
Abstract
Objective
We explored the prevalence of human papillomavirus (HPV) infection among women in Jinshan District, Shanghai.
Methods
We analyzed all HPV testing samples sent from our unit between December 2023 and April 2024. We reported the HPV prevalence overall, by age, and by subtype.
Results
In total, 3788 women aged 16 to 90 years had HPV test results. The prevalence of infection with any HPV subtype was 17.9%. The HPV prevalence by age group was: ≤30 years, 15.4%; 31–40 years, 14.7%; 41–50 years, 17.0%; 51–60 years, 22.4%; >60 years, 31.0%. Among HPV-positive women, 80.6% had infection with one subtype, 16.4% had dual infection, and 3.1% had three or more subtypes detected. We found 640 cases (16.9%) of infection with high-risk HPV subtypes and 191 cases (5.04%) of infection with low-risk HPV subtypes. The most common high-risk subtypes were HPV 52, 53, 58, and 16; the most common low-risk subtypes were HPV 81, 70, and 42.
Conclusion
We detected ≥1 HPV subtype among most women in our study. The prevalence of HPV was lowest in younger women and highest in women age >60 years. Tailored strategies for older women are needed to prevent HPV infection and cervical cancer.
Introduction
Human papillomavirus (HPV) is a small molecular double-stranded DNA virus transmitted through sexual contact and through skin lesions. 1 HPV infection is the most widespread sexually transmitted infection worldwide.2,3 Most cervical cancers are caused by HPV infection,1,2 which can be detected by HPV DNA screening. 3 Cervical cancer is one of the most common types of cancer among women globally, 4 making HPV infection critically important in relation to the incidence of cervical cancer.5–8 Cervical cancer ranks seventh among malignant tumors that affect Chinese women. 9 More than 200 HPV genotypes have been identified, which are divided into high-risk and low-risk subtypes9,10 according to their carcinogenicity and infection rate. There are differences in the frequency of HPV genotypes among women with HPV infection according to different ages.11,12
Cervical cancer is a serious public health issue in Shanghai, China, particularly among women of reproductive age. 9 Specific screening services and preventative health services are crucial to prevent and control the incidence of cervical cancer. The two most important preventative health services currently available to women are HPV vaccination and routine Pap smears. HPV vaccines represent the potentially most effective form of preventing infection with high-risk HPV strains, which contribute to over 70% of all cervical cancers. 13
The aim of this study was to clarify the status of HPV infection and HPV subtypes among women of different age groups in Shanghai. Our findings can be useful in developing effective measures and approaches to preventing infection with both high- and low-risk HPV subtypes.10,11 To better understand the prevalence of HPV infection among women in Shanghai, we collected and analyzed data of women in all age groups who underwent HPV testing at Tinglin Hospital in Jinshan District between 2023 and 2024.
Methods
We conducted a cross-sectional study to investigate the incidence rate of HPV infection and the corresponding age-specific distribution among women in the Jinshan District of Shanghai. We collected data from HPV-positive patients tested in Tinglin Hospital. To clarify the age-specific HPV infection patterns, we investigated the distribution of HPV genotypes among women of different ages.12,14
This study was conducted according to the principles of the Declaration of Helsinki of 1975, as revised in 2013. Signed, informed consent was obtained from each participant before their inclusion in the study and at each additional follow-up observation. Each participant was given written information regarding the aims of the study, study procedures, potential risks and benefits, and other relevant information. To ensure the quality and transparency of this observational study, we adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 15 This study was approved by the Ethics Committee of Tinglin Hospital, Jinshan District, Shanghai (approval number: TLH-2024-001).
Data collection
The data in this study were collected from gynecology and physical examinations conducted at our hospital between December 2023 and April 2024 among women aged 16 to 90 years. Participants were divided into five age groups: ≤30, 31–40, 41–50, 51–60, >60 years, with 700, 1183, 1046, 549, and 310 women in each age group, respectively.
The participant age range in this study (16–90 years) was chosen to encompass younger people who would benefit from HPV vaccination as well as older people who are at risk of cervical cancer owing to long-term HPV infection. This was in alignment with the 2030 cervical cancer elimination strategy set out by the World Health Organization (WHO), with the following targets: HPV vaccination coverage for 90% of girls by age 15 years; 70% of women screened using high-performance tests at least twice in their lifetime; and treatment for 90% of women with identified cervical disease. 16 The age group 65 to 69 years can offer data that improves understanding of the HPV prevalence and the need for screening, which can be used to support the WHO global health targets.
Recruitment
Participants were recruited during the study period via notification during their routine gynecological and physical examination at our hospital. The inclusion criteria were women aged 16 to 90 years who provided written consent and agreed to participate in the study. Exclusion criteria were a history of cervix surgery, history of cervical cancer, and any other condition that would interfere with sample collection and testing.
Specimen collection
Specimen collection and preservation for HPV detection was carried out by a gynecologist (with the title of the attending doctor or above) at our hospital. First, the entire cervical os was exposed using a vaginal speculum. Excess secretions were wiped from the cervical mouth with an untreated cotton swab in physiological saline. Then, a disposable cervical brush was inserted into the cervical canal and rotated four to five times clockwise or counterclockwise to obtain an appropriate sample of cells. After removing the brush from the vagina, the gynecologist visually examined the specimen to ensure that it was appropriate for laboratory analysis and contained an adequate number of epithelial cells. The cervical brush head was then placed into a tube containing cell preservation solution. The tube was sealed, labeled, and stored vertically at room temperature until the sample was sent for detection. Storage time before testing was not to exceed 48 hours at room temperature or 7 days at 2°C to 8°C, and testing was to be completed within 1 week.
Laboratory testing
The laboratory procedure involved nucleic acid extraction and preservation to confirm the accuracy of polymerase chain reaction (PCR) analysis. We used the Jindi safety automatic nucleic acid extraction and purification instrument (EB-1000; Hangzhou Dean Biotechnology Co., Ltd., Hangzhou, China); a real-time fluorescence quantitative PCR instrument (MA6000; Suzhou Yarui Biotechnology Co., Ltd., Suzhou, China); manual oscillator and uniform thermal sealing film instrument (Mona Biotechnology Co., Ltd. Company, Shanghai, China); microporous plate centrifuge (HL-25W), micro palm centrifuge (HL-6KS), and vortex mixer (Vortex-2; Shanghai Huxi Industrial Co., Ltd., Shanghai, Chin); and 0.2 mL PCR 96-well plate (half skirted, transparent enzyme-free heat-free) and induction sealing film (Mona Biotechnology Co., Ltd.). We also used an HPV nucleic acid typing detection kit (aluminum PCR melting curve method), nucleic acid extraction or purification reagents, and quality control products (Hangzhou Jindian Biotechnology Co., Ltd., Hangzhou, China). This kit can detect 23 HPV genotypes. The 17 high-risk HPV subtypes are HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82. The six HPV low-risk subtypes are HPV 6, I1, 42, 70, 81, and 83.
The HPV nucleic acid extraction procedure was as follows. The HPV specimen was mixed for a few minutes. In total, 400 μL of sample was added to nucleic acid extraction or purification reagents. For each batch of HPV sample, the reagents in the same batch underwent quality control testing. We used the EB-1000 instrument to automatically extract nucleic acid, according to the manufacturer’s instructions. The extracted nucleic acid was then amplified and we conducted real-time fluorescence quantitative PCR, according to the manufacturer’s instructions.
Statistical analysis
We used IBM SPSS version 25 (IBM Corp., Armonk, NY, USA) in the statistical analysis. The χ2 test was used for all age groups, p < 0.05 was considered statistically significant.
Results
Of 3778 specimens from women aged 16 to 90 years, 679 specimens were positive for HPV infection, yielding an HPV infection rate of 17.93%. The HPV infection rate among women in the age group ≤30 years was 15.43% (108/700), the rate in the age group 31 to 40 years was 14.71% (174/1183), that in the age group 41 to 50 years was 17.02% (178/1046), that in the group aged 51 to 60 years was 22.40% (123/549), and the infection rate in the age group >60 years was 30.97% (96/310), as shown in Table 1. In a comparison by age group, we found no differences between the age groups ≤30 years and 31 to 40 years or between the age groups 51 to 60 years and >60 years. The age groups ≤30 years, 31 to 40 years, and 41 to 50 years were different from those aged 51 to 60 years and >60 years. Overall, the difference in the rate of HPV infection among women in different age groups was statistically significant (χ2 = 55.204, p < 0.05).
Human papillomavirus infection among women at different ages.

Distribution of single or multiple HPV infections among women at different ages
Among the 679 cases of HPV infection, the rate of single, double, and triple or more HPV infection among women at different age groups was ≤30 years: 79.63% (86/108), 17.59% (19/108), and 2.80% (3/107); 31 to 40 years: 84.48% (147/174), 12.7% (21/174), and 3.45% (6/174); 41 to 50 years: 83.71% (149/178), 15.17% (27/178), and 1.12% (2/178); 51 to 60 years: 77.24% (95/123), 70% (23/123), and 4.07% (5/123); and >60 years: 72.92% (70/96), 21.88% (21/96), and 5.21% (5/96), respectively (Figure 1). According to the data, most women had single HPV infection, followed by double infection. The age groups with the highest rates of single infection were 31 to 40 years and 51 to 60 years, followed by 31 to 40 years, and >60 years. The rate of infection with two HPV subtypes was highest in the age group 41 to 50 years. The rate of infection with three HPV subtypes was relatively low in all age groups. Analysis of overall HPV infections in different age groups showed an inverted “U” shape (Figure 2).
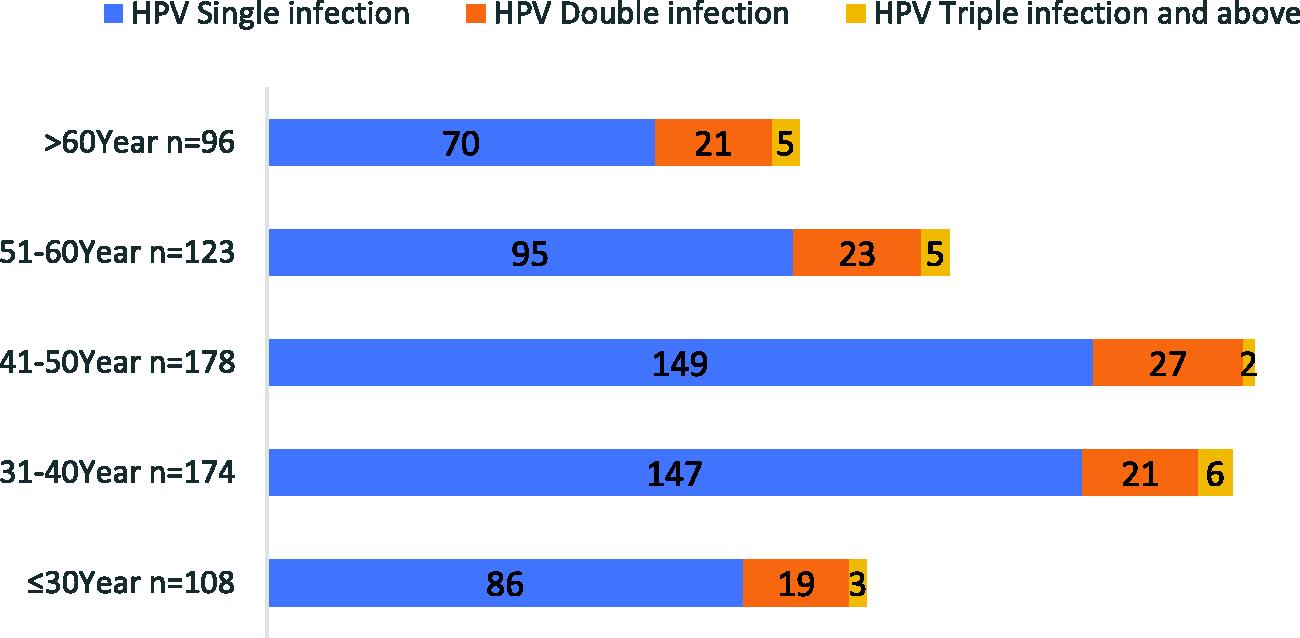
Women infected with human papillomavirus (HPV) by age group.
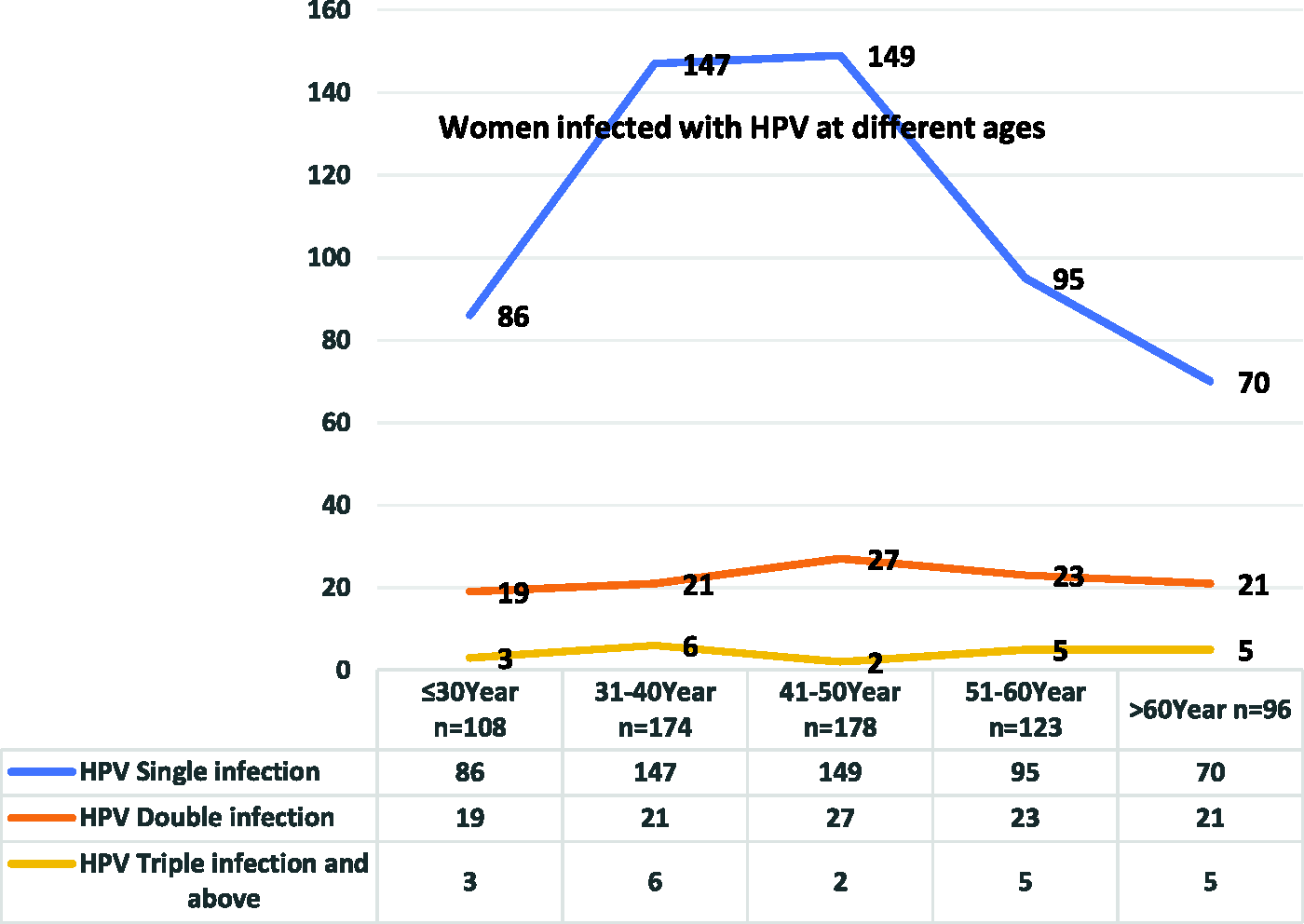
Distribution of single and multiple human papillomavirus (HPV) infections among women of different ages.
Distribution of high- and low-risk HPV subtypes among women in different age groups
Among the 679 cases of HPV infection found among the 3788 collected specimens, we detected 831 HPV subtype genes (including repeated counts for multiple infections). The infection rates for single infections with high-risk and low-risk HPV subtypes were 16.90% (640/3788) and 5.04% (191/3788), respectively (Tables 2 and 3). Analysis of HPV subtype infections showed that 23 subtype genes were detected. Among them, the most frequent single infections with high-risk HPV subtypes were, in descending order, HPV 52, 53, 58, 16, 66, 51, 31, 68, 18, 56, 35, 45, 39, 59, 73, 82, and 33 (Figure 3). The most frequent single infections with low-risk HPV subtypes were, in descending order, HPV 81, 70, 42, 6, and 11. The infection rate for the HPV 83 subtype was extremely low (Figure 4).
Distribution of single infections with high-risk human papillomavirus (HPV) subtypes among women of different ages.

Distribution of single infections with low-risk human papillomavirus (HPV) subtypes among women of different ages.


Distribution of single infections with high-risk human papillomavirus (HPV) subtypes among women of different ages.
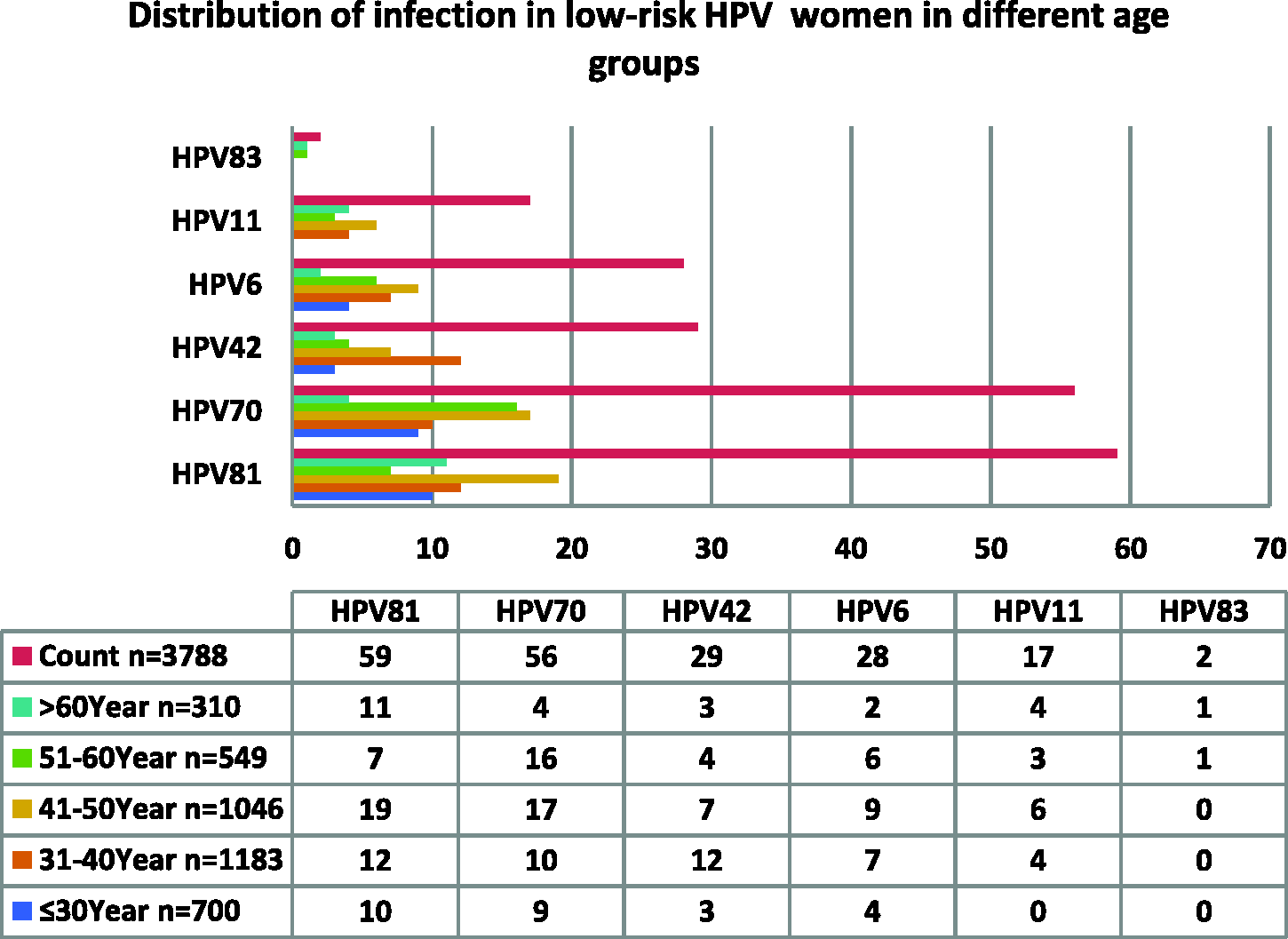
Distribution of low-risk human papillomavirus (HPV) infections among women in different age groups.
Discussion
Studies have shown that cervical cancer is a leading cancer among women worldwide, and most cases occur in low- and middle-income countries. 17 The literature shows that HPV DNA can be detected with nucleic acid testing of specimens from patients with cervical cancer; 18 thus, the occurrence of cervical cancer is closely related to HPV infection. Women with long-term HPV infection are at greater risk for developing cervical cancer.19,20 In our analysis regarding the prevalence of HPV infection among women of different ages in Jinshan District, Shanghai, 679 cases of HPV infection were detected among specimens from 3788 women, with a total infection rate of 17.93%. Among all age groups, the HPV infection rate increased with age and was highest in individuals over 60 years old (30.97%). This trend may be associated with a decrease in hormones, reduced immunity, and other factors that increase the likelihood of infection in older women. Research indicates that hormonal changes associated with menopause, such as decreased estrogen levels and thinning of the vaginal and cervical epithelium, as well as age-related immune senescence, contribute to the higher infection rates observed in older age groups. 21 Conversely, the infection rate was lowest in the age group 31 to 40 years (14.71%), which may be owing to higher metabolism, robust hormone secretion, and strong immune resistance, all of which decrease the probability of infection in younger women. Younger adults generally have a more effective immune response and better physiological resilience, enabling them to clear HPV infections more efficiently than older adults. 22 Whereas the overall HPV infection rate in this study was similar to that in other regions of China, the distribution of HPV subtypes varies by region. Regional differences in the HPV subtype prevalence could be owing to variations in population genetics, sexual behavior, public health practices, and screening protocols. 23
Implications for practice
Our study findings have many real-world implications. The results revealed that older women are more prone to HPV infection, highlighting that public health strategies should be tailored according to age. This involves improving screening and vaccination programs for older women who are more likely to develop persistent infection and therefore be at greater risk of cervical cancer. We also found regional differences in the circulating genotypes of HPV. This information can be useful for local public health initiatives, helping practitioners in designing prevention or intervention strategies relevant to their region within the context of the epidemiological profile for that region.
Women in Shanghai have access to various health services, such as Pap and HPV DNA testing. Although these services help in detecting HPV infection, the incidence of cervical cancer remains high. Thus, it is critical to provide screening services that are affordable to all women, regardless of socioeconomic status or geographic region. Local health initiatives must be optimized to meet the WHO recommendations for the global elimination of cervical cancer and to reduce the number of cases of cervical cancer among women of all ages in China and globally.
Recommendations for research
Further research is crucial to build on the findings of this study. Such research should include more extensive longitudinal studies to clarify the potential causality between age-related physiological changes and the prevalence of HPV infection. Additionally, investigating the feasibility and efficiency of age-specific public health interventions to reduce the HPV prevalence and cervical cancer incidence is imperative. Researchers should also strive to enhance the diversity of geographic sampling and the age-group composition in study populations from China for a more comprehensive understanding of the HPV epidemiology and influence of the sociocultural environment on HPV infection. China's geographic makeup is relatively complex, comprising many cultural and ethnic contexts and socioeconomic conditions, resulting in differences in the rate and type of HPV infection. The findings of more comprehensive research will assist public health programs in developing more effective strategies to decrease the HPV incidence and reduce the related burden of cervical cancer worldwide. Each region should increase prevention, early detection, and early treatment according to the regional infection rate by HPV subtype and age group to improve women's health. This study provides a reference for the detection and analysis of infection with HPV subtypes among women of all ages in different geographic regions.
Limitations and strengths
Whereas the present study has some critical limitations, it also possesses considerable strengths. Because of its cross-sectional design and focus on a single district in Shanghai, this study could not capture changing patterns or cause-and-effect relationships over time among age, immunity, and HPV infection. In addition, the study sample, drawn from a single district of Shanghai, may not be fully representative of other regions with distinct demographic or socioeconomic characteristics. The study's most notable strength lies in its comprehensive age range, which revealed that the highest HPV infection rates are among older women. This is a pivotal finding that warrants special attention from healthcare professionals. Overall, the present study provides one of the most extensive and balanced overviews of the epidemiology of HPV across the lifespan in Shanghai, China.
Conclusions
In this study, we assessed the HPV infection prevalence among women in Jinshan District, Shanghai, stratified by age, to examine the differences and patterns in the distribution of HPV subtypes across age groups. Our findings show that HPV infections are highest among women aged over 60 years. This may be owing to the natural aging process in women, characterized by decreased hormonal levels, lowered immunity, and susceptibility to persistent infections. The lowest prevalence of HPV infection was observed in the age group 31 to 40 years, which is likely owing to improved immunity and better physiological remediation in young adults.
Our study also clarified variations in the prevalence of HPV subtypes in different areas, indicating the need for region-specific public health initiatives. These findings are imperative for improving vaccination and screening programs, particularly for older women, who tend to have more persistent infections and therefore, a greater risk of developing cervical cancer.
This study adds to the accumulating evidence on HPV infection and cervical cancer prevention, highlighting the need for targeted screening and vaccination programs developed on the basis of the regional age distribution and HPV prevalence.
Footnotes
Acknowledgements
We thank Chen Shanshan and Chen Jing for their help with the completion of this manuscript.
Author contributions
Xiao Tao wrote the manuscript; Chen Shanshan and Chen Jing conducted statistical analysis of the data.
Data availability statement
The data cannot be made public owing to patient privacy issues.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research was supported by the Hospital-level Project Fund of Tinglin Hospital, Jinshan District, Shanghai (no. TLYY-KYKT-2024-01).