
Abstract
Uterine artery embolization (UAE)-assisted induction of labor is an alternative method of managing pregnant women with complete placenta previa (CPP). Sepsis secondary to UAE, although rare, is a serious complication. We herein present a case of severe sepsis following UAE-assisted termination of a pregnancy at 27 gestational weeks in a woman with CPP. The woman developed a high-grade fever and elevated inflammatory indices following UAE. She did not recover until the infected tissue was removed by emergency cesarean section. This case suggests that the increasing use of UAE for termination of pregnancy in women with CPP requires awareness regarding the possibility of serious sepsis associated with this procedure.
Keywords
Introduction
Complete placenta previa (CPP), defined as complete coverage of the internal cervical os by the placenta, is a high-risk factor for obstetric hemorrhage. If the fetus is likely to survive, cesarean section or prophylactic uterine artery embolization (UAE) immediately followed by cesarean section is the first-choice technique for termination of pregnancy with CPP. In cases involving fetal demise or major malformation, which are not uncommon in pregnancy with CPP, cesarean section cannot decrease the intraoperative hemorrhage.1,2 Moreover, delivery by cesarean section increases the risk of placental abnormalities, such as placenta accreta and cesarean scar pregnancy, in subsequent pregnancies. Termination of pregnancy in such conditions contributes to therapeutic dilemmas for the treating obstetricians. UAE blocks the main placental blood supply, thereby reducing the incidence of peripartum hemorrhage and avoiding cesarean section in women at risk. In two separate case series, Peng and Zhang 3 and Huang et al. 4 recommended UAE-assisted induction of labor as a safe method of managing women with CPP because it was associated with a lower incidence of postpartum hemorrhage and fewer complications (such as gluteal muscle pain) without any increase in the duration of labor. Our experience with the successful use of UAE in 16 women supports this recommendation. However, increased application of UAE-assisted induction of labor should be accompanied by an awareness of the serious complications associated with this procedure. We herein present a case of serious sepsis in a woman with CPP following UAE-assisted induction of labor that required emergency cesarean section.
Case report
The patient was a 31-year-old woman who was admitted at 27 weeks of gestation for abnormal fetal development identified on a routine prenatal checkup. Ultrasonography revealed anencephaly with a biparietal diameter of 5.4 cm and femur length of 2.8 cm. The fetal position was right sacrum anterior. The placenta was mostly located on the anterior uterine wall and completely covered the cervical os. Placenta accreta was ruled out on both ultrasonography and magnetic resonance imaging (Figure 1). At admission, her temperature was 37.1℃, and laboratory tests revealed a white blood cell (WBC) count of 13.0 × 109 cells/L with 81.4% neutrophils and a C-reactive protein (CRP) level of 1.8 mg/L. Her coagulation profile and liver and renal function tests results were normal.
Imaging findings. (a) Diffusion-weighted imaging and (b) T2-weighted magnetic resonance imaging scans showed that the cervical os (white arrow) was completely covered by the placenta (black arrow). Axial scan.
On the second day following admission, 100 mg of ethacridine lactate was injected into the amniotic cavity to induce labor. Two hours later, UAE was performed by the Seldinger technique (Figure 2). Four hours following UAE, the patient was found to have a temperature of 41.1℃. Laboratory tests revealed a WBC count of 3.9 × 109 cells/L with 69.2% neutrophils and a CRP level of 28.2 mg/L. She was administered intravenous moxifloxacin at 0.4 g once daily. Her inflammatory marker levels were higher when tested 10 hours following UAE (WBC count, 21.5 × 109 cells/L with 98.1% neutrophils; CRP, 30.8 mg/L; procalcitonin, 48.34 ng/mL; activated partial thromboplastin time, 67.2 s; prothrombin time, 19.8 s; alanine transaminase, 142 U/L; and aspartate transaminase, 251 U/L). Her blood pressure decreased to 75/40 mmHg. She exhibited no evidence of uterine contraction or cervix dilatation. Septic shock was suspected, and an emergency cesarean section was performed to remove the infected tissues. The weight of the fetus was 400 g. Intravenous moxifloxacin (0.4 g once daily) and vancomycin (0.5 g twice daily) were administered for 1 week postoperatively. Both uterine cavity culture and blood cultures revealed Serratia marcescens sensitive to moxifloxacin. The patient was discharged on postoperative day 9, after her temperature and inflammatory markers had normalized.
Uterine artery embolization was performed under local anesthesia along with two experienced interventional radiologists. The uterine artery (black arrow) was selectively catheterized with a 5-Fr Yashiro catheter (Terumo Corporation, Tokyo, Japan). Both uterine arteries were blocked with an absorbable gelatin sponge (Gelfoam; Pfizer, New York, NY, USA) measuring 1400 to 2000 µm at a total dose of 90 to 150 mg. L: left side. (a) Before embolization. (b) After embolization.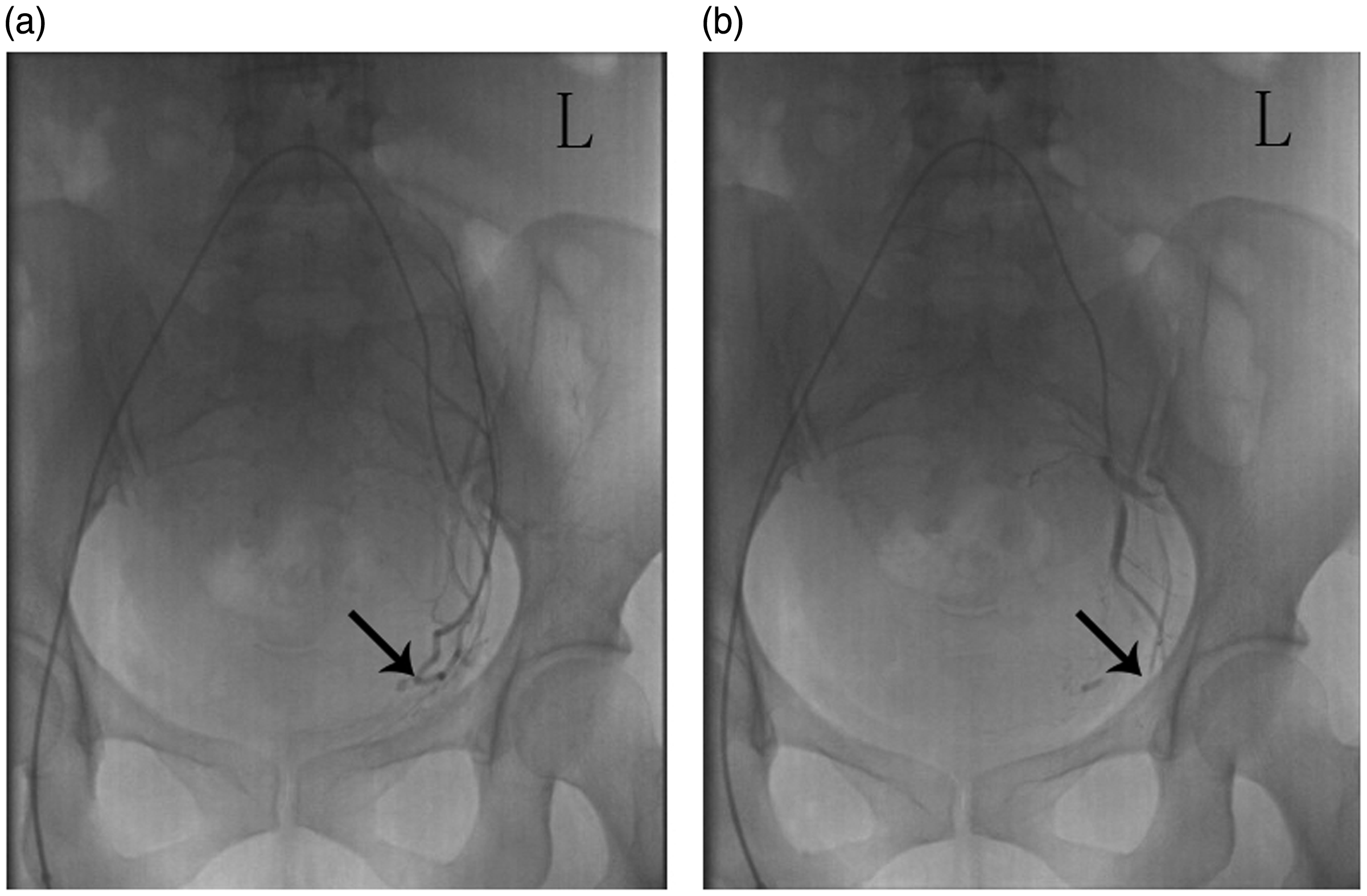
The present study was approved by the ethics committee of Zhejiang University, and the termination of the pregnancy because of anencephaly was performed according to the Chinese law. The patient provided written informed consent for publication of her information and images.
Discussion
UAE is a safe technique for the control of certain hemorrhagic conditions in gynecology and obstetrics, such as postpartum hemorrhage, cesarean scar pregnancy, and arteriovenous malformations, and it is associated with a low complication rate. 5 The uteroplacental blood supply is an important factor contributing to intrapartum and postpartum hemorrhage. 6 CPP often leads to massive hemorrhage requiring urgent cesarean section and sometimes even hysterectomy. UAE-assisted induction of labor was recently described as a feasible method for termination of pregnancy in women with CPP and was reported to have a high rate of successful vaginal delivery.3,4 The experience at our center is similar; among 20 women treated with UAE, 16 women (80%) had a successful vaginal delivery (unpublished data).
UAE-associated infective complications result in a significantly high readmission rate and may occur despite the use of periprocedural prophylactic antibiotics. Although sepsis after UAE is very rare, it is potentially fatal. Sepsis has an overall incidence of 0.002% to 0.01% of all deliveries and is a leading cause of maternal mortality in the United States. 7 The patient in the present case had no evidence of infection before induction of labor, but uterine cavity and blood cultures isolated S. marcescens. The sepsis broke out shortly following UAE, and broad-spectrum antibiotics were ineffective until the infected tissues were removed following cesarean section. Although the underlying mechanism for sepsis in such cases is uncertain, the following factors may be involved: Downregulation of cell-mediated immunity during pregnancy may predispose women to certain infections, 8 a reduced blood supply following UAE may prevent antibiotic access to the uterus while uterine ischemia encourages bacterial proliferation, 9 and the closed uterine cavity secondary to the presence of CPP prevents drainage of inflammatory material or septic foci. 7 The involvement of these factors is supported by the prompt clinical improvement after emergency cesarean section and intravenous antibiotics.
In conclusion, UAE effectively reduces the uteroplacental blood supply and the risk of hemorrhage in women at risk. However, UAE renders the uterus ischemic, which in combination with the sealed status of the uterus may encourage bacterial growth and result in sepsis. In these women, severe sepsis may be caused by multiple factors, especially uterine infections similar to chorioamnionitis. Our study suggests the need for obstetricians to be aware of the potential for serious sepsis following UAE-assisted termination of pregnancy in women with CPP.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.