temperature limited to 60°C for the RVOT and the LVOT. Left-sided mapping was performed via the retrograde transaortic approach with systemic heparinization under the targeted activated clotting time of >250 seconds. Acute ablation success was defined as no recurrence of spontaneous or induced PVCs/VT within 30 minutes after the last ablation with or without isoprenaline infusion.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics for Windows (version 20.0; IBM Corp., Armonk, NY, USA). Continuous variables are presented as the mean ± standard deviation (SD). Categorical variables are expressed as counts and percentages. Baseline characteristics were compared using the χ2 test for categorical variables and the Mann–Whitney U test for continuous variables. The differences in the accuracies between the ECGI and ECG algorithms and those for the seven ECG algorithms were evaluated using McNemar’s tests. Kappa coefficients were also calculated to assess the interobserver agreement for all seven ECG algorithms. Kappa values ≥0.75 were considered to represent adequate agreement. A p value <0.05 was considered to be statistically significant.
Results
Patient characteristics
Twenty-seven patients with OTVAs were enrolled into this study. Patient clinical characteristics are summarized in Table 2. Acute procedural successes were achieved for all the included patients. Ablation was delivered at 22 RVOT sites, including 19 RVOT septum sites, three RVOT free wall sites, and five LVOT sites. Based on the successful PVCs/VT ectopy ablation site, the patients were divided into the RVOT group or the LVOT group.
Patients’ clinical characteristics.

RVOT, right ventricular outflow tract; LVOT, left ventricular outflow tract; PVC, premature ventricular contraction; LVEF, left ventricular ejection fraction; LVIDd, left ventricular internal dimension diastole; LVIDs, left ventricular internal dimension systole; LAd, left atrial diameter; SD, standard deviation.
Localization accuracy of ECGI and comparison with the 12-lead ECG algorithms
All clinical PVCs/VT were recorded before the EPS and ablation procedure by the ECGI system, and the 3D electroanatomic maps were reconstructed for all patients, which were then applied to localize the origin of OTVA ectopy (Figure 1).

ECGI map of PVCs that originated from the RVOT septum and its comparison with the successful site of ablation.
The OTVA chamber was correctly identified in 27/27 (100%) patients and the sublocalization within the RVOT was achieved in 21/22 (95.5%) patients using the ECGI procedure. The sensitivity and specificity were both 1.00 for ECGI for differentiating between RVOT origins and LVOT origins, and these parameters were 0.95 and 1.00 for sublocalization of the septum and free-wall, respectively, within the RVOT. For 20/27 patients who had a V3 transition in the ECG, the OTVA chamber was correctly diagnosed in 20/20 (100%) patients and the sublocalization was also correctly diagnosed within the RVOT in 19/20 (95.0%) patients using the ECGI method. One failed sublocalization (patient 22) in the ECGI group predicted an origin site in the RVOT free wall, but the OTVA was ablated successfully at the RVOT septum. However, compared with the ECGI procedure, the chamber was correctly identified in only 21/27 (77.8%) patients (p = 0.041) and the sublocalization was correctly localized in 13/22 (59.1%) patients (p = 0.027) using the ECG algorithm (Table 3).
Localization accuracy of ECGI and comparison with that of 12-lead ECG algorithms.
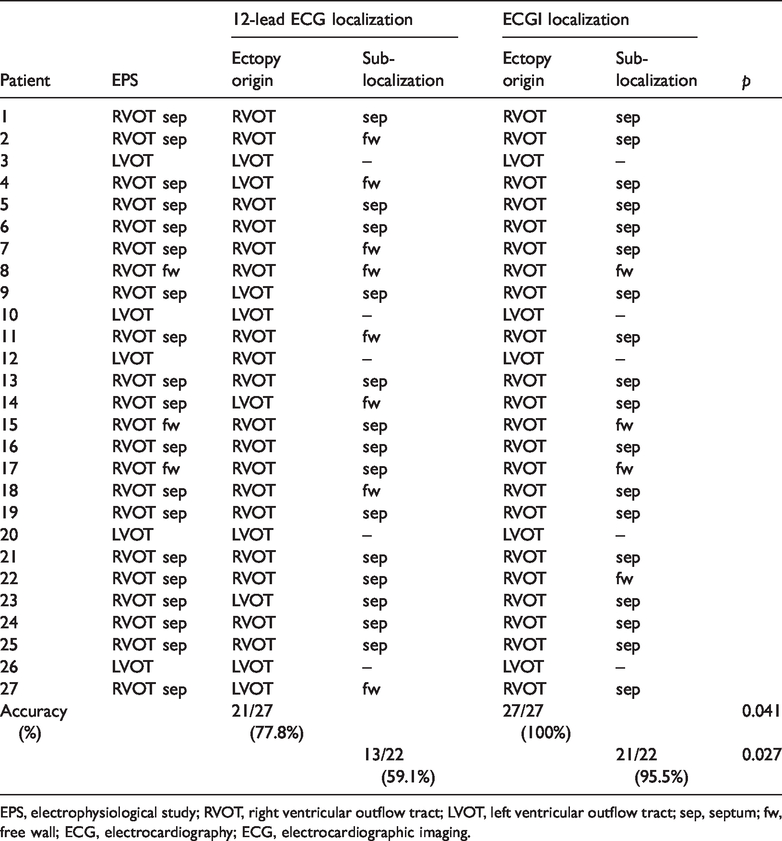
EPS, electrophysiological study; RVOT, right ventricular outflow tract; LVOT, left ventricular outflow tract; sep, septum; fw, free wall; ECG, electrocardiography; ECG, electrocardiographic imaging.
In addition, the receiver operating characteristic (ROC) curve analysis regarding the predictive value of ECGI and the seven ECG algorithms for differentiating the LVOT from the RVOT arrhythmias was conducted. The results showed a similar diagnostic accuracy among the seven ECG algorithms, with areas under the curve (AUCs) ranging from 0.69 to 0.86, but there was a significantly higher accuracy for ECGI, which had an AUC of 1.00 (p < 0.05; Figure 2).

ROC analysis for the predictive value of ECGI and seven ECG algorithms for differentiating between the RVOT and the LVOT.
Comparison of the predictive value of the seven 12-lead ECG algorithms for differentiating between the RVOT and LVOT
The seven ECG algorithms were assessed for their diagnostic accuracy, specificity, sensitivity, and likelihood ratios (LRs) of differentiating between the RVOT and LVOT to determine the origin of PVCs/VT. The results are summarized in Table 4. Assessment of the diagnostic accuracy showed that each of the seven algorithms had only moderate accuracy, and the greatest accuracy was observed in the algorithm proposed by Yoshida 10 . However, when the algorithms were compared for their accuracy, specificity, sensitivity, and LRs, no significant differences were found.
Overall diagnostic accuracy of seven 12-lead ECG algorithms for differentiating the RVOT from the LVOT, and the specificity, sensitivity, positive and negative likelihood ratios for differentiation.

LR(+), positive likelihood ratios; LR(−), negative likelihood ratios.
The interobserver agreement between the two independent electrophysiologists in localizing between the RVOT and LVOT was calculated for all the ECG algorithms. The algorithm published by Yoshida 10 had the highest kappa value of 1.00, and acceptable kappa values of 0.886 and 0.836 were obtained for algorithms proposed by Yoshida 11 and Ouyang 9 , respectively. However, poor interobserver agreements, with kappa values ranging from 0.625 to 0.697, were detected for algorithms proposed by Cheng, 5 Betensky, 4 Zhang 12 , and Ito 7 (Table 5).
Interobserver agreements between ECG algorithms.

RVOT, right ventricular outflow tract; LVOT, left ventricular outflow tract.
Sublocalization within the RVOT: Septum vs. free wall
The ECG algorithms proposed by Zhang et al. 12 and Ito et al. 7 provide criteria for sublocalization of the origin in the RVOT septum compared with the RVOT free wall. The accuracy of the ECG algorithm proposed by Zhang et al. 12 was significantly higher compared with that proposed by Ito et al. 7 , and there were significant differences in specificity, sensitivity, and positive and negative LRs between these two algorithms (p = 0.039) (Table 6). However, poor interobserver agreement was detected for the algorithm by Zhang 12 , which had a kappa value of 0.252, and this is much lower compared with the algorithm by Ito 7 (kappa value, 0.636) (Table 5).
Accuracy, specificity, sensitivity, positive, and negative likelihood ratios of two ECG algorithms in sublocalization within the RVOT: septum vs. free wall.

aMcNemar’s test.
LR(+), positive likelihood ratios; LR(−), negative likelihood ratios; RVOT, right ventricular outflow tract; ECG, electrocardiography.
Discussion
The results of our study showed that non-invasive ECGI had better accuracy compared with that of the conventional 12-lead ECG algorithm for identifying the origin of OTVAs.
Comparison of the seven different ECG algorithms in localizing the origin of OTVAs
In the “head-to-head” comparison, all the seven published 12-lead ECG algorithms for OTVA differentiation were similar in terms of the diagnostic accuracy, specificity, sensitivity, and LRs. The predicted accuracy of the ECG algorithms in our study ranged from 74.1% to 88.9%, the specificity ranged from 60% to 80%, and the sensitivity ranged from 77.3% to 90.9%, all of which were lower compared with results that were previously reported by their authors.4,5,7,9–12
Possible explanations for the lack of reproducibility may be the differences in the population and the heterogeneity between the assessors in the present study and the developers of a particular algorithm because four of the seven ECG algorithms exhibited poor interobserver agreement.
To the best of our knowledge, the specificity, sensitivity, and LRs of the published ECG algorithms for determining the OTVA origin have not been tested in a “head-to-head” comparison. The positive and negative LRs of a particular algorithm that is used to diagnose the OTVA origin may have clinical value by providing a comprehensible measurement of the strength that is required to reach a diagnosis. 16
Recently, some new algorithms were also proposed, such as the QRS morphology pattern in V5R, 12 synthesized right-sided chest lead electrocardiography, 8 and the QRS-RVA interval during an electrophysiology study, 17 all of which focused on parameters that are beyond the conventional 12-lead ECG algorithm and provide more tools to help physicians reach an accurate diagnosis.
Two ECG algorithms in our study provide further criteria for sublocalization of the RVOT septum compared with the RVOT free wall. The ECG algorithm proposed by Zhang et al. 12 was found to be superior to that proposed by Ito et al. 7 in terms of the specificity, sensitivity, LR(+), and LR(−). However, the algorithm proposed by Zhang et al. 12 exhibits a significantly low kappa value of 0.252, suggesting poor interobserver agreement. The accuracy of both algorithms was lower in our study compared with that in its origin study7,12 and in studies that were recently published on differentiating between the origin sites within the RVOT.16,18 Thus, the results should be interpreted with caution.
Limitations of the ECG algorithms and conventional mapping methods
There are some limitations that are associated with using the 12-lead ECG algorithms that were found in this study or reported in previous studies.8,16,19 For example, several algorithms require an accurate measurement of many ECG parameters, and thus, inconsistencies and heterogeneities between assessors may be inevitable, especially with wandering baselines, lead noise, and lack of electronic calipers.8,16,19 The spatial relationship between the heart and torso among different patients and variable precordial lead placements could further lead to inaccuracies in ECG algorithms.
In addition, in some proposed ECG algorithms, the sinus rhythm and QRS-wave that precede the PVCs/VT are essential, which could limit their clinical application. Additionally, for the algorithms of sublocalization within the RVOT, the steps to reach a certain diagnosis increased significantly, which could result in more extensive errors and heterogeneity. All the erroneous predictions of the OTVA origin that used a 12-lead algorithm may result in inappropriate ablation approaches and negatively affect its effectiveness.
Some limitations of conventional mapping techniques during the procedures may also worsen the ablation outcome, including poor spatial resolution of pace mapping, in scenarios where spontaneous ectopy is infrequent, or when there is difficulty in inducing tachycardia.
The newly developed invasive noncontact three-dimensional mapping systems, such as Ensite and CARTO, provide new platforms for mapping cardiac arrhythmias in three dimensions. They provide accurate visualization of the OTVA origin in a complex three-dimensional substrate, which greatly increases the success of ablation and reduces the procedure time. However, it requires systemic heparinization, even in the right ventricle, which increases the risk of bleeding complications. In addition, only a single chamber can be mapped at a time in a point-by-point manner.
Efficacy and advantages of ECGI in localizing OTVA origin and its clinical impact
ECGI had a high accuracy of 100% in chamber localization and 95.5% in sublocation within the RVOT to determine the OTVA origin. These results are similar to those in a previously published study by Jamil-Copley et al., 19 which assessed the performance of electrocardiographic mapping in locating the origin of outflow tract ventricular tachycardia using the Tikhonov regularization method and the generalized minimal residual iterative technique. However, we proposed a novel mathematical method for ECGI and directly compared the performance of ECGI with that of seven published ECG algorithms, demonstrating the superiority of ECGI.
For patient 22, the ECGI system suggested an OTVA origin in the RVOT free wall, but the ablation site was in the RVOT septum. These two locations are quite close to each other. This incorrect result may be caused by the ill-posed nature of the spatiotemporal ECG-inverse problem in ECGI using our improved potential-based method. Thus, the potential-to-activation transformation method should be further optimized in our mapping algorithm to improve its accuracy.
Because ECGI is a unique method and each patient’s own heart–torso model is used, the limitations of the 12-lead ECG that result from individual variability and variable lead placement could be addressed to some extent, especially for patients who had a V3 transition in the ECG and underlying structural cardiac abnormalities. ECGI can localize the PVC origin within only one heartbeat, and both ventricles can be mapped simultaneously, exhibiting its advantage in mapping infrequent OTVA. Additionally, it is a non-invasive method that could be a useful tool to study the mechanisms of various complicated arrhythmias such as atrial fibrillation.
The ECGI system could also contribute to planning the ablation strategy regarding the appropriate arterial or venous vascular access, which may reduce the risk of complications. Additionally, the high accuracy of ECGI can greatly simplify the mapping process, potentially reduce the procedural and fluoroscopic time, and improve clinical outcomes, resulting in greater clinical utility.
Some limitations should be noted. First, complete predictive accuracy should not be expected because ECGI is still in the early stages of development. Second, the increased overall radiation exposure should be taken into account because CT scanning is currently required for the system, and this should be weighed against all the benefits. Cardiac magnetic resonance imaging (MRI) could replace CT scanning in the future, which may further reduce CT-related high radiation exposure. Finally, ECGI mainly provides the epicardial activation maps, but they are not always identical to the endocardial activation maps. To directly compare the ECGI and ECG performance, the localizing ability of ECGI was limited to left ventricle or to two segments in the right ventricle, and the precise site was not further assessed.
The small patient group in our study may, to some extent, affect the results of both the comparison among 12-lead ECG algorithms and between ECG algorithms and ECGI in predicting the OTVA origin because not all the possible ectopies were included, especially those from the aortic sinus cusps or epicardium, and only five patients with a LVOT origin were included. However, non-invasive ECGI was still shown to have good accuracy and better performance compared with the 12-lead ECG algorithms, especially in patients with symptomatic but infrequent OTVAs.
Conclusions
The seven published 12-lead ECG algorithms have similar and moderate accuracy in the localization of OTVA origin, while the non-invasive ECGI can accurately differentiate between the RVOT and the LVOT and between the septum and free wall in the RVOT, which outperforms the conventional 12-lead ECG.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research was supported by the Zhejiang Provincial Key Research and Development Project of China [grant number 2015C03041] to W.M., and the Zhejiang Provincial Research Project of Public Welfare Technology [grant number LGF19H020003] and the Zhejiang Provincial Medical Science and Technology Foundation of China [grant number 2017KY507] to X.Z.