
Abstract
Objective
Serum chloride disorders have been gaining increased attention. We aimed to assess the impact of serum chloride on all-cause mortality in critically ill patients in coronary care units (CCUs).
Methods
We extracted clinical data from the Multiparameter Intelligent Monitoring in Intensive Care III database. We used data for the first CCU admission of each patient; baseline data were extracted within 24 hours after CCU admission. Statistical methods included the Lowess smoothing technique, Cox proportional hazards model, and subgroup analyses.
Results
A total 5616 patients who met the inclusion criteria were included. We observed a U-shaped relationship between admission chloride levels and 30-day all-cause mortality. In multivariate analysis adjusted for age, ethnicity, and sex, both hyper- and hypochloremia were significant predictors of risk of 30-day, 90-day, and 365-day all-cause mortality. After adjusting additional clinical characteristics, hypochloremia remained a significant predictor of risk of 30-day all-cause mortality (hazard ratio, 1.47; 95% confidence interval, 1.19–1.83). For 90-day and 365-day all-cause mortality, similar significant robust associations were found.
Conclusions
We observed a U-shaped relationship between admission chloride levels and 30-day all-cause mortality among patients in the CCU. Hypochloremia was associated with increased risk of all-cause mortality in these patients.
Keywords
Introduction
Electrolyte disturbances in potassium, calcium and magnesium have been shown to be risk factors for mortality in critically ill patients.1,2 Recently, serum chloride disorders have been gaining increased attention. Chloride is the most abundant anion in the extracellular fluid, 3 and it has an important role in physiology. Movement of chloride through cell membranes involves regulation of cell volume, smooth muscle cell contraction, and synaptic transmission. 4 There is sufficient evidence that extracellular chloride plays a pivotal role in the regulation of macula densa renin secretion in the kidneys, 5 and this is independent of Na+ and water content. 6 Therefore, serum chloride is involved in acid–base balance, muscle activity, and immune regulation. 7
Several studies have focused on the relationship between serum chloride levels and acute kidney injury (AKI).8,9 There is also evidence that hyperchloremia in critically ill septic patients is associated with mortality.10–12 Van Regenmortel and colleagues 13 found that hyperchloremia at admission was significantly associated with increased 30-day intensive care unit (ICU) and hospital mortality. Recently, several clinical studies showed serum chloride was an independent prognostic marker for mortality in patients with cardiovascular disease, including acute or chronic heart failure14,15 and hypertension. 16 Nevertheless, to our knowledge, there has been no study exploring the association between serum chloride and mortality in coronary care unit (CCU) patients. The aim of this study was to assess the impact of serum chloride on all-cause mortality in critically ill patients in the CCU.
Methods
Data source
The Multiparameter Intelligent Monitoring in Intensive Care III database version 1.4 (MIMIC-III v1.4) includes more than 38,000 patients in the intensive care unit (ICU) of Beth Israel Deaconess Medical Center in Boston, Massachusetts, United States (US) from 2001 to 2012. 17 Our access to the database was approved by the institutional review boards of the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center after we completed the National Institutes of Health’s web-based course and passed the Protecting Human Research Participants exam.
This study is based on data from the MIMIC-III v1.4. We used the PostgreSQL tool (version 9.6) to extract clinical data, including patient demographics, laboratory test results, mortality, and other clinical variables. The information of included patients was hidden to protect privacy and the project was granted a waiver of an ethics review and informed consent.
Population selection criteria
The database includes 38,645 adult patients (≥16 years of age). Eligible patients were those who were hospitalized in the critical care unit (CCU) at their first admission for more than 2 days. Patients were excluded with the following criteria: 1) no serum chloride measured during their CCU stay; 2) missing >5% individual data.
Data extraction
The extracted data included demographic parameters, clinical parameters, laboratory parameters, and scoring systems. Only the data for the first CCU admission of each patient were used, and baseline data were extracted within 24 hours after CCU admission. Comorbidities included coronary artery disease (CAD), congestive heart failure (CHF), atrial fibrillation (AFIB), stroke, renal disease, liver disease, valvular disease, endocarditis, peripheral vascular disease, hypertension, uncomplicated diabetes, chronic obstructive pulmonary disease (COPD), cardiac arrhythmias, respiratory failure, and acute respiratory distress syndrome (ARDS). Laboratory measurements included bicarbonate, creatinine, hemoglobin, glucose, hematocrit, platelet, sodium, blood urea nitrogen (BUN), white blood cells (WBC), and potassium. Sequential Organ Failure Assessment (SOFA) score 18 and Simplified Acute Physiology Score II (SAPSII) 19 were obtained at the time of CCU admission. Survival information regarding vital status was obtained from the US Social Security death index records. The endpoints for this analysis were 30-day, 90-day and 365-day mortality.
Statistical analysis
We divided chloride levels into three groups based on the normal range for chloride in a previous study: hypochloremia (<98 mmol/L), normochloremia (98–107 mmol/L), and hyperchloremia (≥107 mmol/L). 13 Baseline characteristics of all patients were stratified according to these three groups; continuous variables are presented as mean ± standard deviation (SD) or median and interquartile range (IQR). Categorical data are summarized as number or percentage and were compared using the chi-squared test. The Lowess smoothing technique was used to examine the relationship between serum chloride and 30-day mortality in logit scale. 20 To facilitate clinical interpretation of our results, we used Cox proportional hazards models to determine whether serum chloride was independently associated with 30-day, 90-day, and 365-day all-cause mortality, with results presented as hazard ratios (HRs) with 95% confidence intervals (CIs).
We used two multivariate models for each endpoint. The normochloremia group was considered the control group. In model I, covariates were adjusted for age, ethnicity, and sex. In model II, covariates were adjusted for age, ethnicity, sex, creatinine, hematocrit, platelets, sodium, glucose, blood urea nitrogen, systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate, respiration rate, oxygen saturation (SPO2), SAPSII, SOFA, CHF, uncomplicated diabetes, AFIB, liver disease, CAD, stroke, COPD, and respiratory failure. We selected these confounders based on a change in effect estimate of more than 10%.
We performed stratification analyses to assess the association between serum chloride and 30-day all-cause mortality, including CHF, diabetes, AFIB, CAD, stroke, COPD, respiratory failure, liver disease, heart rate, respiratory rate, SBP, DBP, temperature, SPO2, creatinine, hematocrit, platelets, sodium, BUN, glucose, SOFA score, and SAPSII score. The data were analyzed using EmpowerStats version 2.17.8 (http: //www.empowerstats.com/cn/) and R software version 3.42 (The R Project for Statistical Computing, Vienna, Austria). P < 0.05 was considered statistically significant and all reported P-values were two-sided.
Results
Participant characteristics
A total of 5616 patients who met the inclusion criteria were divided into three groups according to the normal range for chloride: there were 795 patients in the hypochloremia group, 3472 patients in the normochloremia group, and 1439 patients in the hyperchloremia group. Characteristics of the study patients according to serum chloride levels are displayed in Table 1. Patients who were white and male had a higher proportion of CCU hospitalizations. Patients with hypochloremia were more likely to be older; have faster respiratory and heart rates; higher bicarbonate, creatinine, glucose, and BUN; higher SOFA and SAPSII scores; higher mortality; and higher comorbidities of CHF, AFIB, renal disease, liver disease, hypertension, diabetes, COPD, cardiac arrhythmias, and respiratory failure.
Characteristics of study participants, according to serum chloride levels

Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; SOFA, Sequential Organ Failure Assessment; SAPSII, Simplified Acute Physiology Score II.
Chloride levels and clinical endpoints
The relationship between admission chloride levels and logit-transformed 30-day all-cause mortality was non-linear (Figure 1). We observed a U-shaped relationship, suggesting that both hyper- and hypochloremia were associated with equally increased risk of 30-day all-cause mortality.

Relationship between serum chloride and logit-transformed mortality using the Lowess smoothing technique.
In multivariate analysis, adjusted for age, sex, and ethnicity, both admission hyper- and hypochloremia were significant predictors of risk of 30-day, 90-day and 365-day all-cause mortality. The corresponding adjusted HRs (95% CIs) for hypochloremia compared with normochloremia were 2.28 (1.91, 2.72), 2.27 (1.95, 2.64), and 2.15 (1.89, 2.45), respectively. Similarly, the corresponding adjusted HRs (95% CIs) for hyperchloremia were 1.40 (1.17, 1.66), 1.21 (1.04, 1.41), and 1.16 (1.03, 1.32), respectively. After adjusting for age, ethnicity, sex, creatinine, hematocrit, platelets, sodium, glucose, blood urea nitrogen, heart rate, SBP, DBP, respiration rate, SPO2, SAPSII, SOFA, CHF, uncomplicated diabetes, AFIB, liver disease, CAD, stroke, COPD and respiratory failure, we found that hypochloremia remained a significant predictor of risk of 30-day all-cause mortality (HR, 1.47; 95% CI, 1.19 to 1.83; P=0.0004). In 90-day and 365-day all-cause mortality, similar significant robust associations were found. Nevertheless, hyperchloremia was not independently associated with these clinical endpoints (Table 2).
Hazard ratios (HRs) and 95% confidence intervals (CIs) for mortality across groups of serum chloride.
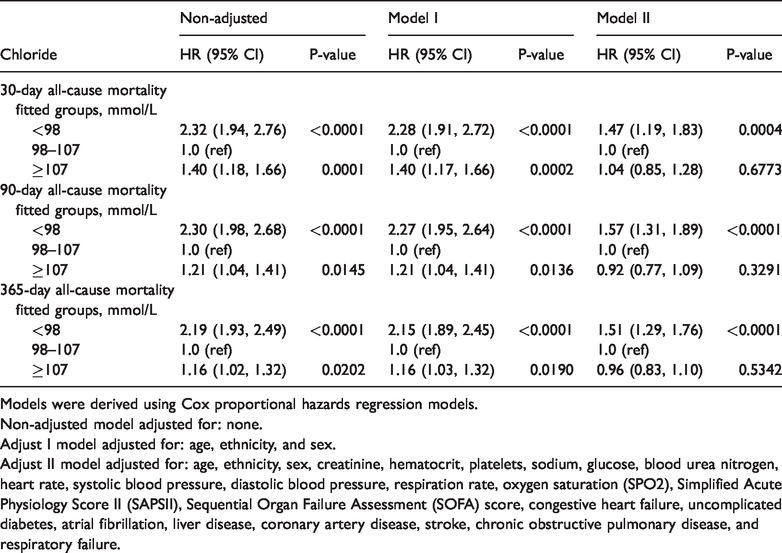
Models were derived using Cox proportional hazards regression models.
Non-adjusted model adjusted for: none.
Adjust I model adjusted for: age, ethnicity, and sex.
Adjust II model adjusted for: age, ethnicity, sex, creatinine, hematocrit, platelets, sodium, glucose, blood urea nitrogen, heart rate, systolic blood pressure, diastolic blood pressure, respiration rate, oxygen saturation (SPO2), Simplified Acute Physiology Score II (SAPSII), Sequential Organ Failure Assessment (SOFA) score, congestive heart failure, uncomplicated diabetes, atrial fibrillation, liver disease, coronary artery disease, stroke, chronic obstructive pulmonary disease, and respiratory failure.
Subgroup analyses
We conducted subgroup analyses to investigate the associations between serum chloride and 30-day all-cause mortality (Table 3). We observed significant interactions with CHF (P for interaction: 0.0009). Both hypochloremia and hyperchloremia were linked to mortality in patients with CHF.
Subgroup analysis of the associations between serum chloride and 30-day all-cause mortality.

Abbreviations: CHF, congestive heart failure; AFIB, atrial fibrillation; CAD, coronary artery disease; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Discussion
We observed a U-shaped relationship between admission chloride levels and logit-transformed 30-day all-cause mortality. After adjusting for age, ethnicity, sex, creatinine, hematocrit, platelets, sodium, glucose, blood urea nitrogen, heart rate, SBP, DBP, respiration rate, SPO2, SAPSII, SOFA, CHF, uncomplicated diabetes, AFIB, liver disease, CAD, stroke, COPD, and respiratory failure, we observed that hypochloremia was associated with increased risk of 30-day, 90-day and 365-day all-cause mortality in critically ill patients in the CCU. To our knowledge, this is the first such study in a broad CCU population.
Body chloride is primarily derived from diet, and is mainly excreted by sweat and kidneys. Chloride accounts for about one-third of the tonicity and two-thirds of all negative charges in plasma. 21 It is a cationic buffer that includes acids and sodium, playing an important role in the ability of the kidney to remove salt and water. 7 The relationship between serum sodium and adverse outcomes has been the subject of many previous studies.22,23 In contrast to sodium, chloride may have a stronger prognostic effect because it has a broader homeostatic role, and deregulation of chloride results in a wide range of abnormalities. 24 For example, chloride overload is significantly associated with the development of acute kidney injury, 25 and the mechanism for this process may be owing to hyperchloremia causing vasoconstriction of afferent arterioles, lowering renal blood flow velocity and cortical perfusion.26,27
Given the growing body of literature demonstrating the importance of chloride, we conducted research relevant to this issue. We evaluated the importance of the effects of serum chloride on outcomes among patients in the CCU. After adjustment for various clinical characteristics including sodium, we found that hypochloremia was a particularly unfavorable prognostic indicator for CCU patients. This is consistent with previously reports of hypochloremia as an independent prognostic marker for mortality in patients with heart failure14,15 and hypertension. 16 Nevertheless, our results differed from those of a retrospective cohort study in which hyperchloremia was linked to increased mortality in critically ill patients in a mixed intensive care population. 13 This discrepancy may be related to the difference in the composition of diseases between the CCU and a mixed ICU.
Our study had several limitations. First, this study had a single-center retrospective design with inherent biases; selection bias cannot be ignored. Second, we extracted data for chloride in patients only upon admission to the CCU and did not assess changes during the CCU stay. Third, although we used a multivariate model to control bias, there remain numerous other known and unknown factors. Finally, data pertaining to the treatment of chloride disorders before CCU admission were unavailable, which may affect the reliability of the results.
Conclusions
We observed a U-shaped relationship between admission chloride levels and 30-day all-cause mortality among patients in the CCU. Hypochloremia was associated with increased risk of all-cause mortality in these patients. Nevertheless, these conclusions need to be confirmed in large prospective multicenter studies.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520911500 - Supplemental material for Hypochloremia is associated with increased risk of all-cause mortality in patients in the coronary care unit: A cohort study
Supplemental material, sj-pdf-1-imr-10.1177_0300060520911500 for Hypochloremia is associated with increased risk of all-cause mortality in patients in the coronary care unit: A cohort study by Zongying Li, Cheng Xing, Tingting Li, Linxiang Du and Na Wang in Journal of International Medical Research
Footnotes
Data availability
The clinical data used to support the findings of this study were obtained from the Multiparameter Intelligent Monitoring in Intensive Care III database version 1.4 (MIMIC-III v.1.4). Although the database is publicly and freely available, researchers must complete the National Institutes of Health’s web-based course, known as Protecting Human Research Participants, to apply for permission to access the database.
Disclosure
The funders of the project were not involved in study design, collection, data analysis, writing of the report, or publication.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.