
Abstract
Objective
To investigate human papillomavirus (HPV) infection status and influencing factors among lesbians.
Methods
In August to October 2018, 300 lesbians were recruited in Beijing using snowball sampling. Sociodemographic characteristics, behavioural indices and HPV status were measured. Colposcopy was performed on participants with HPV genotypes 16 and 18 and on participants with other high-risk HPV subtypes and positive ThinPrep (TCT) results.
Results
The overall HPV-positive rate was 25%. High number of sexual partners, smoking, drinking, not using condoms and using sex toys during intercourse were identified as HPV infection risk factors. Of the HPV subtypes detected, 84% were high-risk HPV subtypes. The colposcopy results showed that 20 participants (80%) with HPV 16 and HPV 18 had cervical intraepithelial neoplasia I (CIN I) or above lesions. The colposcopy results also showed that 16 participants (64%) infected with other high-risk types of HPV virus and who had positive TCT results had CIN I or above lesions.
Conclusions
The cervical health of lesbians should not be neglected, and appropriate health education should be improved for this group.
Keywords
Introduction
Research on the psychosocial aspects of homosexual groups is relatively mature. However, most studies on physical health have focused on the health issues of gay men, such as human immunodeficiency virus (HIV) infection and sexually transmitted diseases.1,2 Studies on the physical health of lesbians are rare and have mostly being conducted in developed countries. 3 Cervical health is an important part of women’s health, and the prevention of cervical cancer is an important aspect of public health work. Women who engage in sex should have regular cervical health checkups. The human papillomavirus (HPV) test, ThinPrep cytologic test (TCT), and colposcopy are important procedures for detecting cervical lesions, especially cervical cancer. 4 HPV infection causes genomic instability and local immune suppression and is thus closely related to the occurrence and development of cervical cancer and other cancers. 5
HPV genotyping is useful to characterize HPV infection and provides a basis for the prevention and treatment of cervical cancer. 6 HPV infection with high-risk genotypes, such as HPV16 and HPV18, is closely related to cervical cancer. 7 Therefore, further medical procedures, such as TCT or colposcopy, are necessary for those infected with high-risk genotypes. 8 However, lesbians often neglect to attend such gynaecological examinations. Although lesbians engage in different sexual behaviours than heterosexuals, the risks associated with sexual intercourse are the same for both. Unsafe sex is associated with health risks. 9 In developing countries such as China, lesbians are a minority group and their identities are often concealed. Therefore, scant attention is paid to their reproductive health by medical staff, public health personnel and the media. The health education of this group must be improved. This study investigated the epidemic cervical health status and risk factors of cervical diseases among the lesbian population in Haidian District, Beijing, China. The aim was to obtain data that could inform future health interventions for this group.
Materials and methods
Participants
From August to October 2018, snowball sampling was used to recruit 220 lesbians in Haidian District, Beijing, from bars frequented by lesbians, or other places. Participants had to meet the following predetermined eligibility criteria: 1) never had a heterosexual partner, 2) 18 to 60 years of age, 3) lived in urban areas, 4) had had homosexual sex in the last year, and 5) not vaccinated with HPV vaccine.
Procedures
This study aimed to explore the prevalence and risk factors of HIV infection among lesbians in Beijing, China. Participants infected with high-risk HPV subtypes were screened for cervical diseases to explore cervical health. The following procedure was used: 1) A cross-sectional anonymous questionnaire comprising questions on sociodemographic characteristics and behavioural indices was administered. 2) Participants were asked to undergo an HPV examination and to avoid sex in the 24 hours before the medical examination. They were asked not to wash their vagina or use vaginal suppositories in the 48 hours before the examination, or to undergo vaginal endoscopy. Medical examinations were performed during non-menstrual periods. 3) Participants with different sociodemographic and behavioural characteristics were compared in terms of HPV prevalence. Then, factors influencing HPV infection were analysed and the type of HPV virus identified. 4) Colposcopy was performed on patients with HPV genotypes 16 and 18. TCT was performed on participants with high-risk HPV subtypes other than 16 and 18.
Measures
Questionnaire variables
The sociodemographic variables assessed were age, marital status, educational background, monthly income and family history of cancer. The behavioural indices measured were smoking; drinking; recent sleep situation; usage of condoms, fingertips or sex toys; number of sexual partners; age at first sexual act; level of awareness of disease risk and gynaecologic examinations attended.
HPV test
Twenty-one types of HPV genes were detected using DNA chip technology combined with in vitro amplification of polymerase chain reaction and reverse dot hybridization of DNA. Fifteen high-risk types were detected: HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66 and 68. Six low-risk types were detected: HPV 6, 11, 42, 43, 44 and CP8304 (81). Cervical mouth secretions were wiped with a cotton swab; a cervical brush was then rotated clockwise three to five times at the cervical mouth. The excess brush handle was broken and the brush head was placed in a specimen tube containing the cell preservation solution. The bottle cap was closed, marked well and sent for inspection (results were available within 24 hours). The main instruments and equipment used were the HPV Kit and Hybri-Max hybridizer (Guangdong Hybribio Biotech Co. Ltd., Guangdong, China).
TCT test
Cervical cells were detected using a liquid-based thin-layer cell detection system and classified by cytology. A thin-layer liquid-based cytology cervical brush was inserted into the cervical orifice. At the junction of the squamous columnar epithelium of the external cervical orifice, the cervical brush was rotated evenly in three circles around the outer mouth of the cervix. Then, the cervical brush was removed and placed into the TCT liquid-based cytology preservation solution for examination. Using the ThinPrep 2000 system, all cytological specimens were processed by liquid-based thin-layer cytology. The specimens were fixed with 95% alcohol and examined by microscopy after Papanicolaou staining. Following the new Bethesda System classification standard recommended by the International Cancer Society in 2001, the results of cytological diagnosis were classified as follows: 10 (1) Within normal limits; (2) atypical squamous cells of unknown significance (ASCUS); (3) atypical glandular cells (AGC); (4) atypical squamous cells excluding highly squamous intraepithelial lesions (ASC-H); (5) low-grade squamous intraepithelial lesions (LSIL); (6) high-grade squamous intraepithelial lesions (HSIL); (7) squamous cell carcinomas (SCC); and (8) adenocarcinomas (AC). The ASCUS diagnostic rate was no higher than two to three times the SIL rate. Cytological positive diagnosis indicated ASCUS/AGC lesions. The main instruments and equipment used were ThinPrep2000 automated cell microtome (Hologic, Marlborough, MA, USA) and a biomicroscope (Olympus Corporation, Tokyo, Japan).
Electronic colposcopy and cervical biopsy
To obtain histopathological results, we performed rapid frozen pathological biopsy or routine pathological biopsy at suspicious sites. The main instruments used were an electronic colposcope (Kimkuwait SLC 2000B, Philips, the Netherlands), a fully automatic dehydration instrument, a fully automatic embedding instrument, a semi-automatic slicing machine, a fully automatic dyeing slicing machine (all Leica, Solms, Germany) and a biomicroscope (Olympus Corporation, Tokyo, Japan).
Statistical analyses
Differences in frequencies among groups were calculated using the χ2 test. A logistic regression model was used to analyse factors influencing the results of the HPV test. Two-tailed tests were used and a significance of α = 0.05 was assumed. All data processing and analyses were carried out using SAS Version 9.4 for Windows (SAS Institute Inc., Cary, NC, USA).
Results
Sample
Of the 350 individuals invited to participate, 300 agreed (participation rate = 85.71%). The mean age (±standard deviation) was 28.18 ± 5.45 years. Participants had their first sexual intercourse at the age of 14 to 32 years; the median age was 22.54 ± 3.32 years. Sociodemographic and behavioural indices are shown in Table 1.
Sociodemographic and behavioural characteristics.

Comparison of HPV infection rate according to sociodemographic and behavioural characteristics
Of the 300 participants, 75 (25%) were HPV-positive. HPV infection rates of participants with different sociodemographic and behavioural characteristics were compared. Participants who had a large number of sexual partners, smoked, drank, did not use condoms and used toys during intercourse had high HPV infection rates (all P < 0.001) (Table 2).
Comparison of HPV infection rates according to sociodemographic and behavioural characteristics.

HPV: human papillomavirus.
Influencing factors of HPV infection
Factors influencing HPV infection were further explored using logistic regression analysis. The results showed that number of sexual partners (P < 0.001), smoking (P < 0.001), drinking (P < 0.001), condom use (P = 0.015) and use of toys during intercourse (P = 0.045) were factors influencing HPV-positive results. The effect of sociodemographic and behavioural factors on HPV infection is shown in Table 3.
Results of logistic regression analysis of factors affecting HPV infection.
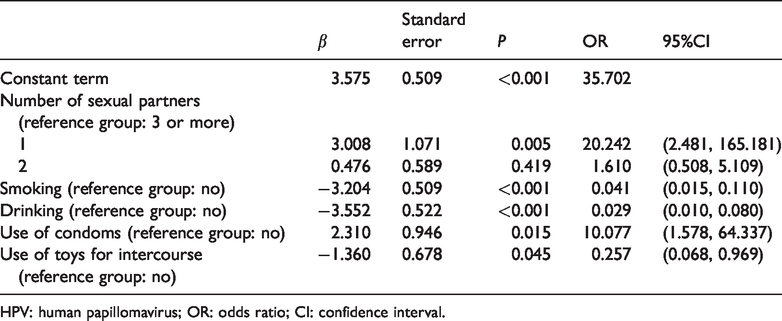
HPV: human papillomavirus; OR: odds ratio; CI: confidence interval.
Distribution of HPV subtypes
Of the 75 cases of HPV infection, 52 (69.33%) involved single subtype infection and 23 (30.67%) involved multiple subtype infection. Multiple infection subtypes were counted separately (total = 100). Of the multiple subtype infections, 84% were high-risk HPV subtypes and 16% were low-risk subtypes. Sixty-four participants had high-risk HPV subtype infections (high-risk HPV infection rate = 21.33%). The most common subtypes were HPV 16 (14%), 18 (13%), 52 (12%), 58 (12%) and 33 (11%). The distribution of subtypes is shown in Table 4.
Distribution of subtypes in 75 lesbians with HPV infection.

HPV: human papillomavirus.
TCT and colposcopy results for HPV-infected participants
Of the 75 cases of HPV infection, 25 were infected with HPV 16 or 18 subtypes. Of these, two cases were infected with both subtypes. The results of colposcopy and tissue biopsy were as follows: five cases of chronic inflammation, nine cases of cervical intraepithelial neoplasia (CIN I), six cases of CIN II, four cases of CIN III and one case of SCC. A total of 39 people infected with other high-risk HPV subtypes were examined using TCT; positive results were found for 25 of these. There were ten cases of ASCUS, six cases of AGC, three cases of ASC-H, three cases of LSIL and three cases of HSIL. The colposcopy results showed nine cases of chronic inflammation, five cases of CIN I, six cases of CIN II, four cases of CIN III and one case of SCC. In summary, of the participants infected with HPV 16 and 18, 20 (80%) were diagnosed with CIN I or above lesions. Of the participants infected with other high-risk types of HPV virus with positive TCT results, 16 (64%) were diagnosed with CIN I or above lesions.
Ethical considerations
The study protocol was approved by and carried out in accordance with the recommendations of Wuhan University School of Medicine Ethics Committee (No. 20170328). All subjects provided written informed consent in accordance with the Declaration of Helsinki.
Discussion
The findings indicated a total HPV-positive rate of 25% in the 300 participants, 64 of whom had high-risk HPV subtype infections. The high-risk HPV infection rate was 21.33%. The HPV-positive rate in this study was higher than that found in Western countries. Research shows that 13% or even 21% of lesbians show HPV infection. 11 In China, this may stem from a lack of sex education both in school and at home. Owing to traditional cultural values in China, sex education in schools is limited, tends to discourage students from premature sexual activity and rarely covers reproductive health. 12 In mainland China, homosexuality is stigmatized and homosexuals do not have access to reproductive health education. 13 Therefore lesbians who are sexually active often pay little attention to their sexual health. Moreover, the HPV vaccination rate and health education about the HPV vaccine are low in mainland China. 14 Although the 9-valent HPV vaccine was introduced to mainland China in 2018, the number of vaccinations is very low. In contrast, HPV vaccination is part of the national immunization strategies of many developed countries, and vaccination rates in these countries have increased. The effectiveness of the HPV vaccine for HPV infection has been confirmed. 15
The HPV-positive rate in the present study was higher than that found in a large survey of heterosexuality in the same area (Beijing), 16 and higher than in other studies using the same method of detection. For example, Zhao et al. 17 found a HPV-positive rate of 4.94% in 879 samples aged 25 to 29 years in Beijing. Cui et al. 18 conducted a survey of 719 urban women aged 30 to 39 years in Beijing and found a HPV infection rate of 6.95%. Lesbian groups have a high HPV infection rate, which may stem from the following factors. First, lesbian sexual intercourse includes kissing, oral sex, clitoral stimulation, genital grinding and the use of sexual devices. 19 HPV is transmitted by skin-to-skin or mucosa-to-mucosa contact and enters the body via cutaneous or mucosal trauma. 20 Some homosexuals insert unclean sexual devices into the vagina or share these devices, which can increase the spread of viruses and bacteria. 21 Second, although lesbian intercourse does not involve pregnancy and miscarriage risks, it is associated with risk of cervical disease. However, some lesbians may have insufficient knowledge of the causes of diseases such as cervical cancer and believe that homosexual practices cannot contribute to this disease. Hence, many ignore the importance of safe sex and do not consider the possibility of contracting cervical disease. For example, a lack of condom use or the use of fingertips to increase sexual pleasure may increase the spread of HPV. 22 Moreover, lesbians often fail to attend gynaecological examinations. 23 Third, although this study included only lesbians without heterosexual partners, many lesbians do have sexual intercourse with men. Male circumcision is an important cause of HPV infection in women. 24 The participants in the present study contracted HPV from sexual partners who had had sex with HPV-infected men. 25
The factors influencing HPV infection in this sample were further analysed. Drinking, smoking and excessive number of sexual partners were identified risk factors. Drinking and smoking can reduce autoimmunity. People with low immunity are easily infected with HPV virus.26,27 Lack of condom use is another risk factor, as there is a greater risk of HPV infection from direct sexual contact. 28 An individual engaging in unsafe sexual behaviours may become infected from a partner who has HPV. Use of sex toys was a risk factor, as such toys may be shared and not disinfected first, which increases the risk of HPV infection. Participants with multiple sexual partners had a higher HPV infection rate than those with a single sexual partner; as HPV is transmitted through sexual intercourse, such individuals are more likely to engage in sexual behaviour with carriers of the HPV virus.
HPV subtypes were analysed in this study. Of the 75 cases of HPV infection, 52 (69.33%) involved single subtype infection, and 23 (30.67%) involved multiple subtype infection. All the 21 subtypes were detected. Of the multiple infection subtypes, 84% were high-risk subtypes and 16% were low-risk subtypes, indicating that the high-risk HPV subtype infection rate was high. Most HPV infections are transient and as the virus can be eliminated by autoimmunity, only persistent HPV infection may cause cervical cancer and other cancers; however, high-risk HPV infection still requires attention. 29 The present findings showed that the most common subtypes were HPV 16 (14%), 18 (13%), 52 (12%), 58 (12%) and 33 (11%). This distribution is similar to those of other studies in China.30,31 As HPV 16 and 18 infections are high-risk factors for cervical cancer (and the infection rate is high), there is an urgent need to increase sexual health education and cervical cancer screening for lesbians. 32
Colposcopy was performed on participants infected with HPV 16 and 18 and with other high-risk subtypes with positive TCT results. Of the 50 cases, 36 (72%) were diagnosed with CIN I or above lesions. This finding indicates that the prevalence of cervical lesions is high in lesbians with high risk of HPV subtype infection. Therefore, lesbians should be screened for cervical diseases using HPV tests, TCT and colposcopy according to their specific conditions.
The present findings could inform future strategies to improve the sexual health of lesbian groups. The findings showed that the educational background of participants was generally high; 72.34% had college education or above. This suggests that targeted sexual health education should be strengthened for female college students, white-collar workers and other educated groups. The number of participants who had attended previous gynaecological examinations was relatively small compared with figures from previous studies, 33 suggesting that the participants in the present study attached little importance to gynaecological examinations. Thus, different strategies to improve health education for this group are necessary. Health education should address the following issues. First, lesbians must be educated about HPV and the spread of HPV and other sexual diseases through homosexual sexual behaviour. 34 The concept of safe sex should be emphasized to lesbians with multiple sexual partners and those who do not use condoms or use fingertips. The purpose and necessity of gynaecological examinations should be conveyed, and regular gynaecological examinations should be recommended. Second, many lesbians have a drinking habit, so lifestyle education is needed that (for example) emphasizes quitting smoking and limiting alcohol intake. 35 Third, HPV vaccines for lesbians should be promoted. Detailed information about vaccines, such as their function and who they are appropriate for, should be available. 14
The present study has some limitations. The snowball sampling method to increase the sample size; however, this sampling method may lead to selective bias. This was a cross-sectional study. However, the cervical HPV infection, TCT and colposcopy results varied at different times. Therefore, longitudinal research studies are needed to investigate this topic.
Conclusion
This study showed that lesbians have a high prevalence of cervical disease. Therefore, health education for this group needs to be strengthened. To improve the reproductive health of lesbians, healthy sexual behaviours and lifestyles should be advocated, and the rates of gynaecological examinations and HPV vaccination should be increased.
Footnotes
Acknowledgement
The authors thank all the participants who took part in the study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Humanities and Social Science Foundation of the Ministry of Education, China (15YJAZH094) and Fundamental Research Funds for the Central Universities of Harbin Engineering University.