
Abstract
Compared with monopolar transurethral resection of the prostate (TURP), which requires electrolyte-free irrigation fluid, normal saline can be used as the irrigation solution in bipolar and laser TURP. The risk of TURP syndrome and severe electrolyte disturbance is minimized when normal saline is used as the irrigation fluid. However, the use of isotonic saline also causes acid-base imbalance and electrolyte disturbance. We experienced two patients who developed hyperchloremic metabolic acidosis during bipolar TURP. After proper intervention, hemodynamic instability resolved, and laboratory test results normalized. Anesthesiologists must pay attention to acid-base and electrolyte status when rapid absorption of excessive isotonic solution is suspected, even during bipolar and laser TURP, which use normal saline as the irrigation fluid.
Keywords
Introduction
Transurethral resection of the prostate (TURP) is a treatment option for benign prostatic hyperplasia (BPH), and this procedure has recently undergone various methodological advancements. Monopolar TURP requires an electrolyte-free solution for bladder irrigation because the energy dispersed from the monopolar electrode uses the body as a conduit. Excessive absorption of hypoosmolar irrigation fluid causes hypervolemia, hyponatremia, and TURP syndrome in severe cases.1,2
During bipolar and laser TURP, normal saline can be used as the bladder-irrigating fluid, and improved hemostasis and minimized risk of TURP syndrome have led urologists to adopt these approaches. Although the risk of TURP syndrome is minimized with bipolar and laser TURP, rapid absorption of normal saline could lead to hyperchloremic metabolic acidosis. This report describes two patients who developed hyperchloremic metabolic acidosis during bipolar TURP.
Case report
Case 1 involved a 79-year-old man with hypertension. Preoperative laboratory testing revealed the following: pH, 7.467; base excess (BE), −0.6; hemoglobin (Hb), 111 g/L; sodium (Na), 136 mmol/L; and chloride (Cl), 100 mmol/L. Preoperatively, the prostate was estimated to weigh 94.1 g. General anesthesia was chosen for TURP, and 1 hour after the operation started, the patient’s blood pressure decreased rapidly, following which, 5 mg ephedrine was injected. Because of persistent hemodynamic instability despite ephedrine administration, a phenylephrine infusion was initiated. An arterial line was placed for continuous blood pressure monitoring and for blood collection for laboratory testing. The laboratory test results are shown in Table 1 (pH, 7.074; BE, −14.3; Hb, 93 g/L; Na, 140 mmol/L; Cl, 120 mmol/L; and calcium (Ca), 0.22 mmol/L). We administered 60 mEq of sodium bicarbonate, 300 mg of calcium chloride, and 10 mg of furosemide, and monitored electrolytes. In addition, two units of packed red blood cells were transfused because of persistent bleeding. The prostatic capsule was perforated during the procedure. The estimated blood loss was 600 mL, total operation time was 130 minutes, resected prostate weight was 57 g, and irrigation fluid volume was 47 L. The patient was transferred to the intensive care unit (ICU) after surgery and remained there overnight. Bladder irrigation via an indwelling urethral catheter was ongoing. At the time of transfer from the ICU, the acidosis had resolved, and the Hb level was normal at 100 g/L. The patient was transferred to a general ward and remained in hospital for another 7 days.
Laboratory test results for the two patients in this study.
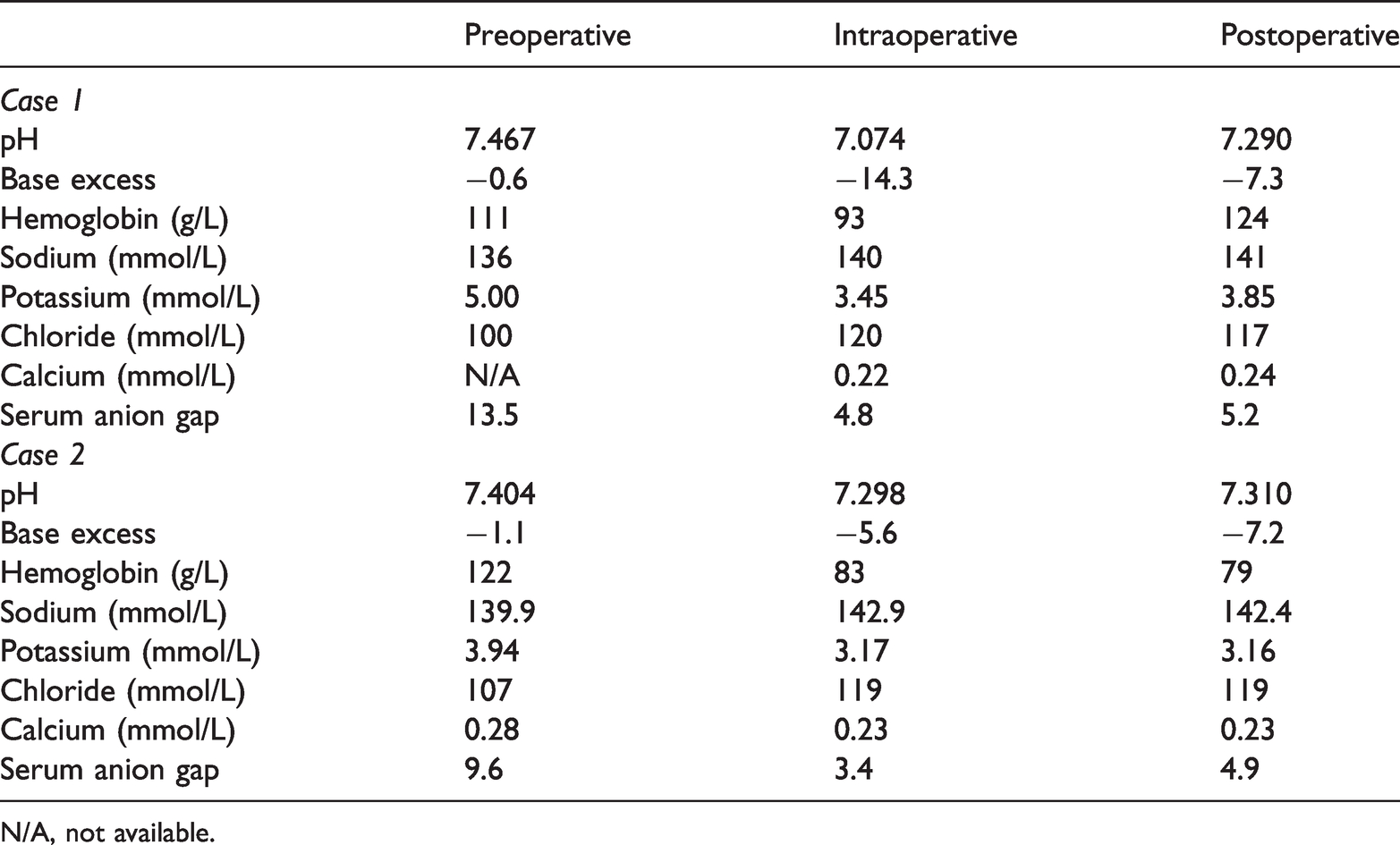
N/A, not available.
Case 2 involved an 80-year-old man with a history of hypertension, diabetes mellitus, and deep vein thrombosis. The preoperative estimated prostate weight was 186 g. General anesthesia was induced, and surgery was performed. Preoperative laboratory testing revealed the following: pH, 7.404; BE, −1.1; Hb, 122 g/L; Na, 139.9 mmol/L; and Cl, 107 mmol/L. Ephedrine and phenylephrine were administered intraoperatively because of a sudden decrease in blood pressure. Intraoperative laboratory test results 65 minutes after beginning surgery were as follows: pH, 7.298; BE, −5.6; Hb, 83 g/L; Na, 142.9 mmol/L; and Cl, 119 mmol/L. Capsular perforation was also observed. The estimated blood loss was 1000 mL, operation time was 95 minutes, resected prostate weight was 63 g, and irrigation fluid volume was 24 L. The patient was transferred to the postanesthesia care unit after surgery.
Discussion
We report two cases of hyperchloremic metabolic acidosis that occurred during bipolar TURP. TURP syndrome occurs in 1% to 8% of patients undergoing monopolar TURP, and is caused by absorption of hypoosmolar irrigation fluid. Dilutional hyponatremia, hypoosmolality, and cardiovascular compromise, which could be fatal, occurs in TURP syndrome. 1 During bipolar and laser TURP, the risk of TURP syndrome is eliminated owing to the use of normal saline as irrigation fluid. However, acute changes in BE, pH, and electrolytes, combined with hemodynamic instability, may occur.
Scheingraber et al. 2 reported that massive absorption of irrigation fluid causes clinically relevant metabolic acidosis, and that monitoring acid-base status is crucial during anesthesia for TURP. Although severe cardiovascular disturbances, hypervolemia, and electrolyte imbalance were not observed, pH and sodium and chloride concentrations decreased, and BE deteriorated in the patients in Scheingraber et al.’s report. The resected prostatic tissue and irrigation volume were lower than those observed in our cases.
Irrigation volume, time, and the preoperative and resected prostate weights directly influence the amount of fluid absorbed. 3 Moreover, the height of the irrigation bag above the prostatic sinuses has an effect on the absorption of irrigation fluid. 4 Finally, irrigation fluid absorption is highly affected by the prostatic anatomical barrier. 5 When manipulating close to the prostatic capsule, more fluid can be absorbed. If capsular perforation or large vessel injury is present, hemodynamic compromise can occur. Although the reported volume of absorbed fluid varies among studies, most studies have reported a volume of less than 2000 mL, which is considered dangerous, in TURP syndrome. 5
Patients with hemodilution caused by isotonic solutions have different symptoms and laboratory test results than those with TURP syndrome. Neurological symptoms are rare, and hemodynamic compromise caused by absorption of isotonic solution tends to occur in the latter part of the surgery, whereas TURP syndrome occurs within 15 to 20 minutes to 24 hours.1,5 Hyponatremia can be used as an indicator of fluid absorption only when using hypoosmolar irrigation solutions. Hyperchloremia and acidosis can be used as potential indicators of fluid absorption because high chloride concentrations are absorbed from the normal saline. 5
When risk factors are suspected during TURP, anesthesiologists must pay attention to serum electrolyte and acid-base status even when the procedure uses isotonic solution as the irrigation fluid. The risk factors are large irrigation volume, height of the irrigation solution bag exceeding 60 cm, long operation time, manipulation near the anatomical barrier, and extended tissue resection.2–5
Spinal anesthesia offers some advantages over general anesthesia for monopolar TURP. However, mortality, morbidity, and postoperative complications are not significantly different between spinal and general anesthesia groups in bipolar and laser TURP. Increased morbidity is more often associated with surgical and patient factors than the anesthesia type. 6 Furthermore, geriatric patients often receive medications for comorbidities, and the use of anticoagulants is common. In case 2, the patient was receiving anticoagulants owing to deep vein thrombosis. General anesthesia using laryngeal masks was chosen for our patients; neurological symptoms, actual volume of absorbed fluid, height of the irrigation bag, and serum osmolality were not monitored. 4
In conclusion, anesthesiologists must monitor acid-base and electrolyte status when rapid absorption of excessive isotonic solution is suspected, even during bipolar and laser TURP, which use normal saline as the irrigation fluid. The risk factors for rapid absorption are prolonged surgery, large irrigation volume, high irrigation solution bag, and large preoperative and resected prostate weights.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
This study was performed in accordance with the guidelines of the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Kyung Hee University Hospital (ethics approval number: 2020-11-043, approval date: 19 November 2020). The patients provided written informed consent for publication, and this case report was written in accordance with the CARE case report guidelines.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.