
Abstract
Objective
To evaluate the relationship between the preoperative imaging differences and prognosis in patients with cervical spondylosis with cervical vertigo who underwent total disc replacement (TDR).
Methods
This was a retrospective study of patients with cervical spondylosis with cervical vertigo treated with single-segment TDR. The severity of pre- and postoperative cervical vertigo was evaluated separately. Paired samples t-tests were used to compare the severity of the symptoms before and after surgery. Characteristics of plain films, computed tomography myelography and magnetic resonance imaging were compared between patients with different outcomes by analysis of variance and Fisher’s exact tests.
Results
The severity of cervical vertigo was significantly different after single-segment TDR. Three groups with different treatment outcomes were not significantly different with regard to gender, age, type of the cervical spondylosis, follow-up time, segment of surgery, cervical curve, range of motion, T2WI high signal in the spinal cord, and location of compression. The type of compression was significantly different between the three groups.
Conclusions
Cervical vertigo was improved in patients with cervical spondylosis through the TDR procedure. Those in whom a herniated disc was the main source of compression may have a better prognosis following TDR.
Keywords
Vertigo is caused by various diseases and is associated with various systems. Patients with vestibular, visual, neurovascular, and cervico-proprioceptive disorders can all present with vertigo.1,2 Regarding vertigo originating from the cervical spine, vascular compression, altered proprioceptive input, and vasomotor changes caused by irritation of the cervical sympathetic chain are the three mechanisms widely accepted to date. 3 In 1926, Barre and Liéou noticed that cervical spondylosis may play a role in alternating the blood flow of the vertebral artery. The resultant cervical pain, vertigo, headache, dizziness, vomiting, and blurry vision are thus called Barré–Liéou syndrome, and has been referred to as cervical vertigo. 4 However, recent studies revealed that the clinical symptoms of vertigo are actually not directly correlated with ischemia of the vertebral artery. Bilateral vertebral artery obstruction would not lead to an ischemic lesion of the corresponding area. 5 Therefore, vertebral artery deficiency cannot solely explain the mechanism of cervical vertigo, and thus the etiology of cervical vertigo remains controversial. In clinical practice, it seems that trauma, degeneration, inflammation, and neoplasia of the cervical spine all can present with cervical vertigo. Endo et al. 6 confirmed that traumatic changes to the cervical spinal cord such as whiplash injury could induce cervical vertigo and lead to posture sway. Our previous research suggested that anterior cervical discectomy and fusion in patients with cervical spondylosis could alleviate cervical vertigo and other sympathetic symptoms. 7 Compared with anterior cervical discectomy and fusion, cervical total disc replacement (TDR) has a significantly better outcome in one-level disc disease with respect to symptom relief and maintenance of function.8,9
In clinical practice, we found that some patients also get relief from vertigo as well as cervical spondylopathy after TDR. Although cervical TDR seems to be a promising method for the treatment of patients with single-level cervical spondylosis, no literature has addressed the effectiveness of cervical TDR with respect to alleviating cervical vertigo. This 3-year follow-up study was carried out to determine whether cervical vertigo can be improved after single-segment cervical TDR in patients with cervical spondylosis and whether the prognosis can be predicted by preoperative plain films, computed tomography (CT) myelography, and magnetic resonance imaging (MRI).
Materials and Methods
This was a retrospective study of patients who were diagnosed with cervical spondylosis between March 2010 and July 2013 and treated with single-segment TDR. Thirty-one of these patients reported preoperative vertigo. All data were collected by the authors of this manuscript. There were three follow-up points: prior to surgery, immediately after surgery, and final follow-up before we prepared to write this article. The exclusion criteria were as follows: (1) otolaryngologic and neurovascular diseases were diagnosed before cervical surgery; (2) psychological disorders were diagnosed before cervical surgery. None of the 31 patients were excluded.
All of the surgical procedures were performed at Beijing Jishuitan Hospital. Single-segment cervical TDR was performed strictly according to the standard Smith–Robinson approach. 10 After decompression, the artificial disc was inserted. The Bryan™ disc (Medtronic, Minneapolis, Minnesota, USA) was used in all patients. The severity of preoperative, immediate postoperative, and postoperative vertigo (final follow-up) was evaluated separately based on a visual analog scale (VAS) from 0 to 10. Paired sample t-tests were used to compare the severity of the symptoms before and after surgery.
Plane films, CT myelography, and MRI were evaluated preoperatively and postoperatively. The cervical curvature was divided into two categories on lateral view radiographs: lordotic, straight, and kyphotic. The range of motion was calculated by the hyperextension Cobb angle minus the hyperflexion Cobb angle of the operated segment. The compression type was divided into two categories determined by the CT myelography in the sagittal plane and T2WI of the MRI in the sagittal plane (Figure 1): herniated disc as the chief cause of compression (Type A), osteophyte as the chief cause of compression (Type B). The T2WI high signal in the spinal cord was determined by MRI in the sagittal plane. The location of the compression was divided into four categories in the axial plane MRI (Figure 2): no significant impression with the anterior border of the spinal cord flattened (Type A), central impression with symmetry (Type B), central–lateral impression with penetration of the midline (Type C), and lateral impression without penetration of the midline (Type D).
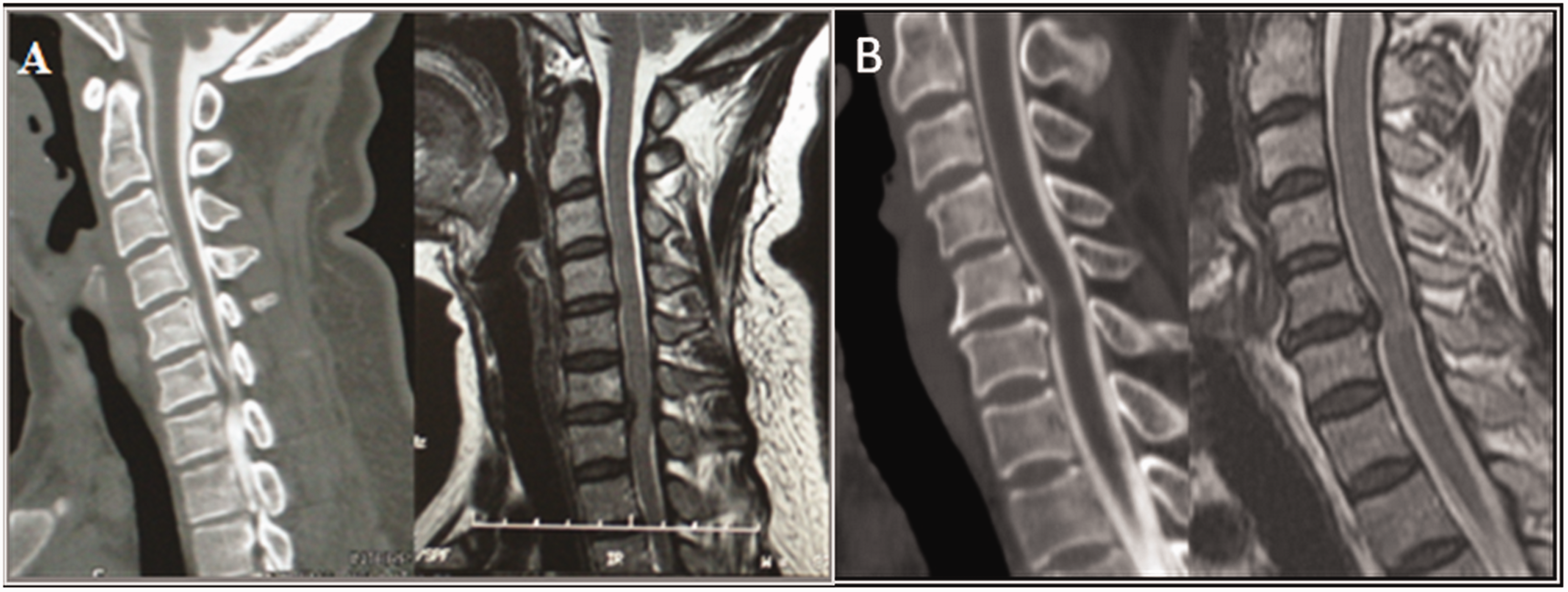
Categories of compression type. The vertical distance to the posterior border of the vertebral body from the furthest part of the herniated disc minus that from the furthest part of the osteophytes of the same segment is positive defined as herniated disc as the chief cause of compression (Figure 1a, type A). The opposite condition is defined as an osteophyte being the chief cause of compression (Figure 1b, type B).

Categories of location of compression. Type A: no significant impression with the anterior border of the spinal cord flattened. Type B: central impression with symmetry. Type C: central-lateral impression with midline penetration. Type D: lateral impression without midline penetration.
Then, according to the recovery rate (RR) of cervical vertigo [(preoperative scores–postoperative scores (latest follow-up))/preoperative scores] (Table 1), these patients were divided into a deteriorative group (RR < 0), a partially improved group (0 < RR < 1), and a completely improved group (RR = 1). Consecutive data for age, follow-up time, and range of motion were analyzed by analysis of variance (ANOVA), and categorical variable data for sex ratio, type of cervical spondylosis, operated segment, physical curve, compression type, T2WI high signal in the spinal cord, and location of the compression were analyzed by the Fisher’s exact test.
The preoperative scores, postoperative scores (latest follow-up), and recovery rate of each patient. In type of compression, A stands for herniated disc as the chief cause of compression, and B stands for osteophyte as the chief cause of compression. In the location of compression, A stands for no significant impression with the anterior border of the spinal cord flattened, and B stands for central impression with symmetry, C stands for central-lateral impression with midline penetration, and D stands for lateral impression without midline penetration.

Results
There were 16 men and 15 women with cervical vertigo who had an average age of 48.8 years (range, 31 to 71). Seventeen of those patients were diagnosed with myelopathy, 4 with radiculopathy, and 10 with mixed cervical spondylosis. Two patients were operated on in the C3/4 segment, 5 patients in the C4/5 segment, 19 patients in the C5/6 segment, and 5 patients in the C6/7 segment. Among these patients, 22 (71.0%) were followed for more than 12 months after surgery, and the average follow-up time was 34 months. These patients had main complaints of myelopathy, radiculopathy, and mixed-type cervical spondylosis, which were accompanying symptoms to cervical vertigo that bothered them greatly. Most of these patients were either under the care of a neurologist or otolaryngologist without the disease being identified, or had attempted treatment by a neurologist or otolaryngologist without symptomatic improvement.
The severity of vertigo in these patients with cervical spondylosis was significantly different before and after single-segment TDR (p < 0.01).
According to the recovery rate (RR), there were 3 patients in the deteriorative group (RR < 0), 15 patients in the partially improved group (0 < RR < 1), and 13 patients in the completely improved group (RR = 1). Most patients improved immediately after surgery. There was no significant difference between the latest follow-up and immediately after surgery. Only one patient had recurrence 2 years later, with complete resolution of symptoms of vertigo immediately after surgery. However, in this patient, the vertigo symptoms are now less severe than preoperative symptoms.
Results are shown in Table 2.
Summary of study results.
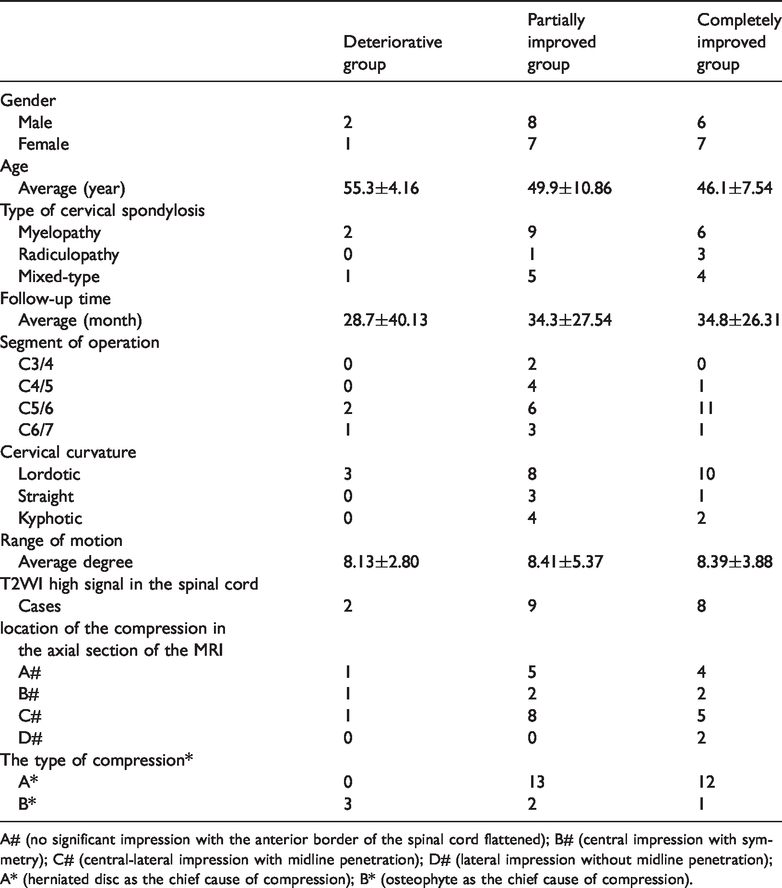
A# (no significant impression with the anterior border of the spinal cord flattened); B# (central impression with symmetry); C# (central-lateral impression with midline penetration); D# (lateral impression without midline penetration); A* (herniated disc as the chief cause of compression); B* (osteophyte as the chief cause of compression).
According to ANOVA and Fisher’s exact tests, these three groups had no significant difference concerning gender, age, type of cervical spondylosis, follow-up time, and segment of operation (p > 0.05). There were also no significant differences between cervical curvature, range of motion, T2WI high signal in the spinal cord, and location of the compression in the axial section of the MRI (p > 0.05). However, the type of compression was significantly different between the three groups (p = 0.004). When comparing the three groups, there was a significant difference between the deteriorative group and the partially improved group (p = 0.012) and between the deteriorative group and the completely improved group (p = 0.007). There were no significant differences between the partially improved group and the completely improved group (p > 0.05).
Discussion
It has been proposed that asymmetric sensory input from the cervical region can lead to cervical vertigo. 1 This suggests that the location of the compression may be related to symptoms of cervical vertigo. However, according to the results of this retrospective study, the location of the compression may not be a risk factor for cervical vertigo and has no influence on the outcome of surgical treatment.
The average range of motion was normal in each group without a significant difference between groups. This also demonstrated that the right surgical decision was made. The high signal on T2WI MRI usually implies a spinal cord lesion, which had no significance on the outcome of cervical vertigo or on the cervical curvature. However, the type of compression was significantly different in the completely improved group and the partially improved group compared with the deteriorative group. Furthermore, patients in whom the type of herniated disc was the main source of compression (Type A) seemed to have a better outcome after TDR compared with those in whom the type of osteophyte was the main cause of compression (Type B). This result raises the questions: what is the underlying difference behind these two patterns of compression? Is it because of the rigidity of the compression itself or different procedures performed on the patients?
By reviewing all of the operative records, we found that in patients in whom a herniated disc was the main source of compression (Type A), full decompression was performed with resection of the posterior longitudinal ligament (PLL). In patients where an osteophyte was the main source of compression (Type B), after removing the entire disc, we chose to preserve the PLL and remove bony spurs in front of the PLL, then used a probe to make sure that the decompression was sufficient.
There are considerations about whether to remove the PLL. In type A, a herniated disc might penetrate through the PLL and hide behind it or between the layers of the PLL, so resection of the PLL was effective for a full decompression. In Type B, the corresponding compression was due to an osteophyte, which can be safely removed without disturbing the integrity of the PLL, so we chose to treat type B by leaving the PLL intact. The principle we followed for whether we preserved or removed the PLL was as follows: all of the pathological tissues were removed as much as possible while preserving the healthy tissues to the greatest extent.
According to the literature, the PLL contains sensory nerves as well as sympathetic nerves. A dense sensory fiber network forming a single layer was found at the intervertebral disc region in the cervical PLL, whereas sympathetic fibers in this region were sparsely distributed. 11 It was also reported that there is nerve peptide Y (NPY) and calcitonin gene related peptide immunoreactive nerve fibers distributed in the lumbar intervertebral disc (IVD) and PLL, and this may be the pathogenesis of the lower back pain.12,13 This pattern of nerve fiber distribution may also exist in the cervical region, and this requires further investigation. During the procedure for TDR, removal of the PLL on the responsible segment might reduce the stimulation to the sympathetic fibers and sensory fibers in the intervertebral disc region and ultimately lead to remission of vertigo. However, in patients in whom an osteophyte was the main source of compression, the PLL was left intact and the sensory pathway may not have been blocked, and this may have been responsible for the poor improvement of cervical vertigo.
Based on the current study, we speculate that there are sensory fibers or sympathetic nerve fibers distributed in the PLL. Degeneration of the intervertebral disc or bony spurs may cause the lesion to these nerve fibers in the PLL, leading to cervical vertigo via a certain pathway, and so removal of the PLL may block the pathological lesion pathway to the PLL and help to eliminate cervical vertigo. In 2008, Cassaglia, Griffiths, and Walker showed that sympathetic nerve activity withdraws the blood flow while sympathectomy can increase it, and other experiments also confirmed this theory.14–16 Miyoshi also investigated sympathetic and parasympathetic changes produced by the stimulation of nerves around the proximal vertebral artery (the vertebral nerve) in a cat model, and found that pupillary changes, pulse, and blood pressure changes in cats. 17 This suggests that sympathetic excitation can produce a decrease in blood flow of the vertebral artery. Thus, the vertebrobasilar insufficiency symptoms such as cervical vertigo may also be caused by stimulating the sensory and sympathetic nerve fibers in the PLL. 18
Our study was a retrospective study, and the number of cases was limited, which may have influenced our results. Another group with a Type B compression pattern could be evaluated in which both the PLL and the bony compression are removed. If patients in this group were to also report satisfactory outcomes with alleviation of the cervical vertigo, the conclusion could be more convincing. Further pathological tests could also be performed to confirm the features of the sympathetic nerve fiber distribution. Prospective, randomized, controlled trials should be carried out in the future to evaluate the validity of this study.
Conclusions
Cervical vertigo was improved in patients with cervical spondylosis following the TDR procedure. Patients with cervical spondylosis in whom a herniated disc was the major cause of compression achieved a better treatment effect after TDR.
Footnotes
Acknowledgements
This study was funded by Beijing Municipal Health Commission (BMC2018-4).
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Written informed consent for publication was obtained from all patients.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
The study was approved by the institutional review board of Beijing Jishuitan Hospital. All of the patients gave written consent for the publication of their individual research data, provided that their identity cannot be revealed by those data.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.