
Abstract
Objective
Rib fixation is an effective treatment for patients with multiple rib fractures. We retrospectively evaluated the application of a four-claw titanium plate in patients with rib fractures.
Methods
Fifty-four patients treated for multiple rib fractures in our hospital from 2012 to 2016 were divided into a surgery group (n = 27) and conservative treatment group (n = 27). The patients’ age, sex, cause of fracture, Injury Severity Score, chest Abbreviated Injury Scale score, number of ventilator days, and length of hospitalization were recorded.
Results
The mean duration of mechanical ventilation was 4.5 ± 0.7 and 7.9 ± 1.7 days in the surgery and control group, respectively, with a significant difference. The length of intensive care unit stay was also significantly different between the groups (5.9 ± 0.6 vs. 10.6 ± 1.9 days, respectively). The length of hospital stay and recovery time to regular life in the surgery and control group were 11.5 ± 1.9 and 3.9 ± 4.0 days and 38.2 ± 8.3 and 60.8 ± 12.1 days, respectively, both with significant differences.
Conclusion
A four-claw titanium plate is valuable for patients with multiple rib fractures, allowing easy fixation of broken ribs beneath the scapula, even the second rib.
Keywords
Introduction
Blunt chest trauma combined with multiple rib fractures often causes thoracic collapse and hemopneumothorax. Severe chest pain always limits respiratory effort, causing dyspnea. This is exacerbated in patients with flail chest, which can cause respiratory failure. Ventilator support is the first-choice treatment for patients with respiratory failure. Prolonged mechanical ventilation increases the incidence of pulmonary complications such as empyema, ventilator-associated pneumonia, or barotrauma. A new treatment method is necessary to shorten the time of mechanical ventilation, shorten the intensive care unit (ICU) length of stay, and decrease the mortality rate of patients with respiratory failure caused by multiple rib fractures.
Surgical fixation for rib fractures is currently an accepted therapy. Although the absolute indications for rib fixation remain controversial, it is well accepted that rib fracture fixation is necessary for patients with obvious chest deformity, flail chest, and multiple displaced rib fractures with overlapping ends. 1 Because postoperative analgesia can effectively relieve the pain caused by rib fractures, whether pain scores can be used as indicators in patients with rib fracture remains controversial. Surgical fixation has been suggested to shorten the duration of mechanical ventilation and ICU stay, improve respiratory function, and decrease the pain score.2–4 Internal fixation devices that have been used include the 90° drill and screwdriver, the STRATOS System (MedXpert GmbH, Heitersheim, Germany), titanium bars and clips, osteosynthesis plates, intramedullary rib splints, and others. These devices have been suggested to improve the prognosis of patients with multiple rib fractures.5–8 Because the ribs are not all of the same shape, each fixation instrument has its restriction. Four-claw titanium plates were introduced in our hospital in 2012. They are thinner and shorter than other internal fixation instruments being applied. We herein present our experience of surgical stabilization of multiple rib fractures using four-claw titanium plates.
Patients and methods
Patients
Patients who were treated for multiple rib fractures in our hospital from January 2012 to January 2016 were included in this retrospective study. The study protocol was approved by the ethics committee of our hospital, and written informed consent was received from each patient. All patients underwent chest computed tomography and three-dimensional rib reconstruction on the first day of presentation to our emergency department. All patients had flail chest and severe chest wall deformities. Patients with respiratory failure received mechanical ventilator support. Patients who needed emergency thoracotomy, had good chest stability, or had no thoracic collapse were excluded from the study.
The patients were divided into a surgery group and control group. Patients in the surgery group underwent rib fixation with a four-claw titanium plate on the second or third day if they were hemodynamically stable. Patients in the control group received only conservative therapy (mainly pain relief, chest bandage fixation, oxygen inhalation, sputum induction, or mechanical ventilator support).
Surgical technique
The four-claw titanium plate used in the present study was 3.5 cm long and 1.9 cm wide (Figure 1). It had two claws at each end. The stress of a four-claw titanium plate is twice that of the ribs according to finite element modeling and analysis. 9 The four-claw titanium plate can be shaped to match the shape of the ribs using special pliers, and different special pliers can be selected according to the different positions of rib fractures.

Four-claw titanium plate
Patients in the surgery group underwent general anesthesia and double-lumen tracheal intubation. The patients were placed in the lateral position. The upper limb of the injured side was raised. A 30° endoscope was inserted into the thoracic cavity from the midline of the seventh intercostal space to detect pleural hemorrhage, possible lung damage, and the position of the fractured ribs. An incision was made above the rib fracture sites. If the broken ribs were beneath the scapula, the incision was made at the lower margin of the scapula. Because the second rib beneath the scapula was difficult to expose, two retractors were usually used in surgery. By adjusting the position of the two retractors, it was easier to expose the second broken rib. The serratus anterior and latissimus dorsi were cut to expose the rib fracture site. The rib fractures were reset in the anatomic position with forceps. The four-claw titanium plate was pressed with special pliers according to the shape of the ribs, placed at the broken end of the ribs, and locked with pliers (Figures 2–4). A chest tube was placed in the chest cavity from a video-assisted thoracic surgery (VATS) observation hole.

Rib fracture before and after the operation. (a, b) Broken rib before the operation. (c, d) Satisfactory reconstruction of the fracture
(a) Broken rib. (b) The broken rib was reset in the anatomic position. (c) The four-claw titanium plate was used to cover the broken end of the rib and was then locked with pliers. (d) Satisfactory reconstruction of the fracture

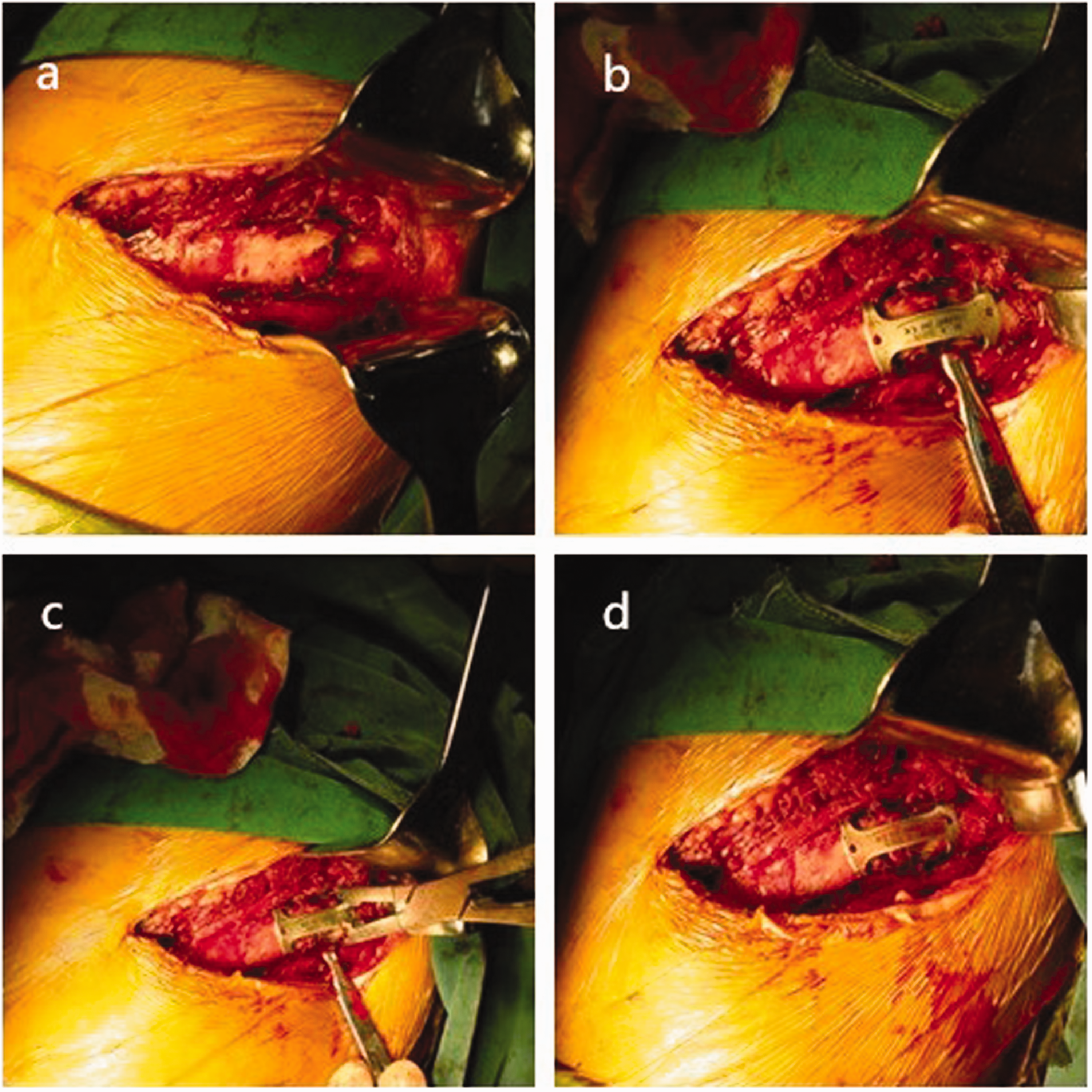
(a) A broken rib under the scapula was exposed by two retractors and fixed with a four-claw titanium plate using special pliers. (b) Satisfactory reconstruction of the fracture
Statistical analysis
The patients’ age, sex, cause of fracture, Injury Severity Score, chest Abbreviated Injury Scale score, number of ventilator days, length of ICU stay, and length of hospitalization were recorded.
All statistical analyses were performed using the SPSS 22.0 software package (IBM Corp., Armonk, NY, USA). The data regarding the patients’ characteristics are expressed as mean ± standard deviation. Pearson’s χ2 test was performed for comparison of categorical variables, and Fisher’s exact test was performed for comparison of quantitative data. A P value of <0.05 was considered statistically significant.
Results
This retrospective study involved 54 patients (surgery group, n = 27; control group, n = 27). There were no significant differences in age or sex between the groups. The mechanisms of rib fracture in the surgery and control groups were traffic accidents (n = 19 and 18, respectively), falls from a height (n = 6 and 8, respectively), and heavy weight extrusion (n = 2 and 1, respectively). The complications in the surgery and control groups were brain trauma (n = 2 and 3, respectively), abdominal injury (n = 4 and 3, respectively), spine fracture (n = 3 and 4, respectively), limb fracture (n = 5 and 7, respectively), and pulmonary contusions (n = 27 for both groups). There were no significant differences in any of these injury mechanisms or complications between the two groups. The number of fractured ribs, the chest Abbreviated Injury Scale score, and the Injury Severity Score were higher in the surgery group than in the control group, but the difference was not statistically significant. Seventeen patients in each group required mechanical ventilation upon admission to our hospital. The duration of mechanical ventilation of patients with flail chest was 4.5 ± 0.7 and 7.9 ± 1.7 days in the surgery and control group, respectively (P < 0.01). The length of ICU stay in patients with flail chest was much shorter in the surgery group than in the control group (5.9 ± 0.6 and 10.6 ± 1.9 days, respectively; P < 0.01). The length of hospitalization was 11.5 ± 1.9 and 13.9 ± 4.0 days in the surgery and control group, respectively (P<0.01) (Table 1). The recovery time to regular life was much shorter in the surgery group than in the control group (38.2 ± 8.3 and 60.8 ± 12.1 days, respectively; P < 0.01). The median follow-up in the two groups was 1 year. There was no mortality in either group. Six patients in the surgery group sustained a second broken rib beneath the scapula. No steel plate rupture or dislocation occurred during follow-up.
Data of the surgery group and control group

Data are presented as n or mean ± standard deviation.
AIS, Abbreviated Injury Scale; ICU, intensive care unit
Discussion
Rib fractures often induce persistent and severe pain. Multiple rib fractures can cause collapse and deformity of the chest wall. Multiple fractures of multiple ribs can even cause flail chest, which can greatly increase the risk of mortality. Rib fixation is a new method that has become more widely accepted in recent years. Current research suggests that compared with conservative treatment, rib fixation can remarkably relieve the patient’s chest pain, shorten the duration of mechanical ventilation and hospitalization, reduce the incidence of pneumonia, and decrease the mortality rate of patients with flail chest.10–12 Even in patients with isolated, multiple distracted and painful non-flail rib fractures, surgical stabilization has been shown to be safe and effective in alleviating postoperative pain and improving patient recovery. 13 However, this is still controversial. A study by Farquhar et al. 14 showed that the nonsurgically managed group had significantly better outcomes than the surgical group in terms of ventilator days, length of stay in the ICU, total hospitalization duration, and incidence of pneumonia. There were no significant differences in long-term outcomes, such as chest pain or dyspnea. 14 Our research suggests that rib fixation can shorten the ICU length of stay and duration of ventilation in patients with flail chest. In all patients, rib fixation can significantly shorten the length of hospitalization and recovery time to regular life, suggesting that rib fixation is beneficial for patients with flail chest or chest wall deformity.
Many kinds of internal fixation instruments are available for rib fractures. Although each can firmly fix the broken ribs, they have some limitations. For example, if titanium elastic nails and Synthes MatrixRIB outer cortical plates (DePuy Synthes, Warsaw, IN, USA) are used to fix a broken rib, a hole must first be created on the outer cortex of the fractured rib. Because the two materials are fixed in the bone marrow cavity, the bone marrow cavity sustains inevitable damage.15,16 Some plates are fixed with screws, which may be time-consuming and laborious. For these plates, more dissociation of the muscles around the ribs is needed, which increases the damage to local tissue and extends the operation time.5,6,17–20 Several kinds of claw-type titanium plates can be used. The number of claws ranges from 8 to 18.21,22 We found that a higher number of claws is associated with a greater titanium plate length, resulting in increased dissociation of the muscles around the fractured ribs. The four-claw titanium plate was invented in 2012 by a doctor in our department. The number of claws of the titanium plate was decreased to four to reduce the damage to the muscle around the rib. Reducing muscle dissociation can also shorten the operation time. The distance between the two longitudinal claws is 35 mm, which is long enough to cross most of the two broken ends of the fracture. The stress of the four-claw titanium plate is twice that of the ribs, providing ample stability for the fractured ribs. No patients in the present study had developed loosening or unreliable fixation of the four-claw titanium plates at 3 to 6 months postoperatively, indicating that four-claw titanium plates are safe and efficient.
VATS was first introduced for diagnosis and therapy in patients with chest trauma in 1990.23–25 It is now used in surgery for patients with rib fractures.15,25 In the present study, all patients in the surgery group initially underwent VATS to detect intrapleural injury and accurately locate the position of the rib fracture, thus facilitating accurate surgical incision.
Severe trauma often leads to fractures of the second and third ribs. Fractured ribs beneath the scapula, especially the second rib, are difficult to expose; thus, the highest rib that could be fixed in the current literature is the third rib. In our institution, the scapula is raised with two retractors if the broken ribs under the scapula have undergone fixation. The second broken rib can be exposed by adjusting the position of the two retractors. Because the four-claw titanium plate is shorter than other clawed titanium plates, it requires less muscle dissociation, which decreases the difficulty of the second rib fixation. Using special pliers in the present study, it was not very difficult to fix the broken second rib. Our patients with second rib fixation experienced obvious relief of chest pain after the operation without the need for continuous and intense intercostal anesthesia. Therefore, the four-claw titanium plate is an accepted internal fixation instrument for a second broken rib beneath the scapula.
Conclusion
The four-claw titanium plate is a convenient and effective internal fixation instrument for rib fractures. It allows for easy fixation of broken ribs beneath the scapula, even the second rib.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by a grant from the Medical Guiding Fund of the Science and Technology Commission of Shanghai Municipality (134119b2400).