
Abstract
This report highlights an unusual case of a woman in her 70s who presented with diffuse idiopathic skeletal hyperostosis and an initial symptom of spinal cord compression and associated spinal degeneration. She presented with progressive thoracolumbar pain, bilateral lower limb weakness, and sensory deficits. Imaging showed continuous osteophytes in the anterior and lateral spine, multiple levels of intervertebral space narrowing, marked ligament ossification at T10/11, and severe spinal stenosis. Diffuse idiopathic skeletal hyperostosis was diagnosed and spinal cord compression was significantly reduced after laminectomy. Although diffuse idiopathic skeletal hyperostosis is relatively common in elderly patients, cases of spinal cord compression are still rare, and the combination of intervertebral space stenosis, and ossification of the ligamentum flavum may be misdiagnosed as degenerative spondylopathy. This case suggests the possibility of intervertebral stenosis and ossification of the thoracic ligamentum flavum coexisting with diffuse idiopathic skeletal hyperostosis, highlighting the importance of diagnostic imaging in the early stage of patient management.
Keywords
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is a common skeletal condition observed in older adults. It affects about 3% of individuals aged >40 years, with higher prevalence rates in those aged >65 years. In 1950, Forestier and Rotes Querol named this condition as “senile ankylosing spondylolisthesis” to highlight its age-related nature. 1 The conventional diagnostic criteria for DISH consists of the following three main elements: presence of vertebral flow ossification in at least four adjacent vertebrae; preservation of disc height and absence of significant degenerative changes in the affected vertebral segments to differentiate DISH from degenerative spondylosis; no ankylosis at the small joint interface and no erosion, sclerosis, or fusion of the sacroiliac joints that would distinguish DISH from ankylosing spondylitis (AS). 2 However, in the clinical setting, DISH can occur in conjunction with other conditions. 3 DISH is mainly considered a disease of ligament ossification; neurological complications may occur when ossification of the posterior longitudinal ligament or ossification of ligamentum flavum (OLF) is involved; 4 however, this is a rare occurrence. 5 This poses a diagnostic challenge. This case report describes a patient with DISH who presented with thoracic spinal cord compression as the initial symptom and exhibited thoracic disc degeneration and OLF. The condition was initially mistaken for degenerative spinal disease.
Case report
We have deidentified all patient details. The reporting of this study conforms to the Case Report (CARE) guidelines. 6
Clinical presentation
The patient was a woman in her early 70s who had presented 6 years previously with progressive lower limb numbness and weakness, which had started in the feet and had gradually progressed upward. In the previous 6 months, the patient was unable to walk independently, experienced significant gait instability and had a sensation of girdling and numbness in both lower limbs; she had no urinary or fecal obstruction. Neurological examination revealed grade 3/5 muscle strength in both lower limbs, hyperreflexia, diminished proprioception, and temperature sensation below the groin. The patient has a history of hypertension for 10 years and diabetes for 20 years. There was no relevant personal or family medical history of surgery. The patient denied the use of stimulants and/or irritants, and other risk factors were ruled out.
Imaging findings
Magnetic resonance imaging (MRI) showed local thickening of the ligamentum flavum; slight bulging of some intervertebral discs, especially the thoracic 10/11 disc; narrowing of the spinal canal; and compression of the spinal cord at the corresponding level (Figure 1). The signal intensity of thoracic intervertebral discs decreased on T2-weighted imaging.

(a) MRI sagittal view shows a posteriorly protruding disc and calcified ligamentum flavum at T10/11, compressing the spinal canal from both directions and (b) herniated disc and narrowed spinal canal.
X-ray imaging showed mild hyperostosis and sharpening of the upper and lower corners of the anterior edge of the thoracic vertebrae, with marginal sclerosis. The intervertebral space was unequal in width, locally narrowed, and blurred; the attachments were clear (Figure 2(a) and (b)). Anteroposterior and lateral computed tomography (CT) images showed a clear and more continuous osteophyte proliferation on the anterolateral side of the vertebral body at multiple levels (Figure 2(c) and (d)). CT cross-sectional images provided further details of the interior of the vertebral body, showing the presence of Schmidt’s nodes in the pyramids, marginal osteophytes, spinal canal stenosis, OLF, and compression of the spinal cord (Figure 2(e) and (f)).
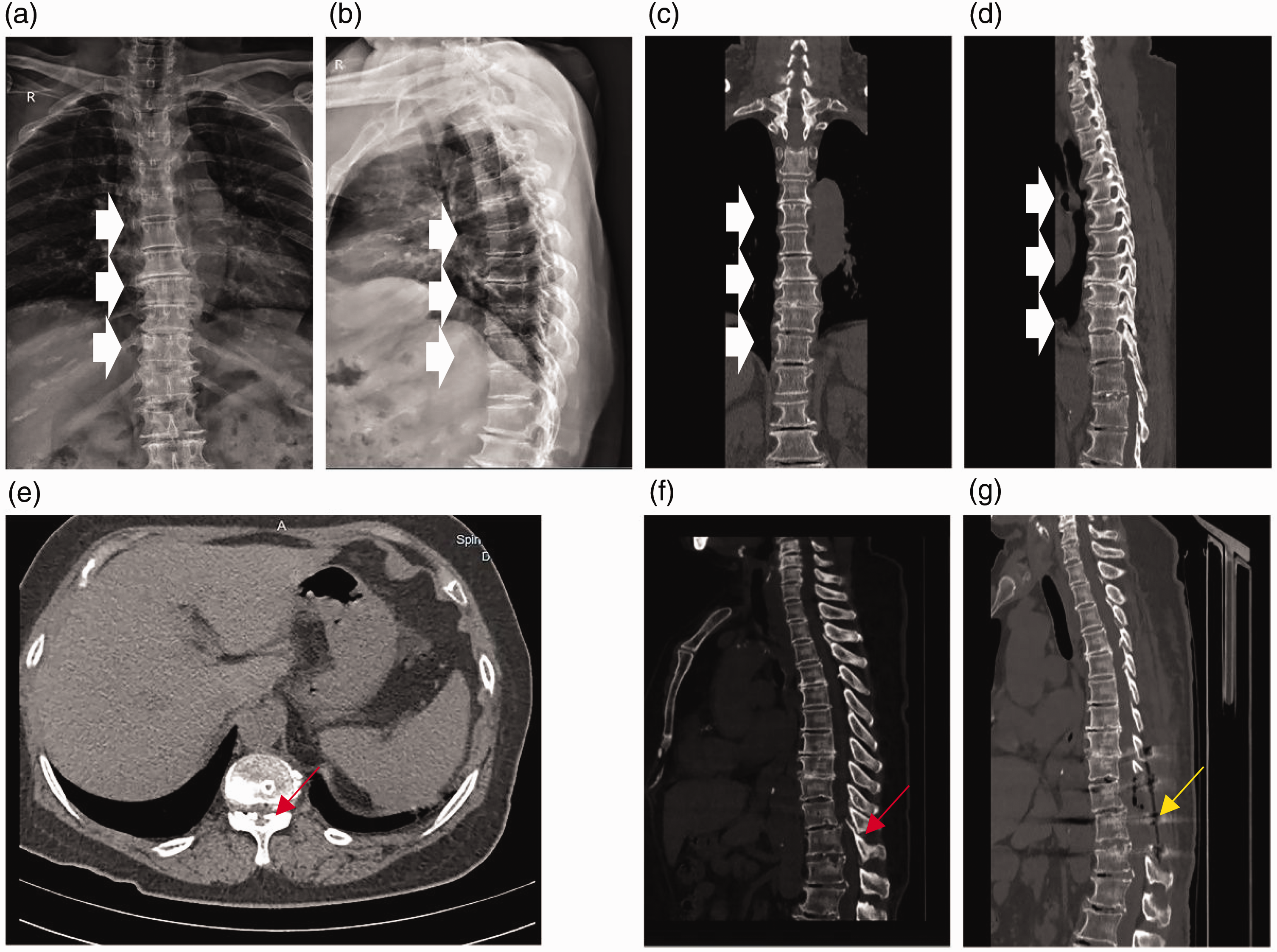
Anteroposterior radiographs. (a) Lateral radiographs; (b) CT anteroposterior radiographs; (c) Anterolateral sagittal section of the CT cone; (d) Preoperative images showing osteophyte proliferation of more than three consecutive segments in the anterolateral vertebral body (solid white arrows); cross-sectional (e) and sagittal (f) CT images revealed ossification of the ligamentum flavum, spinal canal stenosis, and significant spinal cord compression (red arrow) and (g) postoperative CT image showing spinal cord decompression after laminectomy (yellow arrow). CT: computed tomography.
Diagnosis
Comprehensive investigations and imaging tests helped to establish a diagnosis of thoracic compression and DISH.
Treatment and outcome
The patient was first examined at the Department of Neurology, Xinhua Hospital, where spinal cord compression was initially suspected on examination. Therefore, MRI was performed, and the initial diagnosis was disc herniation. After ineffective conservative treatment, the patient was transferred to the Department of Orthopedics in the same hospital for elective surgery. X-ray and CT examination confirmed DISH and spinal cord compression. Thoracic vertebra 10/11 laminectomy was administered as treatment (Figure 3). The surgery was successful, as indicated by significant postoperative reduction in spinal cord compression (Figure 2(g)). After dehydration, circulatory improvement, nerve nutrition, and symptomatic treatment, the patient recovered smoothly. Appropriate functional exercises and regular follow-up after the surgery are necessary for the muscle strength recovery.
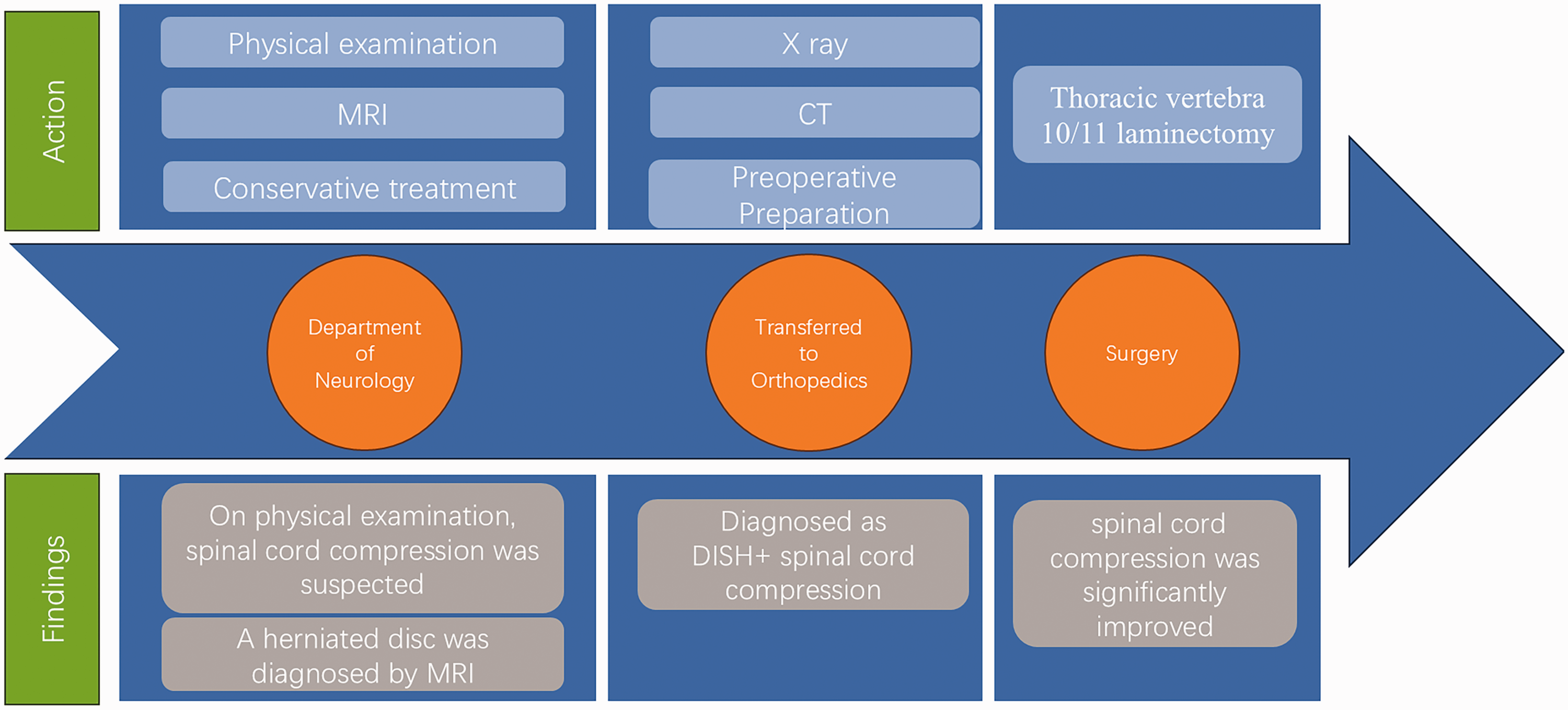
Chronological flow chart.
Discussion
DISH is a noninflammatory bone disorder characterized by calcification and ossification of ligaments. DISH is also known as senile ankylosing osteodysplasia and is easily confused with AS, degenerative spinal disease, and other diseases. The patient in the present case met the diagnostic criteria for DISH proposed by Resnick; features of this case included the following: ossification of the anterolateral edge of ≥4 consecutive vertebral bodies and no ankylosis of vertebral facet joints or sacroiliitis. However, the special contradiction of this case was that there was coexisting intervertebral space stenosis, which led to an incorrect diagnosis of degenerative changes of the spine. Degenerative osteoarthropathy of the spine usually involves parts of the spine with large range of motion and weight-bearing joints. Degenerative osteophytes in the thoracic spine are rare, and extensive calcification of the anterior longitudinal ligament is uncommon. In the present case, imaging showed that the patient’s facet joints were normal without any signs of degeneration; thus, degenerative osteoarthropathy of the thoracic spine was ruled out. Few studies have reported on intervertebral space lesions in DISH. The mechanism of this contradictory phenomenon may be related to the superposition effect of age-related degeneration. With aging, the human intervertebral disc and articular cartilage gradually degenerate. DISH is characterized by the abnormal ossification of ligament and tendon attachment points of the spine. The relationship between DISH and disc degeneration remains unclear, and further in-depth studies are needed to reveal the specific links between them.
As a systemic disease of abnormal bone formation, DISH may affect the metabolism and structure of ligaments. Calcification of the ligamentum flavum is an abnormal mineralization phenomenon of ligaments. OLF and calcification are two different stages of the same disease. In total, 4.9% of DISH patients had OLF. 7 Calvanese F. reported the first case of cervical OLF (C-OLF) coexisting with DISH, resulting in spinal canal compression. It is believed that the coexistence of C-OLF and DISH may be caused by the change of mechanical stress in the cervical spine and the tendency of bone formation in patients with ligament ossification. 8 In the present case, the patient had a 20-year history of diabetes mellitus, a common risk factor for DISH and OLF. The hyperglycemic state can lead to the loss of elastic fibers and the change of collagen fibers in the ligamentum flavum, with increased deposition of calcium salts. DISH may increase the risk of ligamentum flavum calcification by affecting the calcium and phosphorus metabolism and cytokine levels in vivo; this finding needs to be confirmed in future studies. Another possible factor is the change in mechanical stress caused by thoracic DISH and disc degeneration. Osteophyte proliferation in the anterior approach of the mid–upper vertebra and intervertebral space narrowing may lead to calcification of the ligamentum flavum at T10–11 level to bear the greater biological stress.
DISH is generally a benign radiological disorder with common initial symptoms of thoracic spine stiffness and mild pain; the coexistence of spinal cord compression is rare. 5 Spinal cord compression may occur when ossification of the posterior longitudinal ligament or OLF is involved. 4 For neurologists, DISH is an uncommon cause of spinal cord compression, which can easily be missed in the process of diagnosis and treatment. The patient in the present case also had vertebral space stenosis, which was contradictory to the diagnostic criteria and could easily result in misdiagnosis. Therefore, comprehensive diagnosis and treatment should be combined with the patient’s personal information, medical history and imaging examination, results.
Conclusions
This report highlights the rare case of a patient with DISH and spinal cord compression as the initial symptom and concurrent disc degeneration and OLF. Its coexistence with intervertebral space stenosis may lead to misdiagnosis. Laminectomy and decompression can relieve the symptoms of spinal cord compression. This case shows that clinicians should be aware of the coexistence of DISH with intervertebral space stenosis and calcification of the thoracic ligamentum flavum during the diagnosis process, highlighting the importance of imaging diagnosis in early diagnosis and the role of a multidisciplinary approach in the management of complex spinal diseases. Prompt identification and surgical intervention may prevent severe neurodegeneration.
Footnotes
Acknowledgements
I would like to thank Mr. Xu Lichen, Mr. Xia Dongxue, and Mr. Tang Wei for their guidance. I would also like to thank my family and classmates for their companionship and support.
Author contributions
Zhang Jiaqi, Xu Lichen, Xia Dongxue, and Tang Wei were all involved in the care of the patients. Xu Lichen, Xia Dongxue, and Tang Wei provided case materials. Zhang Jiaqi was responsible for writing the entire manuscript. Xu Lichen assisted with manuscript writing and provided important theoretical support. Tang Wei and Wang Wei were responsible for follow-up guidance and coordination of manuscript revision. Wang Wei provided financial support. All authors have read and approved the final submitted manuscript.
Consent to participate
The patient provided his informed consent for surgical procedure and utilization of clinical data for the present study.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article and from corresponding authors upon reasonable request.
Declaration of conflicting interests
None of the authors have any potential conflict of interest.
Ethics approval
Not applicable.
Funding
This study was supported by the Liaoning Provincial Department of Education’s Basic Research Program for Colleges and Universities (LJ232411258026).