
Abstract
Objective
Coronary artery disease (CAD) is the leading cause of morbidity and mortality in the world. The proprotein convertase subtilisin/kexin type 9 (PCSK9) E670G polymorphism has been reported to be associated with variability in levels of low density lipoprotein cholesterol, a risk factor for CAD. However, the relationship between PCSK9 E670G and CAD is still not fully elucidated.
Methods
A total of 225 patients and 189 control subjects were recruited in this study. DNA was extracted from peripheral blood samples and was genotyped by mass array method. In addition, we also conducted a meta-analysis of case-control studies to elucidate the relationship of CAD and polymorphism.
Results
The GG genotype of PCSK9 E670G was associated with a higher risk of CAD [odds ratio (OR) 2.994, 95% confidence interval (CI): 1.174–7.631], even adjusting for risk factors (OR 2.794, 95% CI: 1.215–7.460). Logistic regression analysis showed that the dominant genetic model increased the CAD risk (OR 2.313, 95% CI: 1.070–6.983) after adjusting the confounding factors. Meta-analysis results of 13 studies revealed that PCSK9 E670G polymorphism was correlated with CAD risk under different genetic models.
Conclusion
Our results demonstrated that PCSK9 E670G genotype was associated with a high risk of CAD.
Keywords
Introduction
Coronary artery disease (CAD) is the leading cause of morbidity and mortality in world. Nearly 56 million deaths worldwide were attributed to CAD from 2000 to 2012. 1 A number of external risk factors such as smoking, drinking, sedentary lifestyle, and poor dietary habits are correlated with CAD, a multifactorial disease. 2 Nevertheless, the mechanism of CAD has not been fully elucidated. In the past few decades, genetic polymorphisms have been identified that play a vital role in CAD progression. Based on family and twin studies, it has been estimated that 40% to 60% of susceptibility to CAD can be attributed to genetic factors. 3
Proprotein convertase subtilisin-like kexin type 9 (PCSK9) is a subtilisin serine protease located on chromosome 1p32.3 and is 22 kb long. 4 It plays an important role in modulating the plasma levels of low-density lipoprotein cholesterol (LDL-C) by binding to the LDL receptor (LDLR) and promoting its degradation through a post-transcriptional mechanism.5,6 Overexpression of PCSK9 can cause a reduction in LDLR level and LDL-C accumulates in blood, leading to hypercholesterolemia and atherosclerosis.7,8
PCSK9 is a highly polymorphic gene, and its polymorphisms and mutations are associated with variability in LDL-C levels and CAD. A common single nucleotide polymorphism (SNP) rs505151 (E670G), which is located in the cysteine-rich C-terminal domain in exon 12, results in an amino acid substitution from glutamate to glycine and is potentially associated with the altered enzyme activity of PCSK9.4,9,10 Ding and Kullo 11 noted that the E670G polymorphism was associated with elevated LDL-C levels in both African Americans and European Americans. Cai et al. 12 reported that PCSK9 E670G polymorphism was associated with CAD risk and lipid levels in a meta-analysis. However, the relationship between the genetic polymorphism E670G and CAD remains controversial. Polisecki et al. 13 revealed no relationship between E670G with CAD. Meanwhile, Hsu et al. 14 reported a negative relationship in a Chinese Taiwan population. Thus, to draw a more precise association of the E670G polymorphism of PCSK9 and the risk of CAD, we sought to assess the effect of E670G on CAD and determine a possible association in the Chinese population in a case-control study.
Materials and methods
From June 2018 to January 2019, patients with CAD and controls were consecutively enrolled from the outpatient and inpatient departments of Fujian Provincial Geriatric Hospital. Written informed consent was received from all study participants. Patients were defined as having CAD when presenting a stenosis ≥50% in at least one major coronary artery when examined by coronary angiography. The control group included individuals who received regular health examinations and had no history, signs, or symptoms of cardiovascular disease. Patients with severe liver, renal, or cardiac impairment or any malignancy were excluded from the study. The study was approved by the Ethics Committee of Fujian Provincial Geriatric Hospital and was performed in accordance with the Declaration of Helsinki.
Genotyping
Peripheral venous blood was collected by a phlebotomist from each participant into EDTA anticoagulant tubes. All samples were stored at −80°C until use. DNA was extracted from blood using a commercial kit (Qiagen, Hilden, Germany) according to the manufacturer’s protocol. Genetic polymorphism was identified on the Agena MassARRAY system (Agena/Sequenom Inc., San Diego, CA, USA) according to the manufacturer’s user guide.
Meta-analysis
The PubMed, Embase, China National Knowledge Infrastructure (CNKI), and WanFang Data electronic databases were searched for studies to include in the meta-analysis. Medical subject headings (MeSH) and title/abstract were used to screen all eligible studies that focused mainly on the relationship of the E670G polymorphism and CAD. The references and retrieved articles were hand searched simultaneously. Eligible studies had to meet the following criteria: (1) studies that had been conducted in human subjects; and (2) that supplied the number of individual genotypes in cases and controls; accordingly, the exclusion criteria were as follows: (1) studies without detailed genotype data; and (2) reports with overlapping data.
Statistical analysis
All statistical analyses were performed by using SPSS Statistics for Windows (version 17.0, SPSS Inc., Chicago, IL, USA). Student’s t-test (for continuous variables) or Chi-squared tests (for categorical variables) were used to evaluate differences in demographic variables and genotype frequencies between groups. Logistic regression analysis was used to evaluate the associations between the genotype of the E670G polymorphism and the risk of CAD by comparing the odds ratios (OR) and 95% confidence intervals (CI). The adjusted ORs [including sex, age, body mass index (BMI), and smoking and drinking habits] and their 95% CI were also calculated.
For meta-analysis, heterogeneity was evaluated by the I2 statistic. If I2 < 50%, the fixed effect model (Mantel–Haenszel method) was used; otherwise, the random-effect model (DerSimonian–Laird method) was used to calculate the pooled ORs. Pooled ORs and 95% CIs were calculated using the following genetic models: (1) allele, (2) recessive, (3) homozygous, (4) heterozygous, and (5) dominant. The significance of pooled ORs was assessed by Z-test, where p < 0.05 indicated statistical significance. Publication bias was assessed by Begg’s funnel plots.
Results
Characteristics of the study participants
A total of 225 patients (104 women) and 189 controls (76 women) were recruited for this hospital-based case-control study. All patients were Chinese with confirmed coronary angiography for diagnosis of CAD. There were significant differences in BMI and triglycerides between the CAD patients and individuals in the control group (p < 0.05). In addition, CAD patients had higher frequencies of smoking and drinking habits, which might be an important risk factor for CAD. No deviation from the Hardy–Weinberg equilibrium (HWE) was observed (HWE = 0.082) in the control group. The demographic and clinical characteristics of the participants are shown in Table 1.
Characteristic of the participants.

Significant associations are marked in bold.
BMI, body mass index; TG, triglyceride; TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Genetics association analysis
The genotype distribution of the PCSK9 gene polymorphism in patients and controls is shown in Table 2. No significant differences were observed between patients and controls in the distribution of AA, AG, and GG genotypes (p = 0.057). In contrast, there was a significant difference in the allelic model of genotype A and genotype G (p = 0.033).
The genotype of PCSK9 E670G polymorphism in CAD and control group.

Significant associations are marked in bold.
PCSK9, proprotein convertase subtilisin/kexin type 9; CAD, coronary artery disorder.
To further elucidate the relationship of PCSK9 E670G with CAD, we performed a logistic regression analysis between patients and controls. We found that the AG and GG alleles were significantly correlated with CAD morbidity (OR = 2.697, 95% CI: 1.008–7.213, p = 0.043; OR =2.994, 95% CI: 1.174–7.631, p = 0.017). After adjusting for age, sex, BMI, and smoking and drinking habits, there was still a significant association of the GG genotype (OR = 2.794, 95% CI: 1.215–7.460, p = 0.019) with CAD, whereas no significant difference was observed for the AG genotype (OR = 2.574, 95% CI: 0.981–7.196, p = 0.057). We also found a significant association under the dominant model (OR = 2.911, 95% CI: 1.151–7.366, p =0.019), even after adjusting for the risk factors (OR = 2.313, 95% CI: 1.07–6.983, p = 0.030). Nevertheless, no significant association of the polymorphism with CAD was observed under the recessive genetic model (OR = 1.323, 95% CI: 0.874–2.003, p = 0.185) (Table 3).
The logistic regression analysis of PCSK9 E670G genotype with the CAD risk.

*Adjusting for sex, age, body mass index, smoking, drinking. Significant associations are marked in bold.
PCSK9, proprotein convertase subtilisin/kexin type 9; CAD, coronary artery disorder.
Meta-analysis results
To further explore the relationship of PCSK9 E670G polymorphism with CAD, we conducted a meta-analysis. Thirteen articles (including our results) were enrolled in the analysis (Figure 1). The study characteristics included in the meta-analysis are listed in Table 4 and Table 5. Heterogeneity was identified by I2 statistic in genetic models and the dominant and allelic models were shown to have substantial heterogeneity (I2 = 85.7%, I2 = 85%); thus, the random effect model was used. The fixed model was used in the homozygote, heterozygote, and recessive models. The results revealed a significant association between the PCSK9 E670G polymorphism and CAD under the dominant model (OR =1.67, 95% CI: 1.13 − 2.47, p = 0.011), recessive model (OR = 1.99, 95% CI: 1.37 −2.89, p = 0.001), homozygote model (OR = 2.36, 95% CI: 1.57 − 3.55, p =0.001), heterozygote model (OR = 1.57, 95% CI: 1.06 − 2.32, p = 0.024), and allelic model (OR = 1.65, 95% CI: 1.18 − 2.3, p = 0.003) (Figure 2).

Flow chart summarizing study identification and selection.
Characteristics of the studies included in this meta-analysis.

BMI, body mass index; TG, triglyceride; TC, total cholesterol; NA, not available.
Summary of genotype frequencies of PCSK9 E670G among CAD patients and controls.
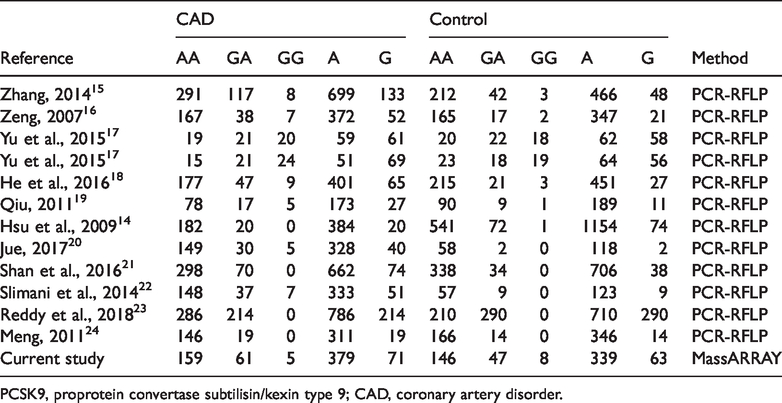
PCSK9, proprotein convertase subtilisin/kexin type 9; CAD, coronary artery disorder.

Forest plots of the PCSK9 E670G polymorphism under different genetic models: (a) dominant model; (b) heterozygote model; (c) homozygote model; (d) recessive model. PCSK9, proprotein convertase subtilisin/kexin type 9.
Publication bias was evaluated by using Begg’s test and no significant publication bias was found (p > 0.05; Figure 3). In addition, we conducted a sensitivity analysis to assess the influence of each individual study on the pooled OR. The results revealed that no single study influenced the quality of the pooled ORs in the sensitivity analyses (Figure 4).

Begg’s funnel plot for publication bias analysis (dominant model).

Sensitivity analysis result of the association between PCSK9 E670G polymorphism and CAD susceptibility under the dominant model. PCSK9, proprotein convertase subtilisin/kexin type 9; CAD, coronary artery disorder.
Discussion
CAD is a primary global public health challenge that is associated with severe health problems and economic burdens worldwide.1,25 However, as a multifactorial disorder, CAD is influenced by the interaction of genetic and physical condition. 26 Dyslipidemia has a multifactorial origin, including environmental factors such as demographics, diet, alcohol consumption, cigarette smoking, and obesity. In our study, we enrolled CAD patients with high levels of total cholesterol and triglycerides and high BMI (Table 1). However, we did not assess dietary factors (e.g., salt intake), which may partly influence the results.
PCSK9 has been shown to play an important role in modulating plasma levels of LDL-C.27,28 It can effectively bind to the LDLR on the surface of hepatocytes, targeting the LDLR for lysosomal degradation and preventing recycling to the hepatocyte surface, mediating approximately 70% of LDL-C clearance. Thus, identifying and understanding the functional importance of genetic alterations is crucial in our understanding of CAD. Numerous studies in different ethnic groups have been performed to investigate the relationship of PCSK9 E670G variants with the incidence of cardiovascular risk. Hsu et al. reported that the frequency of the G allele is rare in whites but more common in blacks. The PCSK9 E670G carrier was identified less frequently in patients with CAD than in controls in Chinese Taiwanese individuals. 14 However, the findings to date are inconsistent. In our study, we investigated the PCSK9 E670G polymorphism in 225 hospital-based patients with CAD; we found that this polymorphism was significantly correlated with the development of CAD, especially in people with the G allelic and dominant genetic model.
Although our case-control study showed positive results for the E670G polymorphism with CAD, we did not find any correlation in the heterozygote and recessive models. In contrast, our meta-analysis of 13 studies showed that the homozygote, heterozygote, recessive, dominant, or allelic models were risk factors for CAD. This may be attributed to the small sample size, different baseline characteristics, and different detection methods. Most of the enrolled studies used PCR-restriction fragment length polymorphisms (RFLP) to examine the SNP genotype, whereas our study used MassARRAY, which was more accurate. In addition, the patients and control participants in our study were much older than participants in the other enrolled studies. We believe these factors may explain the difference between our study and the results of the meta-analysis. These data need to be replicated in a larger cohort of patients, and functional studies are needed to investigate whether and how the PCSK9 E670G polymorphism is involved in the pathogenesis of CAD.
The E670G polymorphism was found to be associated with cardiovascular risk among the general Caucasian population. However, our meta-analyses also showed that the polymorphism was significantly associated with CAD in the Asian population, especially in a Chinese population. The present meta-analysis revealed for the first time that this SNP was correlated with CAD under five genetic models, although it remains to be determined whether this relationship is causal or a concomitant phenomenon. Given the discrepancies in the results of our case-control results, more studies are required to further verify the results.
Although the results of our study may help in identifying patients at risk of CAD, several limitations should be considered. First, the smaller sample size made it difficult to achieve statistical significance under some genetic models. In addition, all participants in our study were recruited from hospital, which might result in potential selection bias. Second, some potential confounding factors might not be included in the present study, which may result in an overestimation or underestimation of the effect of gene polymorphism. Furthermore, the meta-analysis only enrolled patients in the Asian population; the lack of varied ethnicity data may cause publication bias. In future studies, different ethnic groups should be included.
In conclusion, our results revealed that the E670G polymorphism of the PCSK9 gene is mainly associated with an increased risk of CAD. This result was partly in accordance with results of our meta-analysis. However, our results represent only a preliminary conclusion, and a larger cohort study is necessary to investigate whether and how the polymorphism might be involved in the pathogenesis of CAD.