
Abstract
Objective
To investigate the prevalence of hepatitis E virus (HEV) antibodies and RNA in voluntary blood donors, in China.
Methods
Serum samples from blood donors were collected sequentially at six blood donation centres in five geographical regions of China. Donors were stratified between two groups according to their serum alanine aminotransferase (ALT) concentration (≤40 U/l and >40 U/l. Enzyme-linked immunosorbent assay and reverse transcription–polymerase chain reaction were used to quantify anti-HEV antibodies and RNA, respectively.
Results
In total, 21.1% (172/816) of donors were positive for anti-HEV immunoglobulin (Ig) G (elevated ALT samples group 18.9% [85/450]; normal ALT group 23.8% [87/366]), and 0.5% (four of 816) donors were positive for anti-HEV IgM (elevated ALT group 0.9% [four of 450]; normal ALT group 0% [none of 366]). The rate of anti-HEV IgG seropositivity was significantly higher in male than in female donors. No serum sample tested positive for HEV RNA.
Conclusion
The prevalence of anti-HEV antibodies in blood donors in China is high, regardless of ALT concentration.
Introduction
Hepatitis E is an important public health problem that is caused by hepatitis E virus (HEV), a member of the Hepeviridae family. Epidemiological data suggest that HEV may pose a threat to the safe supply of blood for transfusions.1–4
In China, the mandatory screening test panel for voluntary blood donors includes quantification of alanine aminotransferase (ALT), 5 and elevated ALT is the main reason for discarding donated blood. However, ALT concentrations can be affected by factors other than liver disease (including drug or alcohol use, inadequate sleep and being overweight), 6 with the result that blood donations may be discarded unnecessarily. Many countries either do not have compulsory ALT testing for blood donors or use a high ALT cut-off value.7,8
The aim of the current study was to investigate the prevalence of HEV antibodies and RNA in blood donors with elevated or normal ALT concentrations, and to determine whether there is a relationship between ALT concentration and HEV infection.
Subjects and methods
Study population
Samples for this study were collected sequentially for this study, which took place between January and December 2012. All potential blood donors were required to pass a routine predonation screening process, including health-history questionnaire screening, predonation rapid testing (for screening hepatitis B virus surface antigen, ABO blood type, hemoglobin, ALT, HIV, and Treponema pallidum), and a brief physical examination. After a donor passed the predonation screening phase, a unit of blood was collected. In addition, 5 ml of venous blood was collected in two vacuum tubes containing ethylenediaminetetra-acetate-K2 (with separator gel). Plasma was separated from red-blood cells by centrifugation (at 4℃, 2500
Exclusion criteria were positive tests for hepatitis B surface antigen, hepatitis C virus (HCV) antibodies, Treponema pallidum or HIV.
The study protocol was approved by the ethics committee of the Institute of Blood Transfusion, Chinese Academy of Medical Sciences, Chengdu, China, and all donors provided written informed consent.
ALT quantification
The ALT level was quantified via the rate method: 9 ALT concentrations ≤40 U/l were defined as normal; ALT concentrations >40 U/l were defined as elevated.
Anti-HEV serology
Anti-HEV immunoglobulin (Ig)G and IgM antibodies were detected by enzyme-linked immunosorbent assay (ELISA) using HEV IgG and IgM ELISA kits (Wantai Pharmaceutical Co., Beijing, China), according to the manufacturer’s instructions. ELISAs were performed on an automated microplate reader (Molecular Devices LLC, Sunnyvale, CA, USA). According to the package insert, the assay had a specificity of 99.9% when testing 10587 healthy Asian subjects. It is to be noted that confirmatory assays for HEV IgM and IgG antibodies were not available.
HEV RNA detection
All serum samples were tested for HEV RNA by reverse transcription quantitative polymerase chain reaction (RT–qPCR). Nucleic acid isolation was performed using a viral RNA extraction kit (Daan Gene Co., Guangzhou, China) according to the manufacturer’s instructions. Primer sequences for PCR were: forward 5′-ATCCCGCATGACATCGAC-3′, reverse 5′-GGTCGGTCCTGCTCATGTT-3′, and probe FAM-5′-CGGGGAATCTCGTGTAGTTATTCAG-3′-TAMRA. PCR cycling conditions were 40 cycles of denaturation at 94℃ for 15 s, annealing at 55℃ for 30 s, and extension at 72℃ for 40 s. A positive HEV RNA control (1000 copies/ml) and negative HEV RNA control were included in each assay. Amplification, data acquisition and analysis were performed on an ABI StepOne Plus™ Detection System (Life Technologies, Carlsbad, CA, USA).
Statistical analyses
Data were presented as n (%) or mean ± SD. Between-group comparisons were made using one-way analysis of variance followed by Student’s t-test with Tukey’s correction. All statistical analyses were performed using SPSS® version 12.0 (SPSS Inc., Chicago, IL, USA) for Windows®. P-values < 0.05 were considered statistically significant.
Results
The study included 450 blood donors with elevated ALT (396 male/54 female; mean age 30 ± 8 years; age range 18–55 years; Guangzhou Blood Centre n = 33; Xian Blood Centre n = 100; Nanjing Blood Centre n = 50; Suzhou Central Blood Station n = 90; Deyang Central Blood Station n = 127; Beijing Blood Centre n = 50), and 366 blood donors with normal ALT concentrations (183 male/183 female; mean age 24 ± 8 years; age range 19–53 years; Guangzhou Blood Centre n = 20; Beijing Blood Centre n = 20; Nanjing Blood Centre n = 20; Xian Blood Centre n = 30; Suzhou Central Blood Station n = 90; and Deyang Central Blood Station n = 186). All serum samples were negative for HEV RNA.
Prevalence of anti-hepatitis E virus (HEV) immunoglobulin (Ig)G and IgM in volunteer blood donors from Chinese blood centres, stratified according to serum alanine aminotransferase (ALT) concentration.
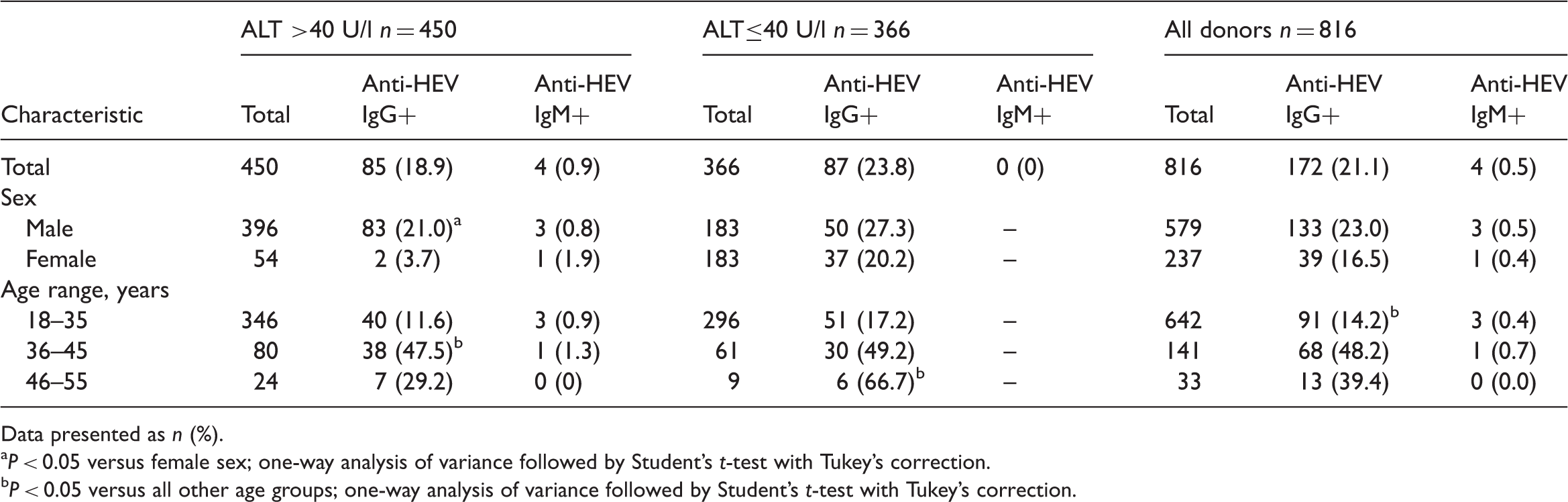
Data presented as n (%).
P < 0.05 versus female sex; one-way analysis of variance followed by Student’s t-test with Tukey’s correction.
P < 0.05 versus all other age groups; one-way analysis of variance followed by Student’s t-test with Tukey’s correction.
In donors with elevated ALT, anti-HEV IgG seropositivity was significantly more common in those aged 36–45 years compared with other age groups (18–35 or 46–55 years; P < 0.05, Table 1). In contrast, in donors with normal ALT levels, anti-HEV IgG seropositivity was significantly more common with increasing age, being higher among older donors (aged 46–55 years) than those aged 18–35 or 36–45 years (P < 0.05, Table 1). In the elevated ALT group, anti-HEV IgG seropositivity was significantly more common in male than in female donors (P < 0.05; Table 1).
Discussion
Transfusion-transmitted HEV infections due to contaminated blood products have been reported in Europe (including the UK) and Japan.1–4,8 Since the majority of HEV infections are subclinical, 10 the risk of asymptomatic infection in blood donors is a major concern. High rates of anti-HEV IgG seropositivity have been demonstrated among blood donors in many countries, with considerable variance between populations (China 0.07%; 11 USA 18.8%; 12 Germany 5.94–15.5%; 13 Switzerland 4.1–5.4%; 14 Brazil 2.3%; 15 France 3.2–16.6%; 16 Japan 3.4–6.6%; 17 Scotland 4.7%). 18 The rate of anti-HEV IgG seropositivity in the present study (21.1%) was considerably higher than the rates described above,11–18 irrespective of ALT concentrations. The anti-HEV IgM seropositivity rates in the present study were 0.9% and 0.0% for donors with and without elevated ALT, respectively. Others reported rates of 0.94–1.8% in China, 11 0.5–1.6% in Japan, 17 and 0.5% (normal ALT) and 8.08% (elevated ALT) in Germany. 13 These differences may be explained by demographic differences, and variations in ALT reference ranges.
In China, the majority of voluntary blood donors are young men. The prevalence of anti-HEV IgG seropositivity was significantly higher in male than in female donors in the present study, but the reasons for this pattern of infection remain unclear and require further investigation. It may be due to more frequent exposure to potential sources of contamination among donors, perhaps due to greater activity in the labour market (such as involvement in high-risk work in livestock farming, cleaning services or the sewage disposal system) in those who were anti-HEV IgG seropositive.
To obtain the true rate of HEV infection in Chinese blood donors we recruited subjects sequentially, with the result that the mean ALT concentration of samples in this study was not very high. In addition, HEV infection was asymptomatic and all donors were negative for HEV RNA.
Since the main factors influencing ALT levels are nonpathological, a large number of healthy blood donors are unnecessarily excluded in China. This can result in serious economic loss and also undue psychological stress to these excluded donors. It would therefore be useful to redefine testing methods and ALT cut-off levels, such has been undertaken in other countries. China has a high risk of hepatitis, so redefining ALT cut-off values or cancelling ALT testing altogether should be considered only after in-depth studies. If ALT testing is no longer recommended, anti-HEV IgM and IgG testing should be initiated, instead.
The current study had some limitations. We demonstrate that HEV circulates in five geographical regions of China, but data regarding HEV prevalence in other Chinese regions are lacking and merit exploration. Further studies are necessary to define the clinical and epidemiological importance of HEV infection in China, to identify sources and routes of transmission, and assess the possible risk of transfusion-transmitted HEV. Factors other than liver disease, including tobacco and alcohol use, can influence ALT concentrations. In China, these lifestyle choices are more common among men than women, and men account for the majority of blood donors. This compounds the risk of blood donations being discarded due to high ALT concentrations. A great deal of time was required to recruit the 54 female donors with elevated ALT in the present study, and it was not possible to sex match the two study groups.
In conclusion, this cross-sectional study shows a high prevalence of anti-HEV antibodies in blood donors in China, regardless of ALT concentration, and indicates that HEV is highly prevalent in this population. It remains unclear whether cancelling ALT screening or redefining ALT cut-off values might be required. We plan to undertake a large-scale study, in collaboration with Chinese Blood Centres, that includes other hepatitis viruses (hepatitis A and hepatitis G), to examine this issue further.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported by the research special fund for public welfare industry of health (Grant Nos. 200902008 and 201002005).