
Abstract
Objective
This study was performed to compare the effectiveness of routine Bakri balloon tamponade (BBT) and uterine gauze packing (UGP) during cesarean section in patients with placenta previa.
Methods
This study involved women with placenta previa who underwent cesarean section with either prophylactic BBT (n = 98) or UGP (n = 64) from January 2016 to December 2018. The clinical variables and pregnancy outcomes were compared between the two groups.
Results
The estimated intraoperative blood loss was significantly lower in the BBT than UGP group (667 ± 358 vs. 791 ± 360 ml, respectively). Additionally, the proportion of patients who required transfusion was significantly lower in the BBT than UGP group (9/98 vs. 17/64, respectively). The operative duration (97.8 ± 17.7 vs. 108.2 ± 16.9 minutes) and the length of stay (3.79 ± 0.89 vs. 4.12 ± 0.85 days) were significantly shorter in the BBT than UGP group.
Conclusions
In patients with placenta previa who undergo cesarean section, preventive application of BBT is superior to UGP for decreasing the intraoperative blood loss and transfusion rate. BBT is a more reliable technique to prevent and control postpartum hemorrhage.
Keywords
Introduction
Placenta previa, defined as complete or partial coverage of the internal os of the cervix by the placenta, complicates about 1 in 200 pregnancies at term, and its incidence is increasing each year because of increases in the cesarean section rate. 1 Patients with placenta previa are at high risk of postpartum hemorrhage, which can result in blood transfusion, hysterectomy, maternal intensive care admission, and maternal death. 2
Intraoperative methods to control profuse bleeding during cesarean section in patients with placenta previa include uterine packing, balloon tamponade, uterine compression sutures, arterial ligation, uterine artery embolization, and hysterectomy.
Some studies have shown that Bakri balloon tamponade (BBT) can control postpartum hemorrhage during cesarean section in patients with placenta previa.3,4 Uterine gauze packing (UGP) is a more traditional method of controlling hemorrhage associated with placenta previa. 5 To our knowledge, no study has compared these two methods in patients with placenta previa undergoing cesarean section.
Therefore, the present study was performed to compare the effectiveness of BBT and UGP during cesarean section in patients with placenta previa.
Materials and methods
This retrospective study involved patients with placenta previa who were treated with either BBT (Bakri balloon; Cook Women’s Health, Spencer, IN, USA) or UGP from January 2016 to December 2018 at the Department of Obstetrics and Gynecology in Guangzhou Women and Children’s Medical Center. The following clinical data were obtained from a review of the medical records: age, parity, body mass index, previous cesarean section, emergency cesarean section, placenta location, placenta accreta, gestational age, intraoperative estimated blood loss, postoperative estimated blood loss, preoperative and postoperative hemoglobin concentrations, need for transfusion, development of disseminated intravascular coagulation, intensive care unit admission, hemostatic measures, duration of the operation, and length of stay. The ethics committee at Guangzhou Women and Children’s Medical Center approved the study, and all participants provided written informed consent.
Prior to Bakri balloon insertion or UGP, all participants were given 40 IU of oxytocin in 500 mL of Ringer’s solution at a rate of 125 ml/h intravenously as well as ergometrine at 0.25 to 0.5 mg intramuscularly.
The choice of either prophylactic BBT or prophylactic UGP was based on the preference of the attending obstetrician after delivery of the placenta during cesarean section. The procedures were performed by one surgical team with different surgeons in our unit.
In the BBT group, the Bakri balloon was inserted into the lower uterine segment through the uterine incision by passing the balloon shaft through the cervix with an assistant pulling vaginally. The uterine incision was closed in two layers after confirming the position of the balloon. The balloon was initially inflated with 100 mL of warm saline, gauze was packed into the vagina to prevent movement of the balloon, and the balloon was filled with warm saline to a final amount of 350 to 500 mL according to the capacity of the uterus. A collection bag was used to collect the blood drainage. The balloon was removed 24 hours later.
The patients in the UGP group were treated as described in a previous study. 6 Briefly, a 3-m-long, 4-cm-wide gauze was soaked in povidone–iodine solution before packing. The uterine cavity was packed with the gauze through the uterine incision. The surgeon held the anterior lip of the cervix using a ring forceps, then inserted the sterile gauze into the uterus fundus with the ring forceps directed downward to the whole uterus cavity and the vagina. The gauze was thoroughly packed within the uterine cavity in a side-to-side manner to eliminate the dead space. The gauze was removed after 24 hours.
Hemostatic procedures were considered to have failed if additional surgical procedures were required, such as application of B-Lynch sutures, suturing of the placental bed, ligation of the internal iliac artery, uterine artery embolization, or hysterectomy.
Use of blood products such as packed red blood cells, fresh frozen plasma, cryoprecipitate, or platelets was initiated for patients with a hemoglobin concentration of <70 g/L or laboratory evidence of coagulopathy (e.g., platelet count of <50,000/mm3, fibrinogen concentration of <100–150 mg/dL, or prothrombin time or activated partial thromboplastin time of >1.5 times normal).
Statistical analyses of clinical data were performed using the IBM Statistical Package for the Social Sciences (IBM SPSS v.19; IBM Corp., Armonk, NY, USA). Dichotomous data were compared using the χ2 test and Fisher’s exact test, and continuous data were compared using the t test. A p value of <0.05 was considered statistically significant.
Results
We reviewed the medical records of 162 patients who were diagnosed with placenta previa and underwent cesarean section. Of the 162 patients, 98 underwent BBT and 64 underwent UGP. The demographic characteristics were compared between the two groups and are shown in Table 1.
Maternal characteristics of the study participants.

Data are presented as n (%) or mean ± standard deviation.
BMI, body mass index; CD, cesarean delivery.
The BBT and UGP groups did not differ significantly in maternal age, parity, body mass index, previous cesarean section, emergency cesarean section, placenta location, placenta accrete, or gestational age (Table 1).
Table 2 shows the operative and postoperative characteristics in the BBT and UGP groups. The mean estimated intraoperative blood loss was 667 mL in the BBT group and 791 mL in the UGP group (p = 0.033). The proportion of patients who required transfusion was significantly lower in the BBT than UGP group (p = 0.006). The duration of the operation (p = 0.023) and the length of stay (p = 0.020) were significantly shorter in the BBT than UGP group.
Operative and postoperative characteristics of the two groups.
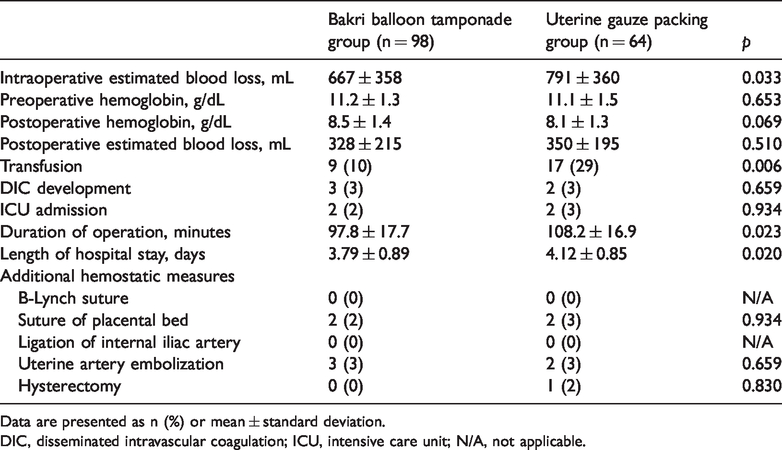
Data are presented as n (%) or mean ± standard deviation.
DIC, disseminated intravascular coagulation; ICU, intensive care unit; N/A, not applicable.
There were no significant differences in the preoperative hemoglobin concentration, postoperative estimated blood loss, postoperative hemoglobin concentration, diagnosis of disseminated intravascular coagulation, intensive care unit admission, or additional hemostatic measures between the BBT and UGP groups.
Discussion
Placenta previa is a leading cause of maternal morbidity and mortality due to intrapartum hemorrhage. Therefore, numerous methods have been proposed to control intrapartum bleeding and thus decrease postpartum hemorrhage and other adverse consequences. 7
In this retrospective study, we evaluated 162 women diagnosed with placenta previa who had undergone either prophylactic BBT or UGP during cesarean section. We found that routine use of BBT was more effective in decreasing intrapartum hemorrhage and the need for transfusion.
Intrapartum bleeding in patients with placenta previa may originate in part from the location of the blood vessel bed in the lower segment, where the myometrium is poorly contractile and does not adequately compress myometrial vessels to control blood loss. In theory, tamponade of the lower segment of the uterus using a Bakri balloon or gauze packing compresses the blood vessel bed to achieve hemostasis. The Bakri balloon was originally applied to manage hemorrhage due to placenta previa and is now widely used to control postpartum hemorrhage. Disadvantages of BBT include balloon damage, high cost, and limited effectiveness in a large uterine cavity.
UGP is an older method used to control bleeding. Previous studies have shown that both BBT and UGP are effective in the prevention and treatment of postpartum hemorrhage in patients with placenta previa.8–10 BBT is simpler and faster to complete than UGP. The longer application time required for UGP may explain why the intraoperative blood loss is higher for UGP than BBT. Infection and concealed hemorrhage are disadvantages of UGP. Soaking the gauze in a povidone–iodine solution is advised to reduce the chance of infection.
The limitations of our study include its retrospective nature, relatively low number of cases, and single-center data. Nevertheless, our study is first to compare the efficacy of BBT and UGP in prevention and control of intrapartum bleeding during cesarean section. Our findings suggest that clinical benefits can be obtained by routine performance of BBT.
In conclusion, prophylactic insertion of a Bakri balloon during cesarean section in patients with placenta previa was associated with lower intraoperative blood loss. Our study demonstrated that routine insertion of a Bakri balloon immediately after delivery of the placenta could be a useful method for controlling bleeding in patients with placenta previa.
Footnotes
Acknowledgements
We thank Prof. Abraham (Nick) Morse for the English language editing and proofreading. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.