
Abstract
Objective
Closed reduction (CR) is a noninvasive treatment for developmental dysplasia of the hip (DDH), and this treatment is confirmed intraoperatively. This study aimed to develop a preoperative estimation model of the probability of requiring open reduction (OR) for DDH.
Methods
The study design was cross-sectional by screening all patients younger than 2 years who had attempted CR between October 2012 and July 2016 by a single surgeon. Potential diagnostic determinants were sex, age, side, bilaterality, International Hip Dysplasia Institute (IHDI) grade, and acetabular index (AI). An intraoperative arthrogram was the reference standard. A logistic regression equation was built from a reduced model. Bootstrapping was performed for internal validity.
Results
A total of 164 hips in 104 patients who met the inclusion criteria were analysed. The prevalence of CR was 72.2%. Independent factors for OR were older age, higher IHDI grade, and lower AI. The probability of OR = 1/[1 + exp − (−2.753 + 0.112 × age (months) + 1.965 × IHDI grade III (0 or 1) + 3.515 × IHDI grade IV (0 or 1) − 0.058 × AI (degrees)]. The area under the curve was 0.79.
Conclusion
This equation is an objective tool that can be used to estimate the requirement for OR.
Keywords
Introduction
In developmental dysplasia of the hip (DDH), closed reduction (CR) in the operating room continues to be a useful procedure up to the age of 18–24 months. 1 Splinting may be first applied to dysplastic or mildly subluxated hips. However, open reduction (OR) is performed if splinting and CR fail.2,3 The long-term outcomes of both treatment modalities are comparable.3,4Because of concerns related to adequacy of acetabular remodelling in older children, only a few centres perform CR after the age of 2 years.5,6
There are several intra- and postoperative aids for decision-making that are mainly based on arthrographic and axial images. Recently, ultrasonography has been used.7–10 One or more of these modalities are used to confirm the success of CR. There is limited information available in the literature regarding the added value of preoperative plain radiographs in predicting achievable CR.11,12
The operative time varies considerably between CR and OR. Moreover, parents often seek to be enlightened about the invasiveness of the proposed intervention. This study aimed to develop an objective diagnostic tool to predict the type of reduction for DDH that is based on readily available clinical information.
Patients and methods
Selection of patients
A cross-sectional study was performed. The study was approved by the institutional review board at King Fahad Medical City (log number: 14-245) and patients’ consent was waived. Data were collected from a single surgeon’s practice. Consecutive patients with DDH who underwent attempted CR between October 2012 and July 2016 were enrolled. Inclusion criteria were the diagnosis of DDH, age younger than 2 years, and International Hip Dysplasia Institute (IHDI) grade II or higher (Figure 1).
13
International Hip Dysplasia Institute (IHDI) classification. This classification is based on the location of the H-point, which is the midpoint of the ossified femoral metaphysis
In the CR group, there was clear evidence of successful reduction besides an initial intraoperative arthrogram. We performed post-reduction computed tomography (CT) and / or an arthrogram showing concentric reduction during cast change. In the OR group, all of the patients were screened for evidence of attempted CR before inclusion. Patients with preoperative ultrasound and no plain films were excluded. We did not include teratological or neuromuscular hips.
Treatment
CR was performed under general anaesthesia with the aid of a standard arthrogram. The arthrogram was performed by injecting 2–3 mL of contrast material (diluted 1:1) inferior to or through the adductor longus tendon. The adequacy of CR was determined based on whether the limbus was simply obstructive. Only a thin line of dye pooling was accepted, where the femoral head was under the limbus. 14 After the CR procedure, percutaneous adductor tenotomy was performed. CR was abandoned if the safe zone of Ramsey remained noticeably narrow after adductor release or if the Ortolani manoeuver was felt to be forceful. 15 The reduction was followed by application of a hip spica cast in the human position with a gentle posterior mold at the greater trochanteric region. 16 Fluoroscopy images were obtained before the patients left the operating room. Only two patients (four hips) needed Kirschner wires to maintain concentric reduction, with one in each diagnostic group. The cast was used for 3–4 months and was changed at least once under general anaesthesia. All of the patients wore a Craig abduction splint full-time for 6 weeks and overnight after this time. None of the patients had preoperative overhead traction. In cases in which CR failed, the patient underwent OR during the same operative session. Adequacy of reduction was based on the equivalent of Shenton’s line as observed on axial images. 8
Potential predictors
Charts were reviewed for information on the patient’s age, sex, side, bilaterality, operative details, and complications. Preoperative anteroposterior pelvic radiographs were examined electronically (Centricity PACS; GE Medical Systems, Slough, United Kingdom) to determine the acetabular index (AI) and IHDI grade. Post-reduction images were reviewed to confirm the intraoperative findings.
As a more direct measure of acetabular dysplasia, the AI was measured using the lateral end of the acetabular lip rather than the lateral bony margin of the acetabular roof (Figure 2).
17
Reliability of this measurement was reported by Agus et al.
18
Predictors that were impractical to obtain in the ambulatory care setting or those that had a subjective interpretation were excluded from this study.
Measurement of the acetabular index (AI) from the lateral end of the acetabular lip compared with the lateral bony margin of the acetabular roof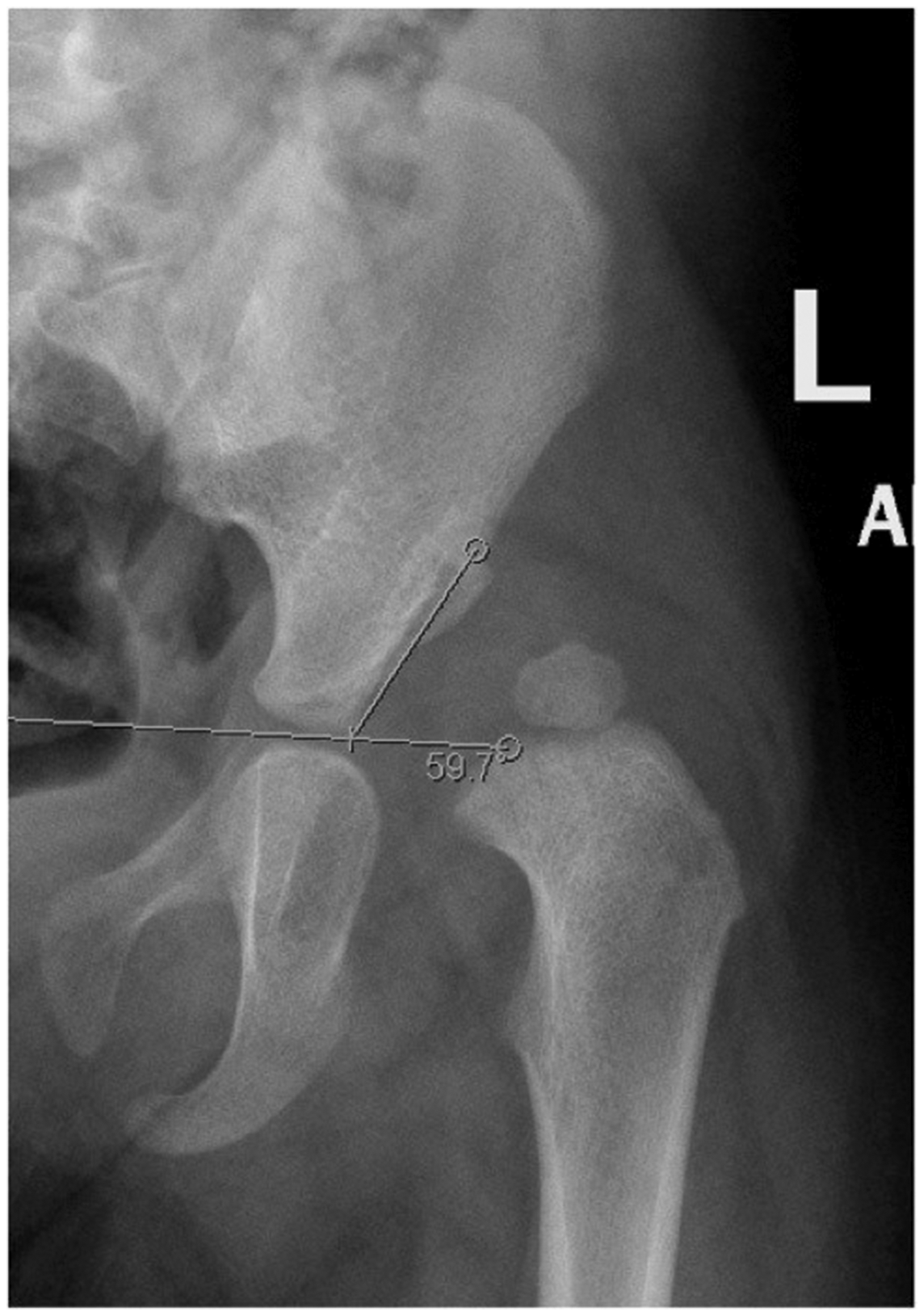
Statistical analysis
Data analysis was performed using R software for statistical analysis, version 3.3.1 (R Foundation for Statistical Computing, Vienna, Austria). Pearson’s chi-squared test was used when comparing proportions. For continuous data, normality was assessed visually. Bartlett test used to confirm the homogeneity of variance. The two-sample t-test was then performed. Two-tailed P values of < 0.05 were considered to be significant. For development of the prediction model, we used the backward stepwise binary logistic regression model. The final model was chosen manually based on clinical importance, P values, and Akaike’s information criterion. The variance inflation factor (VIF) was added to quantify multicollinearity. The performance of the fitted model was then analysed with the receiver operating characteristic (ROC) curve. A calibration curve was computed.
Results
Univariate analysis for potential predictors of open reduction

IHDI, International Hip Dysplasia Institute; CR, closed reduction; OR, open reduction.
Multivariate analyses for predictors of open reduction

IHDI, International Hip Dysplasia Institute; CI, confidence interval; VIF, variance inflation factor.
The highest VIF in the model was 1.09 (Table 2), which is below the accepted higher limit of 2.5. This finding indicated a stable model and no significant multicollinearity. The area under the ROC was 0.79 (Figure 3a). This area ranged between 0.5 to 1.0, and the closer to 1.0, the better the overall discriminative value of the model. Reasonable calibration was observed (Figure 3b), but there was overestimation of the probability of OR for higher values, which we believe is clinically desirable.
(a) Receiver operating characteristic (ROC) curve of the model. (b) Calibration curve.
Based on the coefficients of independent predictors (Table 2), the derived prediction equation for calculating the probability of OR was determined as follows:

There were no complications related to the diagnostic tests. One eligible patient had redislocation that occurred after an arthrogram and CR. This redislocation was confirmed in postoperative CT. The patient was treated the following day by OR and analysed in the OR group. None of the hips in this study were subluxated or dislocated during the routine follow-up visit; 6 weeks after cast removal.
Discussion
This study provides an equation to calculate the probability of the type of reduction required. An older age, high IHDI grade, and low AI were independent predictors for OR. Failed CR and the potential requirement for secondary procedures are probably less detrimental to the long-term outcome than failure of OR. 19 In the present study, CR was attempted in children aged up to 2 years.
Tönnis initially quantified hip displacement into four categories on the basis of the location of the femoral head ossific nucleus. His classification was later modified, reducing the number of classes to three. 20 Because the ossific nucleus is not always present in patients with DDH aged older than 6 months, IHDI classification was used in our study. 13 Several investigations have used femoral head displacement as a prognostic factor, but only a small number of studies have documented its association with successful CR.5,11 Bicimoglu et al. 11 performed a study of 137 hips that underwent CR after lengthening of the adductor longus tendon and iliopsoas in patients aged younger than18 months. They documented an increased rate of OR with higher femoral head displacement in 30% of patients for Tönnis grade 2 and 87% for Tönnis grade 4. They reported no increase in the requirement for OR with age. In the present study, almost all patients with IHDI grade II, 89% with IHDI grade III, and 56% with IHDI grade IV had CR. Luhmann et al. 21 showed that OR procedures were directly associated with age. Recently, Bolland et al. 12 reported more ORs with increased age and Tönnis grade. In the present study, patients with hips that required OR showed a significantly older age and higher IHDI grade than those with hips treated with CR. Arthrographic CR of IHDI grade II hips in this age group is controversial. Guidelines of this situation are lacking in the literature, and the choice of CR in the operating room or application of abduction splinting requires clinical judgment. Based on the current findings, we are now performing more abduction splinting and less CR for IHDI grade II.
Despite technological advances in the imaging of dysplastic hips, conventional radiography remains important. Measuring the AI of the lateral end of the acetabular lip was reported by Kim et al. 17 and later examined by Agus et al. 18 Both of these studies resulted in observers’ agreements that were similar to conventional AI. However, the interclass correlation was not reported in these two studies. In the present study, multivariate analysis showed that the higher the AI, the greater the chance of CR. This finding could be partially explained by the possibility that patients with a lower radiographic acetabular lip have a larger overlying fibrocartilaginous ridge. Ponseti described this finding in an autopsy study and suggested that this ridge is formed by pressure of the femoral head on the outer acetabular margin. 22 Because the shape of the labrum was not determined in the present study, the author could not draw a conclusion about its effect on the rate of OR.
In this study cohort, postoperative CT was feasible for confirming the adequacy of hip reduction. Chin et al. 23 reported 100% sensitivity for magnetic resonance imaging (MRI) and CT in detecting postoperative hip displacement, but MRI is more specific. Because of concerns related to ionizing radiation exposure, MRI is becoming the imaging method of choice. 24 Additionally, the follow-up period does not extend beyond the first follow-up visit; however, the incidence of redislocation after this point in time is low. Case et al. 25 found no redislocation in 67 hips 2 months after reduction.
The prediction equation presented here is not intended to replace the reference standard, namely an intraoperative arthrogram by which the adequacy of CR is confirmed. The prior probability calculated from the formula needs to be updated after an arthrogram. Limitations of this study are potential information bias, the sensitivity of the AI to subtle rotation and tilt, and possible differences in the appearance of femoral head migration between supine and standing radiographs. The outcome of the reduced hips in both groups needs to be determined by a future prognostic study.
Determining the probability of needing to perform OR will enable clinicians to perfect the treatment strategy and plan efficient operative care. More research focussing on confirming the association between preoperative plain radiographic findings and the type of intervention is required.
Footnotes
Acknowledgements
The author would like to thank Benjamin De Boer, PhD, for assistance with writing the manuscript of this study.
Declaration of conflicting interest
The Author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.