
Abstract
Objective
Coronary artery disease (CAD) is the principal cause of mortality and morbidity worldwide. Studies have provided controversial results regarding whether variations in the proprotein convertase subtilisin/kexin type 9 gene (PCSK9) are risk factors for CAD. In this study, we evaluated the risk factors associated with PSCK9 genotypes and CAD in the Taiwanese population.
Methods
A total of 501 patients diagnosed with CAD by angiography and 334 CAD-free controls were recruited. Two single nucleotide polymorphisms of PSCK9 (rs505151 and rs529787) were genotyped.
Results
The prevalence of a positive family history for CAD was significantly higher in individuals carrying the AG + GG genotype of the PSCK9 rs505151 polymorphism. Among CAD patients with a positive family history, the prevalence of diabetes mellitus was significantly higher in those carrying the AG + GG genotype of the PSCK9 rs505151 polymorphism (73.3%) than in those carrying the AA genotype (39.2%).
Conclusion
In CAD patients, the AG genotype of PSCK9 rs505151 is associated with diabetes and a positive family history of CAD.
Keywords
Introduction
Coronary artery disease (CAD) is the principal cause of morbidity and mortality disability worldwide, and the number of deaths resulting from CAD have been predicted to increase rapidly until at least 2030. 1 CAD is a multifactorial disease that results from interactions between genetic and environmental risk factors. Genetic factors account for about 40%–60% of CAD cases, 2 and several genetic defects responsible for rare Mendelian forms of severe hypercholesteremia have been identified.
The proprotein convertase subtilisin/kexin type 9 gene (PCSK9) was the third to be associated with autosomal dominant hypercholesteremia. 3 PCSK9 is a circulating protein that is synthesized and secreted predominantly by hepatocytes. It plays an essential role in low-density lipoprotein (LDL) cholesterol homeostasis by mediating LDL receptor breakdown through a post-transcriptional mechanism, and was found to be a key risk factor for CAD.4–7
PCSK9 consists of 12 exons that encode a 692 amino acid glycoprotein. Since its recognition, accumulating evidence has proposed that PCSK9 variations are associated with the development of CAD and cerebrovascular events in different populations.8–12 However, studies have provided controversial results regarding whether PCSK9 variations are risk factors for CAD. Therefore, in this study, we evaluated whether PSCK9 single nucleotide polymorphisms (SNPs) are risk factors for CAD in the Taiwanese population.
Methods
Study participants
CAD patients were recruited from a cardiovascular clinic in Chung Shan Medical University Hospital (Taichung, Taiwan) and were diagnosed through angiography. Diagnostic criteria were more than 50% stenosis over any segment of the coronary artery as detected by coronary angiography. Individuals from the control group without CAD were recruited from the same hospital as the CAD group. They also underwent coronary angiography, but lumen stenosis was less than 50% lumen narrowing on one or more major epicardial coronary artery segments. Patients who had inflammatory disease, valvular heart disease, or cancer were excluded.
During the recruitment phase, all patients self-reported their age, sex, family history, clinical manifestation, and medical history, which were verified during the clinic visit. Clinical characteristics included: (1) personal history of smoking, hypertension, diabetes, hyperlipidemia, stroke, atrial fibrillation, and congestive heart failure; (2) medical history prior to admission, which included the CAD risk score, cardiac enzyme markers (serum cardiac troponin I levels), height, weight, and blood lipid profile; and (3) family history of cerebral infarction, myocardial infarction, and coronary heart disease. All participants provided written informed consent at each examination, and all study protocols were approved by Institutional Review Board of Chung Shan Medical University Hospital.
SNP selection and genotyping
DNA was extracted from EDTA-anticoagulated venous blood collected from CAD patients and controls using the QIAamp DNA Blood Mini Kit (Qiagen, Valencia, CA, USA) according to the manufacturer’s instructions. The SNPs investigated in this study were rs529787 and rs505151. They were selected based on previous reports supporting their association with PCSK9 expression and atherosclerosis. rs529787 was previously found to be associated with cerebral ischemic stroke in the Chinese population, 13 and rs505151 was associated with the risk of CAD. 14 Genotypes of PCSK9 rs505151 and rs529787 were determined by the ABI StepOne Real-Time PCR System (Applied Biosystems, Foster City, CA, USA), and analyzed using SDS version 3.0 software (Applied Biosystems, Foster City, CA, USA), as described previously.15,16
Statistical analysis
All continuous variables (age, body mass index, and body weight) are presented as mean ± standard deviation (SD). Differences between the CAD and control group were analyzed using an independent sample t test. Differences in the frequencies of sex, hypertension, diabetes mellitus, smoking, and genotypes were analyzed using the chi-squared test or Fisher’s exact test, as appropriate. A P value of less than 0.05 was considered to indicate statistical significance. Data were analyzed using SPSS statistical software (version 11.0; SPSS Inc., Chicago, IL, USA).
Results
A total of 501 CAD patients and 334 controls were recruited, and their clinical, demographic, and biochemical characteristics are shown in Table 1. Significantly higher proportions of smokers and men were seen in the CAD group compared with the control group (P < 0.05). Moreover, patients in the CAD group had significantly higher incidences of diabetes, hypertension, and congestive heart failure, and significantly elevated troponin I levels than controls (P < 0.05).
Demographics and clinical features of subjects in non-CAD and CAD groups (n = 835).
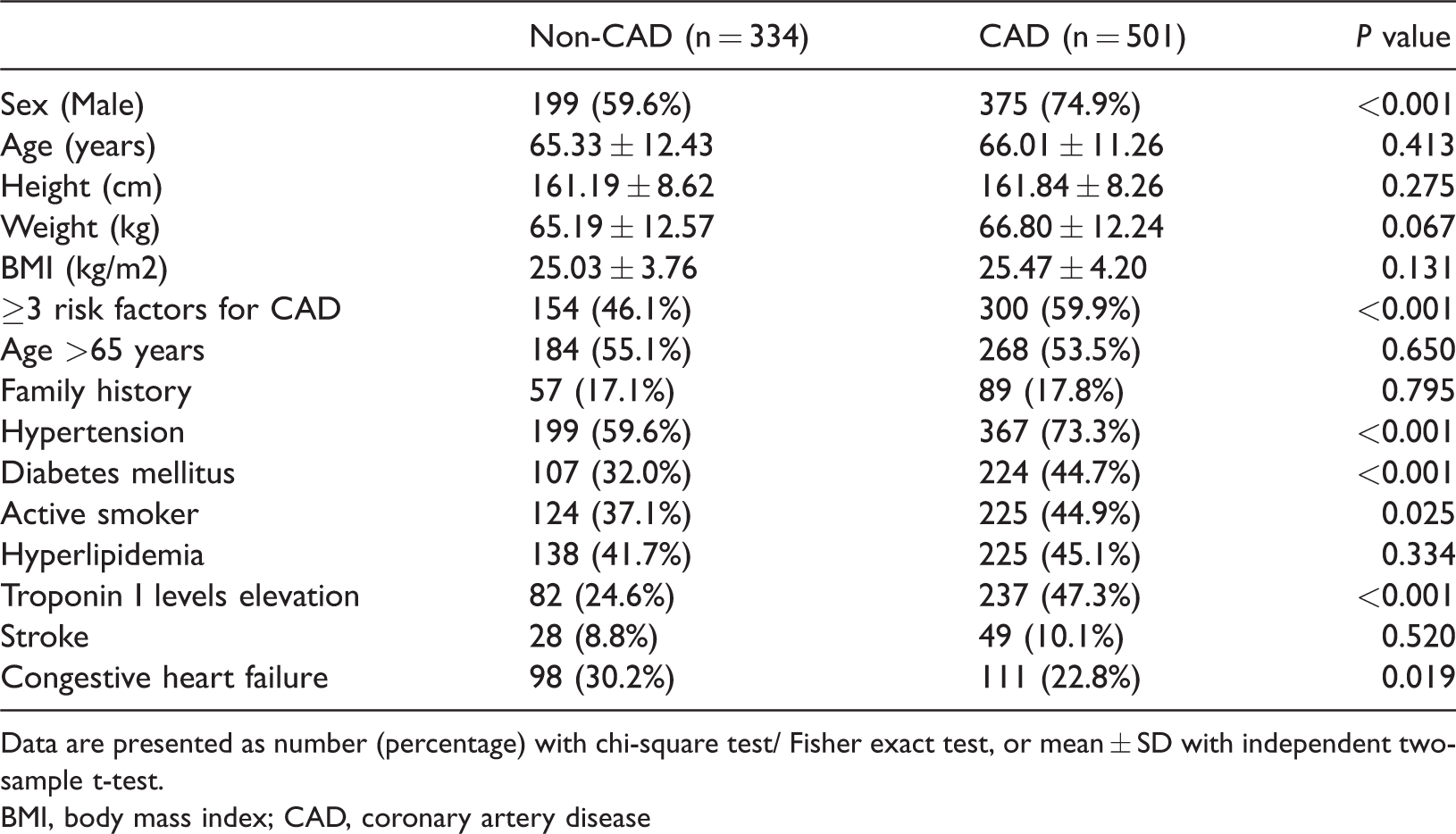
Data are presented as number (percentage) with chi-square test/ Fisher exact test, or mean ± SD with independent two-sample t-test.
BMI, body mass index; CAD, coronary artery disease
Genotype frequencies of PCSK9 SNPs are shown in Table 2. For SNP rs505151, the frequencies of AA, AG, and GG genotypes were 91%, 9%, and 0% in the control group, respectively. Corresponding frequencies were 90.4%, 9.6%, and 0%, respectively, in the CAD group. No significant differences were observed in the frequencies of genotypes and alleles between the two groups. For SNP rs529787, the CC genotype was the predominant genotype (100%) in both groups. Table 3 compares demographics and clinical characteristics between CAD patients with the AA genotype and those with the AG + GG genotype of SNP rs505151. Patients with a positive family history of CAD had a significantly higher odds ratio (OR) of carrying the AG + GG genotype (OR = 2.584, P < 0.05) than those without a family history. No significant differences were observed in other clinical characteristics.
Association of CAD and non-CAD patients with genotypic frequencies of PCSK9.

CAD, coronary artery disease; OR, odds ratio; CI, confidence interval
Comparison of demographics and clinical features between two genotypes of PCSK9 rs505151 for the CAD patient group.

Odds ratio (OR) with their 95% confidence intervals were estimated by logistic regression
We also examined the demographic and clinical characteristics of CAD patients with a positive family history. Among CAD patients with a positive family history, the prevalence of diabetes mellitus was significantly higher in those carrying the AG + GG genotype (73.3%) than in those carrying the AA genotype (39.2%, P = 0.015), with a higher OR of 4.881 (P < 0.05) as shown in Table 4.
Comparison of demographics and clinical features between two genotypes of PCSK9 rs505151 for CAD patients with a family history of CAD.

Odds ratio (OR) with their 95% confidence intervals were estimated by logistic regression
Discussion
In this study, we found a predominant prevalence of the AA genotype of PCSK9 rs505151, followed by the AG genotype in the Taiwanese population. For PCSK9 rs529787, CC was the major genotype. However, no significant difference was observed in genotype frequencies of the polymorphisms among patients with CAD. In the CAD group, the prevalence of a positive family history of cardiovascular events was significantly higher in those carrying the AG genotype of the rs505151 polymorphism. Furthermore, those carrying the AG genotype also had a higher risk of diabetes.
The frequency of PCSK9 rs505151 varies significantly among different races and ethnicities. For example, the rs505151 (E670G) G allele is rare in whites (3.6%–7.4%) and Hispanics (4.2%) but is present in approximately 24.8%–26% of blacks.9,11,17 In the present study, the frequencies of AA and AG genotypes of rs505151 were approximately 90% and 9%, respectively, and that of the CC genotype of PCSK9 rs529787 was approximately 100%. This result is consistent with that of Aung et al., which reported a similar genotype frequency (AA: 91% and AG: 8.36%) in the Chinese Han population. 18
A meta-analysis 14 previously indicated that the E670G polymorphism in PCSK9 might be correlated with the risk of CAD. Although the risk of CAD was higher in all models (allele, dominant, recessive, homozygous, and heterozygous models), the 95% confidence interval of the OR varied from 0.04–50.44. Heterogeneity might exist because of diversity in study design, ethnicity, sample sizes, genotyping methods, and risk profiles among studies. Contrary to previous reports, a study conducted in Taiwan indicated that the PCSK9 rs505151 polymorphism is not a risk variant for CAD in ethnic Chinese. 19 Another study detected an association between PCSK9 polymorphisms and serum lipid levels in the Chinese Han population; however, the risk of CAD was not determined. 18 These findings seem to be in accordance with our results, suggesting that PCSK9 rs505151 is not associated with CAD in ethnic Taiwanese.
Previous studies have also shown that the E670G variant is associated with increased plasma total cholesterol.9,20 In the present study, this finding was not confirmed in patients with CAD or controls (who have a high risk of CAD). Similar to these results, a previous study found that E670G was not associated with increased plasma lipid levels in the Taiwanese population, and another study found that the prevalence of three major risk factors was not higher in older Taiwanese patients with pre-existing vascular disease.19,21
Because of this discrepancy, we analyzed other risk factors associated with CAD in the present study. We found that patients carrying the AG genotype of the rs505151 polymorphism had a higher prevalence of diabetes and a positive family history of CAD. In a study conducted in Korea, pathogenic mutations in PCSK9 and genes encoding the low density lipoprotein receptor and apolipoprotein B were found in 32% of patients with clinically diagnosed familial hypercholesteremia. 22 However, mutation positivity was not a predictor of CAD, and instead hypertension, congestive heart failure, and high-density lipoprotein cholesterol were identified as independent predictors of CAD. As indicated by our results, we failed to correlate PCSK9 variation with CAD. However, we detected a higher risk of CAD in patients carrying the AG genotype of PCSK9 rs505151. Future work should evaluate whether carrying these variants increases the risk of CAD.
This was a cross-sectional study, and correlations could only be identified. Therefore, additional cohort studies should conduct a follow-up of our study population patients. Another limitation of this study was the lack of complete plasma lipid panel parameters. The association between PCSK9 polymorphisms and lipid levels is worthy of further investigation, which will be included in our future work.
In conclusion, our results indicated that the frequencies of the AA genotype in CAD and control groups were both approximately 90%, representing the major genotype of the PCSK9 rs505151 polymorphism in the Taiwanese population. The rare AG genotype of PCSK9 rs505151, associated with diabetes and a positive family history of CAD, was approximately 9%.
Footnotes
Acknowledgement
This work was supported by grants from the Chung Shan Medical University Hospital (CSH-2015-C-006).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.