
Abstract
Objective
To investigate the risk factors of postoperative low back pain (LBP) following posterior lumbar interbody fusion (PLIF) surgery for low-grade isthmic spondylolisthesis (IS).
Methods
This retrospective study enrolled patients with IS that underwent PLIF between January 2011 and January 2016. Demographic, clinical, surgical and radiological characteristics were analysed to determine associations between these characteristics and LBP as measured using a visual analogue scale (VAS) pain score.
Results
A total of 192 patients were enrolled in the study. The mean VAS pain score of LBP decreased significantly after surgery. The mean preoperative VAS pain score was significantly greater in patients with symptoms of ≤3 years duration compared with those with symptoms lasting >3 years. The postoperative VAS pain score was significantly lower in patients with grade 1 slippage compared with those with grade 2 slippage. There was a significant correlation between preoperative to postoperative change of VAS pain score and postoperative disc height (r = 0.99).
Conclusion
PLIF significantly improved LBP in patients with low-grade IS, although patients still reported some postoperative LBP. The grade of slippage was a risk factor for postoperative LBP. Restoring the disc height appeared to improve LBP.
Introduction
Spondylolisthesis is a common spinal disease and according to the Wiltse classification system there are five types: isthmic, dysplastic, traumatic, degenerative and pathologic. 1 Isthmic spondylolisthesis (IS) is one of the most common types of spondylolisthesis with a prevalence of approximately 4–6% in the whole population. 2 Deficiency in the pars interarticularis of the lumbar vertebrae is a key characteristic of IS, usually occurring in L5 or L4. 3 Most patients with spondylolisthesis do not have any symptoms and they are often surprised to be informed they have spondylolisthesis following X-ray imaging. Patients typically visit a physician because of activities-associated low back pain (LBP). The LBP is sometimes accompanied by leg pain resulting from nerve root impingement.4,5 Most patients with symptomatic IS can be treated successfully with conservative methods, such as medication, physical therapy and activity modification. 6 In patients with persistent symptomatology or conservative management failure, surgical treatment should be considered.7,8 The goals of surgery for lumbar IS includes neurological decompression, stability reconstruction, restoration of disc space height or/and correction of deformity.9,10 Posterior lumbar fusion is considered an effective surgical approach for IS patients. Posterior lumbar interbody fusion (PLIF) can be fused with an autologous graft or a cage. Some complications, such as adjacent segmental degeneration and hardware-related problems, remain unavoidable. 11 Despite the risk of complications, PLIF has been widely performed and may have beneficial clinical outcomes for IS.12–14
Both LBP and leg pain are associated with IS. 15 Usually, leg pain is improved following surgery. 14 Posterior decompression and fusion are not as effective as expected in terms of improving LBP. 16 Although surgical techniques have improved, many patients still complain of postoperative LBP. 17 Drugs such as nonsteroidal anti-inflammatory drugs, sedatives, analgesics and narcotics are helpful for postoperative pain management.18–20 Some patients still complain of only achieving partial pain relief of postoperative LBP following medication use. This current study investigated the risk factors that contribute to postoperative LBP in the patients with IS that underwent PLIF.
Patients and methods
Study design and patient population
This retrospective study recruited consecutive patients with IS that underwent primary PLIF in the Department of Orthopaedics, First Affiliated Hospital of Harbin Medical University, Harbin, Heilongjaing Province, China and the Department of Rehabilitation, Second Affiliated Hospital of Heilongjiang University of Chinese Medicine, Harbin, Heilongjaing Province, China between January 2011 and January 2016. The operations were conducted by two senior spinal surgeons (Z.Y. & G.G.) at the two affiliated hospitals of Harbin Medical University. Final follow-up was recorded in January 2019. Every patient underwent X-ray, computed tomography and magnetic resonance imaging (MRI). IS was diagnosed according to the symptoms and radiological findings. The inclusion criteria were as follows: (i) the presence of IS of slippage grade 1 or 2 at L4 or L5. Radiological findings were consistent with that radicular level; (ii) patients that failed or refused to receive at least 6 weeks of conservative treatment; (iii) patients aged 18–65 years; (iv) all patients had radicular leg pain. The exclusion criteria were as follows: (i) patients with trauma, reoperation, neoplasm, infection, congenital deformations and chronic system illness, such as rheumatoid arthritis and neurodegenerative diseases; (ii) LBP or radiculopathy associated with an extraspinal cause; (iii) patients with a high grade of slippage (≥ grade 3); (iv) patients that had undergone secondary surgery at the same level or adjacent levels.
The study was approved by the Institutional Review Broad of Harbin Medical University, Harbin, Heilongjaing Province, China. All study participants provided written informed consent.
Clinical and radiographic outcome measures
Demographic, clinical, surgical and LBP data from all of the study participants were recorded. The presence of LBP was reported according to standardized Nordic questionnaires. 21 Preoperative and postoperative LBP severity were evaluated using a visual analogue scale (VAS) score. 22
Measurements were taken on standing lateral lumbar plain X-ray film radiographs. The segmental lordotic angle was measured between the upper endplate of the cranial side of the vertebral body and the lower endplate of the caudal side of the vertebral body for the operating level.23,24 The lumbar lordotic angle was measured between the upper endplate of the L1 vertebral body and the upper endplate of the S1 vertebral body.23,24The height of the intervertebral disc space was obtained from the mean value of the heights of the anterior, middle and posterior intervertebral discs. 25
The primary outcome measure was the change of VAS pain score of LBP. The preoperative VAS pain score was defined as the score before surgery but not specifically taken at the initial presentation. The postoperative VAS pain score was recorded clinically at the last follow-up.
Statistical analyses
All statistical analyses were performed using SAS software, version 9.1.3, (SAS Institute, Cary, NC, USA). Data are presented as mean ± SD or n of patients (%). The demographic characteristics and clinical data were compared between groups using χ2-test, Fisher’s exact test or t-test, as appropriate. Univariate and multivariate unconditional logistic regression were used to estimate crude and adjusted odds ratios and 95% confidence intervals, which were the measure of the association between the risk factors and LBP. For correlation analyses, Pearson’s correlation coefficient was used to assess the relationship between variables. All reported P-values were 2-sided and a P-value < 0.05 was considered statistically significant.
Results
This retrospective study recruited 244 patients that underwent primary PLIF surgery. Of these, 192 completed the final follow-up, which ranged from 12 to 70 months (mean follow-up duration, 39.8 months). There were 47 men and 145 women with a mean age of 43.01 years (range, 18–65 years). The completed follow-up rate was 78.7% (192 of 244 patients). Patients (n = 21) whose symptoms were not improved well or deteriorated following primary PLIF surgery received an MRI. Five of these patients required revision surgery for inadequate cord decompression and were excluded from the study. Six patients who underwent a second operation for infection were excluded from the study. In two patients, the pedicle screws in the slipping vertebra were pulled out when reduction was undertaken intraoperatively; and although reduction was accomplished via the use of bone cement in the pedicles to enhance the screws, these two patients were excluded from the study. The nerve root was injured in three patients during the operation. A total of 32 patients were lost to follow-up during the 4 years. An additional four patients died during the 4 years for unrelated reasons. All of these 52 patients were excluded from this study.
Table 1 presents the demographic and diagnostic characteristics of the patients. When the preoperative and postoperative VAS scores were compared at the final follow-up, there was a significant difference exhibited (P < 0.01). The mean ± SD VAS score decreased from 6.53 ± 1.23 preoperatively to 4.41 ± 1.63 at the final follow-up after primary PLIF surgery.
Demographic and clinical characteristics of patients (n = 192) with isthmic spondylolisthesis that participated in a retrospective study to investigate the risk factors for postoperative low back pain following primary posterior lumbar interbody fusion.
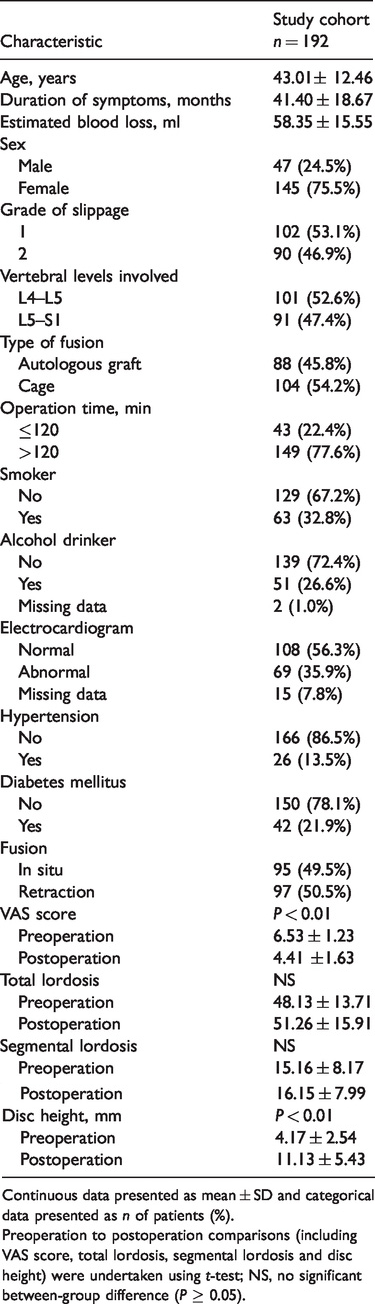
Continuous data presented as mean ± SD and categorical data presented as n of patients (%).
Preoperation to postoperation comparisons (including VAS score, total lordosis, segmental lordosis and disc height) were undertaken using t-test; NS, no significant between-group difference (P ≥ 0.05).
With regard to the primary outcome, the preoperative to postoperative change of LBP VAS pain score, the only significant difference was between patients with grade 1 slippage (mean ± SD, 2.42 ± 1.70) and patients with grade 2 slippage (mean ± SD, 1.78 ± 1.31) (P < 0.01) (Table 2).
Univariate analysis evaluating the association among demographic characteristics, magnetic resonance imaging findings and the preoperative to postoperative change in visual analogue scale (VAS) pain score.

Data presented as mean ± SD.
aP < 0.01; preoperative to postoperative change in VAS pain score compared using t-test.
Of the 192 patients with IS that underwent primary PLIF, 10 patients confirmed that their LBP had disappeared after the operation (5.2%) (Table 3). Most patients still complained about postoperative LBP in varying degrees. Symptom duration appeared to be associated with the disappearance of LBP but there was no statistical difference between the two groups. The grade of slippage was not associated with the postoperative disappearance of LBP.
Univariate analysis evaluating the association between patients with and without low back pain (LBP) following primary posterior lumbar interbody fusion.
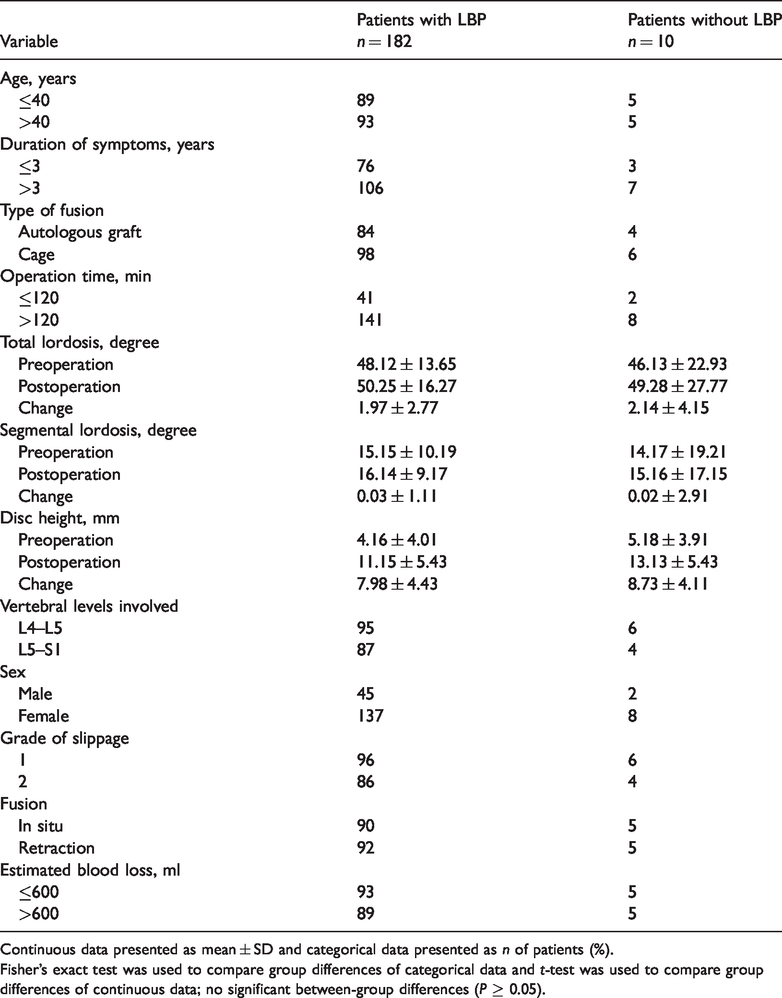
Continuous data presented as mean ± SD and categorical data presented as n of patients (%).
Fisher’s exact test was used to compare group differences of categorical data and t-test was used to compare group differences of continuous data; no significant between-group differences (P ≥ 0.05).
The mean ± SD preoperative LBP VAS score was 7.81 ± 1.19 in the 79 patients with symptoms for ≤3 years and 6.55 ± 1.26 in the 113 patients with symptoms >3 years (P = 0.02) (Table 4).
Univariate analysis evaluating the association among demographic characteristics, magnetic resonance imaging findings and the preoperative visual analogue scale (VAS) pain score.
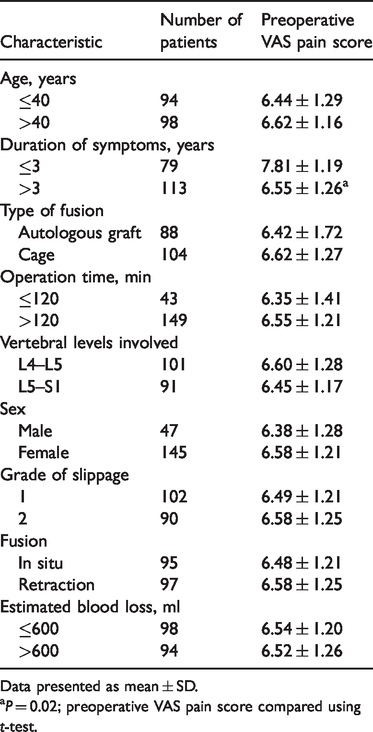
Data presented as mean ± SD.
aP = 0.02; preoperative VAS pain score compared using t-test.
The mean ± SD postoperative LBP VAS score was significantly greater in patients with grade 2 IS (4.80 ± 1.53) than the grade 1 IS group (4.07 ± 1.65) (P = 0.02) (Table 5). The mean ± SD postoperative LBP VAS score was 5.73 ± 1.47 in patients with symptoms for ≤3 years and 4.40 ± 1.74 in patients with symptoms >3 years, but difference was not significant.
Univariate analysis evaluating the association among demographic characteristics, magnetic resonance imaging findings and the postoperative visual analogue scale (VAS) pain score.

Data presented as mean ± SD.
aP = 0.02; postoperative VAS pain score compared using t-test.
There was no significant change in total lordosis and segmental lordosis after surgery, but the postoperative disc height was increased significantly (Table 1) (P < 0.01). There was a good correlation between the preoperative to postoperative change of VAS pain score and disc height (r = 0.99, P = 0.03) (Table 6).
Correlation analysis between the radiological outcomes and the preoperative to postoperative change in visual analogue scale (VAS) pain score.

aP = 0.03; Pearson’s correlation coefficient analysis.
Discussion
This current study showed that some postoperative LBP in patients with IS cannot be managed conservatively with medication and injections. Recently, a systematic review found that there was no strong or consistent association between IS and LBP in epidemiological studies of the general adult population. 26 The current study demonstrated that the surgical treatment of the involved vertebral segment effectively improved LBP regardless of whether an autologous graft or a cage was used for PLIF. A previous study reported that anterior lumbar interbody fusion was beneficial for LBP improvement for IS. 27 This current study found that PLIF provided relief of LBP and a possible explanation for the relief of LBP might that the fusion improves the stability of the lumbar spine. Both autologous grafting and cage fusion showed favourable clinical and radiological outcomes in the current study. This result was consistent with previous studies in terms of the type of fusion.14,28,29
The literature remains sparse regarding the risk factors of LBP after PLIF in patients with IS. In this current study, the grade of slippage was associated with the relief of LBP. Patients with grade 1 slippage experienced a significantly greater improvement of LBP after surgery compared with patients with grade 2 slippage (P < 0.01). Before PLIF surgery, patients with grade 2 slippage did not have more severe LBP compared with patients with grade 1 slippage. These current results suggest that PLIF can alleviate LBP much better in patients with grade 1 slippage compared with grade 2 slippage.
Patients with acute LBP (≤3 years of symptoms) showed significantly more severe preoperative LBP than patients with chronic LBP (>3 years of symptoms) (P = 0.02). Interestingly, patients with acute LBP did not show more severe LBP after surgery compared with patients with chronic LBP. Although they had more severe preoperative LBP, they appeared to recover better after the operation compared with the patients with chronic LBP. The literature remains limited on this issue. For example, two previous studies reported that the operative level was not associated with preoperative LBP.14,30 The current results support the previous conclusions.14,30 The postoperative VAS pain score was significantly associated with the extent of slippage (grade 1 versus grade 2) in the current study (P = 0.02).
Previous studies have aimed to investigate the differences between surgical methods, fusion material and surgical technique.28–32 In this current study, postoperative VAS pain score was not associated with type of fusion (autologous graft or cage) or the fusion techniques (fusion in situ or retraction), which was similar to the findings of previous studies.28–31 These findings suggest that different types of fusion do not influence the effect of surgery. It should be noted that it was not possible to pursue complete retraction in the current study because retraction would not contribute to the surgical outcome. Demographic characteristics of the patients and other surgery-related factors such as operation time, estimated blood loss and involved vertebral levels were not associated with the postoperative VAS pain score.
From these current findings, it would appear that the extent of slippage is an important factor contributing to LBP in patients with IS, which should be investigated in more depth in future research. These current findings also suggest that patients that have experienced symptoms for ≤3 years have more severe preoperative LBP. Despite their more severe preoperative LBP, they still achieved satisfactory improvements in postoperative LBP, which was also partially supported by a previous study by this research team. 14 In this current study, a significant correlation was only found between the preoperative to postoperative change of VAS pain score and disc height. The other radiological parameters of total and segmental lordosis did not show significant correlations. Although total and segmental lordosis increased postoperatively, the differences were not significant. These findings were inconsistent with anterior lumbar interbody fusion. 32 The anterior approach might be more beneficial for increases in lordosis but further research should be conducted to confirm whether increasing lordosis is essential for clinical improvement. The current study demonstrated that achieving a better disc height was associated with better improvements in postoperative LBP, which suggests that regardless of the type of fusion used, the surgery should aim to restore the disc height in order to reduce postoperative LBP.
This current study had several limitations. First, the retrospective nature of the study might have led to selection bias, although the database used in this current study was constructed without knowledge of the current hypothesis so all patient data were collected in an unbiased manner. Secondly, the study did not collect data on the fusion rate of patients, which is important because the fusion rate is a relatively important factor for postoperative LBP. Thirdly, all of the patients underwent open surgery, therefore the risk factors of postoperative LBP following minimally invasive surgery were not evaluated at this time.
In conclusion, over a mean follow-up duration of 39.8 months, patients with IS that underwent PLIF showed significant improvements in postoperative LBP as measured using a VAS pain score, although patients still reported LBP to some extent. The grade of slippage was a risk factor for LBP improvement, with patients with grade 1 slippage experiencing larger improvements in the postoperative VAS pain score that those with grade 2 slippage. Achieving a better disc height during surgery was associated with better improvements in postoperative LBP, which suggests that surgery should aim to restore the disc height in order to reduce postoperative LBP.
Supplemental Material
IMR890791 Supplemental Material - Supplemental material for Risk factors of postoperative low back pain for low-grade isthmic spondylolisthesis: a retrospective study
Supplemental material, IMR890791 Supplemental Material for Risk factors of postoperative low back pain for low-grade isthmic spondylolisthesis: a retrospective study by Fulin Guan, Hongna Yin, Lin Zhu, Zhizhuang Zhang, Qichang Gao, Tuo Shao, Weilong Tang, Guofa Guan, Ming Chen, Zhiyong Chi, Jiaao Gu and Zhange Yu in Journal of International Medical Research
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.