
Abstract
Objective
This study was performed to determine the risk factors associated with peripherally inserted central catheter (PICC)-related venous thrombosis in patients of advanced age (>65 years).
Methods
In total, 549 hospitalized patients aged 66 to 104 years who were undergoing PICC placement from January 2008 to December 2014 were enrolled. Symptomatic venous thrombosis was confirmed by B-mode or Doppler ultrasonography in the presence of clinical signs. Logistic regression analysis was performed on the variables of interest to identify the risk factors for thrombosis. Odds ratios (ORs) with the corresponding 95% confidence intervals were generated.
Results
Of the 549 patients with PICC placement, 106 (19.3%) developed PICC-associated venous thrombosis, 84 cases of which were symptomatic. The logistic regression results revealed that PICC-related venous thrombosis was associated with a history of venous thrombosis (OR, 6.745 [3.237–14.056]), number of lumens (OR, 1.934 [1.362–2.572] and OR, 3.762 [1.672–5.932] for dual and triple lumens, respectively), and PICC gauge (OR, 1.821 [1.256–2.537] and OR, 3.864 [1.367–8.251] for 5-Fr and 6-Fr, respectively).
Conclusions
A history of thrombosis, high number of lumens, and large-gauge catheters were strong risk factors for patients aged >65 years undergoing PICC placement.
Keywords
Introduction
Peripherally inserted central catheter (PICC) placement is a central venous catheterization (CVC) method that utilizes an approach from a peripheral vein path (median cubital vein). Compared with CVC from the femoral vein, subclavian vein, or internal jugular vein, PICC placement provides several advantages such as less local injury, a lower risk of infection, easier nursing, a longer catheter retention time, and less influence on activities of daily living.1,2 Therefore, PICC placement has been widely used in patients undergoing fluid transfusions in combination with normal activities, periodic chemotherapy, or long-term parenteral nutrition support.3–5
Patients of advanced age are one of the main populations that undergo PICC placement. However, the benefits derived from this type of catheterization can be weakened by the development of complications such as vein thrombosis, which is associated with increases in the length of stay, costs, morbidity rate, and even mortality rate. One retrospective study demonstrated that patients aged >60 years are at higher risk of vein thrombosis (odds ratio [OR], 10.15; 95% confidence interval [CI], 8.14–14.52). 6 However, the risk factors for thrombosis in older patients remain unclear because very few studies have focused on this issue. 7 Therefore, it is of great clinical value to analyze the risk factors associated with PICC-related venous thrombosis in patients of advanced age. In our previous study, we investigated the risk factors associated with CVC-related venous thrombosis in older men. 8 In the present study, we investigated useful predictors and risk factors for PICC-related thrombosis in patients of advanced age (>65 years).
Methods
Study population
Hospitalized patients of advanced age who were undergoing PICC placement in the Department of Geriatrics of the Chinese PLA General Hospital, Beijing, China from January 2008 to December 2014 were enrolled in the present study. This study followed the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Chinese PLA General Hospital (PLAGH-A2007171). Written informed consent was collected from all enrolled patients.
Data collection
The following details were collected from each patient: history of type 2 diabetes, chronic heart failure, malignancy, cerebral infarction, history of venous thrombosis, bedridden condition during catheterization, use of special medication (such as aspirin, clopidogrel, or erythropoietin), chemotherapy, and antibiotics used during catheterization. The catheters were composed of silicone material (Groshong; Bard Access Systems, Salt Lake City, UT, USA), and ultrasound guidance was used for all PICC operations. For diagnosis of symptomatic PICC-related venous thrombosis, B-mode or Doppler ultrasound was used in the presence of clinical signs when a PICC was located in situ. For diagnosis of asymptomatic PICC-related venous thrombosis, monthly regular color Doppler ultrasonographic examinations were performed to observe the thrombus.
Statistical analysis
The data are presented as number and percentage (%). The chi-square test or t test was performed to examine the differences in the various risk factors between patients with and without thrombosis. Logistic regression analysis was performed on variables of interest to identify the risk factors for thrombosis. A P value of <0.05 was considered statistically significant. All statistical analyses were performed using SPSS 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Patients’ general characteristics
We encountered 549 patients who had undergone PICC placement during our observation period. The patients’ age ranged from 65 to 104 years (mean age, 86.2 ± 7.2 years). Most patients in our study were male (92.9%), and their average body mass index was 23.0 kg/m2. Almost half of the patients had a diagnosis of type 2 diabetes (48.3%, n = 265), cancer (43.7%, n = 240), cerebral infarction (43.4%, n = 238), or chronic heart failure (36.8%, n = 202). About 6.6% (n = 36) of patients had a history of venous thrombosis. The common indications for PICCs were antibiotic administration (74.3%, n = 408), total parenteral nutrition (59.9%, n = 329), and chemotherapy (17.1%, n = 94). Approximately 19.3% (n = 106) of patients had evidence of documented vein thrombosis as diagnosed by B-mode or Doppler ultrasound. About 20.7% (22 in 106) of the cases of venous thrombosis were asymptomatic. The mean time to thrombosis was about 58.2 ± 28.5 days.
Catheter-related factors were also assessed. More than one-fourth of the 549 patients (25.5%, n = 140) underwent adjustment during catheter insertion. The average number of insertion attempts and adjustments during insertion was 1.28 and 0.27, respectively. About 50.3% (n = 276) and 41.5% (n = 228) of the PICCs were single-lumen and dual-lumen catheters, respectively. The two most common catheter sizes were 4 and 5 Fr, which accounted for 41.9% (n = 230) and 44.6% (n = 245) of the total PICCs, respectively. The PICCs were most commonly placed in the basilic vein (69.6%, n = 382) and in the right arm (67.6%, n = 371). The mean duration of PICC use was 108.6 ± 112.4 days.
Table 1 presents the detailed clinical characteristics of patients with and without thrombosis. The two groups were relatively similar in age, the proportion of male subjects, and the average body mass index. Additionally, the incidences of several common baseline diseases were similar between the two groups. Among the 106 patients with thrombosis, the incidences of type 2 diabetes, chronic heart failure, cancer, cerebral infarction, and a bedridden condition were 44.3% (n = 47), 33.0% (n = 35), 48.1% (n = 51), 44.3% (n = 47), and 25.0% (n = 39), respectively. Among the 443 patients without thrombosis, the incidences of these diseases were 49.2% (n = 218), 37.7% (n = 167), 42.7% (n = 189), 43.1% (n = 191), and 4.9% (n = 134), respectively. No significant differences in the incidences of these baseline diseases were observed between the patients with and without thrombosis. Interestingly, a history of venous thrombosis differed significantly between patients with and without thrombosis (P < 0.05). Of the 106 patients with thrombosis, 19.8% (21/106) had a history of venous thrombosis. However, only 3.4% (15/443) of those without thrombosis had previously experienced venous thrombosis.
Demographics of patients who underwent peripherally inserted central catheter placement.
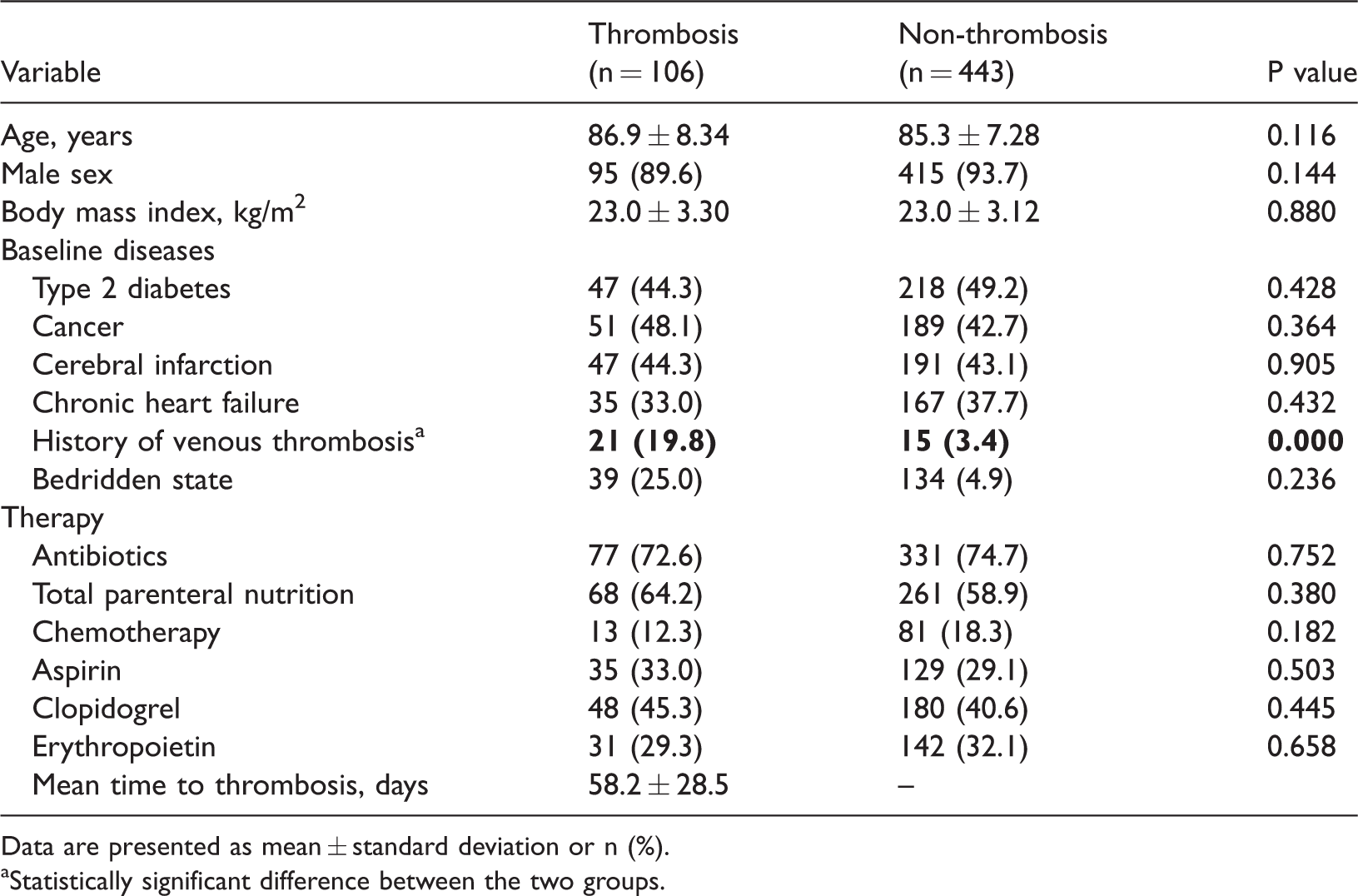
Data are presented as mean ± standard deviation or n (%).
aStatistically significant difference between the two groups.
Next, we compared the catheter-related factors between patients with and without thrombosis. As shown in Table 2, the two groups had a similar mean duration of PICC use (124.2 vs. 105.6 days, respectively). In addition, no significant difference was observed in the number of insertion attempts, percentage of adjustments during insertion, or number of adjustments. Interestingly, significant differences of the number of lumens were observed between the patients with and without thrombosis (P < 0.05). The incidence of single-, dual- and triple-lumen catheters used in patients with thrombosis was 21.7%, 63.2%, and 15.1%, respectively. However, the incidence of these three types of catheters in patients without thrombosis was 57.1%, 36.3%, and 6.6%, respectively. The catheter size was also significantly different between the two groups (P < 0.05). Among patients with thrombosis, the percentages of patients in whom the basilic, brachial, and cephalic vein was used for PICC insertion were 68.9%, 18.9%, and 11.3%, respectively, which were not significantly different from those in patients without thrombosis (Table 2). The proportion of patients in whom the right arm was used for insertion was also similar between the two groups.
Catheter-related factors in patients undergoing peripherally inserted central catheter placement.

Data are presented as mean ± standard deviation or n (%). PICC, peripherally inserted central catheter.
Risk factors for PICC-related venous thrombosis
The logistic regression of patient factors revealed that PICC-related venous thrombosis was associated with a history of venous thrombosis (OR, 6.745 [95% CI, 3.237–14.056], P = 0.000) (Table 3). However, we found no association between PICC-related venous thrombosis and risk factors that have been previously reported, including a bedridden state (OR, 1.167 [95% CI, 0.613–2.223]), total parenteral nutrition (OR, 1.401 [95% CI, 0.793–2.477]), cancer (OR, 1.631 [95% CI, 0.886–3.005]), chemotherapeutics (OR, 0.497 [95% CI, 0.200–1.234]), and the use of antibiotics (OR, 1.452 [95% CI, 0.470–4.481]). With respect to catheter-related characteristics, only the number of lumens (OR, 1.934 [95% CI, 1.362–2.572] and OR, 3.762 [95% CI, 1.672–5.932] for double- and triple-lumen PICCs; P = 0.020 and 0.001, respectively) and the PICC gauge (OR, 1.821 [95% CI, 1.256–2.537] and OR, 3.864 [95% CI, 1.367–8.251] for 5-Fr and 6-Fr PICCs; P = 0.031 and 0.010, respectively) were associated with PICC-related venous thrombosis. The other catheter-related characteristics, including the number of insertion attempts, adjustments during insertion, and sites of insertion, were not associated with PICC-related venous thrombosis.
Logistic regression analysis of risk factors associated with thrombosis in patients with peripherally inserted central catheters.

Discussion
The incidence rates of PICC-related venous thrombosis differ considerably among previous studies. The two highest incidence rates that have been reported are 75.0% 9 and 51.4%. 10 In contrast, Bonizzoli et al. 11 reported that the rate of PICC-related venous thrombosis in post-critical patients was approximately 27.2%, and the results from a study by Wilson et al. 12 indicated a rate as low as 8.4% (36 of 431 cases). Other studies have shown incidence rates of 5.2% in patients with lung cancer 13 and 1.4% in patients with breast cancer. 14 Nevertheless, in the present study, the incidence of PICC-related venous thrombosis was approximately 19.3% in patients of advanced age. The distinct variability in the reported incidences may have resulted from differences in the selection of patients and differences in the type of venous thrombosis examined in these studies. These data also indicate that the occurrence of PICC-related venous thrombosis is affected by multiple factors.
The incidence of thrombosis in our study was approximately 19.3%. One explanation for the observed incidence is the introduction of asymptomatic thrombosis, which accounted for 20.7% of the total thrombosis events in our study. The insurance of patients in our department covered the monthly color Doppler ultrasound examination. Thus, we had a better opportunity to discover the thrombosis before symptoms appeared, resulting in a high rate of observation of the incidence of thrombosis. Another possible explanation is that to our knowledge, our study population is the oldest (85.5 ± 7.2 years) to be examined in the literature to date. An age of >60 years has been identified as a risk factor for thrombosis in patients undergoing PICC therapy; 15 thus, all patients in our study had at least one risk factor for catheterization-related thrombosis. However, no significant association between age and venous thrombosis was observed in our cohort, suggesting that the risk of venous thrombosis does not increase with age in patients older than 65 years.
Interestingly, we found that a history of venous thrombosis was a very strong risk factor for PICC-related venous thrombosis (OR, 6.745 [95% CI, 3.237–14.056]). This finding is consistent with those based on hospitalized patients who have undergone PICC placement 16 and with findings from patients in neurological intensive care units. 12 These results increase the importance of laboratory tests of coagulation function. Several coagulation fibrinolysis factors, such as the activated partial thromboplastin time, fibrinogen level, and mean activity of factor VIII, have been considered to be associated with catheter-related venous thrombosis.17,18 Thus, greater efforts are needed to clarify the mechanism of the contribution of a history of thrombosis to the occurrence of PICC-related venous thrombosis. Moreover, careful attention should be given to older patients with a history of thrombosis.
We also found that the risk of PICC-related thrombosis was associated with the number of lumens and the diameter of catheters, which is in accordance with previous studies.19–21 The mechanical explanation for catheter-related risk could be that larger PICC devices more readily cause endothelial damage, vascular reactivity, and up-regulated coagulation. A survey of laboratory coagulation markers could provide more evidence for this hypothesis. These findings suggest that a single-lumen, 4-Fr PICC could be optimal for older patients. However, older patients usually require long-term placement of catheters with multiple lumens for total parenteral nutrition, chemotherapy, blood collection, and other purposes. Thus, other approaches (e.g., midlines, tunneled catheters, and infusion ports) can also be applied in accordance with the INS Standards of Practice to reduce the incidence of thrombosis in older patients undergoing PICC placement.
Our previous studies showed a low incidence of CVC-related venous thrombosis in a similar cohort of older patients (6.17%), 8 which is only one-third the incidence of PICC-related venous thrombosis. This result is consistent with those from other related studies.11,22 Compared with CVC, PICC placement usually involves smaller-diameter catheters, and the catheterization distance is longer. In addition, a PICC is more likely to move in the upper limb than the catheter used in CVC. Therefore, the incidence of PICC-related venous thrombosis is higher than that of CVC-related venous thrombosis. The risks associated with PICCs are higher than those associated with CVC; however, because of the ease of insertion and perceptions surrounding PICCs, the potential complications of both PICC placement and CVC should be considered when selecting the method of catheterization, especially for patients of advanced age.
Unexpectedly, many accepted risk factors such as malignancy, diabetes, vascular conditions, and a high number of insertions were not found to be associated with PICC-related venous thrombosis in our study. The reasons for this could be related to the following limitations of our study. First, our study population was only from the geriatric department of a single hospital, resulting in a limited sample size and selection bias. Notably, most (>90%) patients in our study were male. Second, information regarding the covariates of interest was limited because of the retrospective design of our study. Third, the risk factors for symptomatic and asymptomatic thrombosis were not analyzed separately for the limited number of patients with asymptomatic thrombosis in our study.
Conclusion
Despite these limitations, our study provides evidence that a history of thrombosis, large number of lumens, and larger catheter size are strong risk factors for older patients (age of >65 years) undergoing PICC placement. In terms of clinical practice, doctors should be aware of these risk factors in older patients, and special attention should be focused on patients with a history of venous thrombosis. In addition, a PICC with a single lumen and small gauge could be optimal for patients of advanced age.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Footnotes
Funding
The work was supported by PLA General Hospital clinical research support projects (No. 2015FC-TSYS-2014).