
Abstract
Objective
To evaluate risk factors for venous thrombosis in patients undergoing chemotherapy via peripherally inserted central catheter (PICC).
Methods
Data regarding age, sex, body mass index (BMI), smoking history, diagnosis, medical history, family history of thrombosis, haemoglobin level, and white blood cell (WBC) and platelet counts were prospectively collected from consecutively recruited patients. Patients were evaluated using six thrombotic risk-assessment scales prior to PICC. Assessments of the general venous system and the catheterized vein and limb were made. Deep vein thrombosis (DVT) was diagnosed by colour Doppler ultrasonography. Thrombosis risk factors were identified by logistic regression analysis.
Results
Thrombosis occurred in 12/188 patients (6.38%). Age >60 years, BMI >25 kg/m2 and WBC >11.4 × 109/l were identified as independent risk factors for thrombosis. The incidence of thrombosis was 16.6% (12/72) in patients with one or more risk factors, and 55.5% (five of nine) in those with two or more risk factors.
Conclusions
Age >60 years, BMI >25 kg/m2 and WBC >1.4 × 109/l are major risk factors for thrombosis in Chinese patients undergoing PICC chemotherapy.
Introduction
The incidence of venous thromboembolism (including pulmonary thromboembolism and/or deep vein thrombosis [DVT]) in people with cancer is growing.1–3 Patients with malignant tumours have an eightfold higher risk of venous thrombosis than patients without tumours, 4 and this risk is especially great during infection, antineoplastic therapy and the perioperative period. 5 Peripherally inserted central catheters (PICC) also increase the risk of thrombosis, since their length and large diameter (relative to peripheral vein diameter) can lead to blood backflow during long-term catheterization.6,7 Prophylactic anticoagulation therapy should be tailored to individual patient risk profiles, 8 but studies of thrombotic risk factors have generally been limited to those undergoing plastic, orthopaedic, vascular or trauma surgery and are mostly retrospective. A prospective study of the risk of thrombosis in outpatients undergoing chemotherapy presented a simple assessment scale for risk of thrombosis, but investigated central venous catheters and subjects of multiple ethnicities. 9 Body mass index (BMI) >35 kg/m2 was identified as a thrombotic risk factor, 9 but this BMI is rare in Asian populations (including Chinese, Indian, Japanese and Korean subjects). 10 The aim of the present prospective study, therefore, was to determine thrombotic risk factors in Chinese patients undergoing chemotherapy via PICC.
Patients and methods
Study population
The study prospectively recruited all consecutive patients undergoing PICC chemotherapy in the Department of Surgical Oncology, Second Affiliated Hospital of Zhejiang University, Hangzhou, China, between December 2010 and August 2011. The study was approved by the Institutional Ethics Committee of Second Affiliated Hospital of Zhejiang University. All patients provided written informed consent prior to enrolment.
Assessment scales
Patients were evaluated using six thrombotic risk assessment scales prior to PICC: chemotherapy-associated venous thromboembolism (VTE); 9 Davidson–Caprini Risk-Assessment Model;11,12 Wells et al.; 13 Yale et al.; 14 Mommertz et al.; 15 and Caprini. 16 Data including age, sex, BMI, disease category, haemoglobin (Hb) level, platelet count, white blood cell (WBC) count, fasting blood sugar, medical history (including thrombus, other relevant diseases, smoking, diarrhoea 17 and family history of thrombus) were collected from each patient. Assessments also included the condition of the general venous system (varicose veins or venous pain) and sites of catheterized vein and catheterized limb. DVT was diagnosed by colour Doppler ultrasonography (sensitivity 97–100% and specificity 98–99% for detecting proximal thrombus18,19).
Statistical analyses
Data were presented as n (%). Univariate χ2 analysis was performed, with thrombosis as the dependent variable and various risk factors as independent variables. Logistic regression analysis was performed on statistically significant variables to identify the major risk factors for thrombosis. All statistical analyses were performed using SPSS® version 16.0 (SPSS Inc., Chicago, IL, USA) for Windows®, with P-value <0.05 considered as being statistically significant.
Results
The study included 188 consecutive patients (40 male/148 female; mean age 51.4 ± 18.3 years; range 29–73 years). Thrombosis occurred in 12/188 patients (incidence 6.38%), and was located in the subclavian, jugular, axillary, or upper limb vein of the catheterized side in 10/12 patients, and the femoral vein in two of 12 patients. Thrombosis occurred within 2 weeks of PICC in seven of 12 patients (58.33%), and within 1 month of PICC in two of 12 patients (16.67%). In total, nine of 12 thromboses (75.0%) occurred before the end of the second course of chemotherapy.
Demographic and clinical characteristics of patients undergoing chemotherapy via peripherally inserted central catheter (PICC), stratified according to the presence or absence of venous thrombosis.

Data presented as n (%).
χ2-test.
Insufficient data for statistical analysis.
NS, not statistically significant (P ≥ 0.05).
BMI, body mass index; Hb, haemoglobin; RBC, red blood cell; WBC, white blood cells.
Logistic regression analysis of risk factors associated with thrombosis in patients undergoing chemotherapy via peripherally inserted central catheter (PICC) (n = 188).
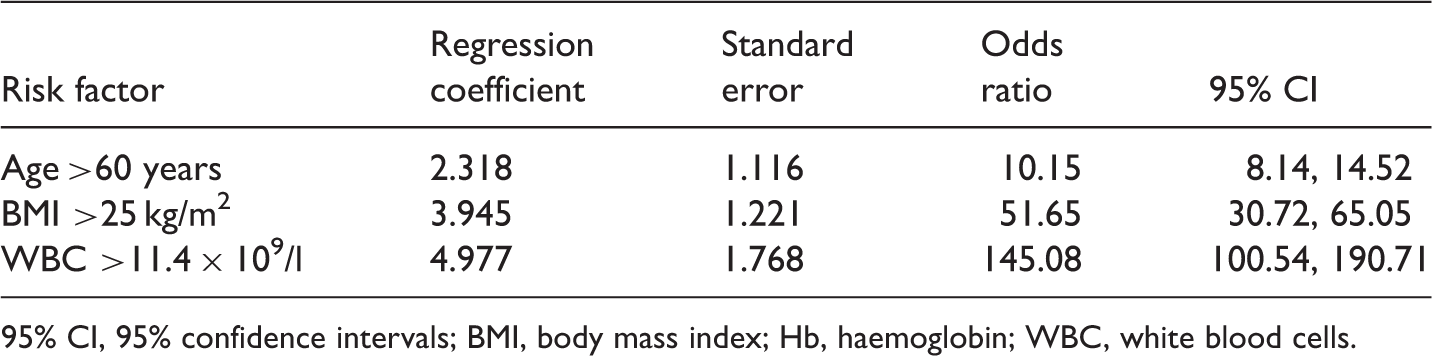
95% CI, 95% confidence intervals; BMI, body mass index; Hb, haemoglobin; WBC, white blood cells.
Discussion
The incidence of venous thrombosis was 6.38% in the present study of PICC, approximately three times that reported in a study of central venous catheters. 9 In accordance with the findings of others, 14 there was a significant correlation between thrombosis and age >60 years in the present study. It is thought that vascular endothelial cells produce increasingly high levels of procoagulants (such as von Willebrand factor and plasminogen activator inhibitor-1) with advancing age, 20 resulting in hypercoagulation. Changes in gonadotropins also predispose elderly people to thrombosis. 20 Age >60 years is a risk factor in the Davidson–Caprini Model11,12 and other risk assessment scales.15
We identified a significant correlation between thrombosis and BMI > 25 kg/m2. BMI values in thrombosis risk assessment scales vary between 25 and 35 kg/m2 or higher,21,9 but the highest BMI value in the present study was 27 kg/m2. BMI varies greatly according to ethnic group. 10 Obesity is a known risk factor for VTE11,12; adipocytokines such as leptin and adiponectin can enhance the activity of the coagulation system and decrease fibrinolytic activity by interfering with blood fat and sugar tolerance-related metabolism.22–24
In accordance with the findings of others, 9 high WBC count (>11.4 × 109/l) was identified as a significant risk factor for thrombosis in the present study. WBC-derived tissue factor (TF) has a role in pathological thrombosis,9,25 and large numbers of TF-containing microparticles can be detected in the blood of patients with severe infection, metastatic cancer or DVT.26,27
Female patients are known to have an increased risk of thrombosis, 28 and both chemotherapy and estrin treatment can increase the risk of thrombosis in patients with breast cancer. 29 TF is involved in haemostasis and thrombosis,30,31 and TF activity is related to hyperlipidaemia, smoking and platelet count. 32 It has been suggested that hypertension can cause extensive damage to vascular endothelial cells, leading to excessive TF release that starts the cascade reaction of extrinsic coagulation. 33 Logistic regression analysis in the present study revealed no significant associations between thrombosis risk and sex, breast cancer, history of smoking, platelet count or hypertension. Both a personal and a family history of thrombosis are risk-assessment items in some scales,13,15 but there was no significant relationship between thrombosis risk and these parameters in the current study.
A study found that patients with three or more thrombosis risk factors accounted for >50% of 142 patients with DVT, whereas those with two or more risk factors accounted for >75%. 34 In addition, Anderson and Spencer 35 reported that patients with two or more risk factors accounted for 76% of 1231 patients with VTE, whereas patients with three or more risk factors accounted for 39%. These data indicate that thrombosis is often a consequence of multiple risk factors, but the actual number of risk factors is not a specific predictor of thrombosis.
Common acquired thrombotic risk factors include trauma, surgery, malignant tumours and the presence of antiphospholipid antibodies. 36 These factors are closely associated with venous thrombosis in hypertension, coronary heart disease, heart failure, diabetes mellitus, cerebral infarction and smoking.37,38 Major genetic risk factors include mutations in coagulation factor V Leiden39,40 and prothrombin 20210A, 41 and defects in protein C and protein S. 42 Thrombosis is thus a combined consequence of acquired and hereditary thrombotic risk factors.
The present study included only Chinese patients undergoing PICC chemotherapy; it is not possible to determine whether the findings are applicable to the wider population. Although we identified three risk factors for thrombosis in patients undergoing PICC chemotherapy, we believe that comprehensive assessment of thrombosis risk is necessary.
In conclusion, this study identified age >60 years, BMI >25 kg/m2 and WBC >11.4 × 109/l as risk factors for thrombosis in Chinese patients undergoing PICC chemotherapy. These patients are already at high risk of VTE due to the presence of three major risk factors (tumour, chemotherapy and PICC). Careful attention should therefore be paid to patients with one or more risk factors, including thorough checking for signs and symptoms of DVT and early symptoms of pulmonary embolism. B-mode ultrasonography and pulmonary angiography should be promptly performed and low-dose or low-molecular-weight heparin should be given to prevent DVT when indicated. 43
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported by the Education Department of Zhejiang Province, China (Grant# N20090118) and the Science and Technology Department of Zhejiang Province, China (Grant# G20110020).