
Abstract
Objective
To examine the cooling effectiveness of a rapid infusion system (RIS) during induction of therapeutic hypothermia.
Methods
This laboratory study simulated the effect of three fluid delivery methods: rapid dripping without any other equipment (control); RIS; pressure bag. Cold energy loss (℃ × min) was calculated as: (temperature of the proximal thermoprobe – temperature of the distal thermoprobe) × (total infusion time).
Results
Infusion time was significantly shorter and cold energy loss significantly lower in the RIS group than in the two other groups.
Conclusions
RIS preserves the cold energy of fluid more effectively than pressure bag or control. RIS allows for rapid infusion at a constant pressure and can be easily applied in an emergency setting.
Introduction
Therapeutic hypothermia (TH) is used to protect the brain and other organs of patients who remain comatose after the return of spontaneous circulation (ROSC) following cardiac arrest.1,2 Although the optimum timing is unclear, physicians generally induce moderate hypothermia as soon as possible after ROSC. 3 Several methods are used for the induction and maintenance of therapeutic hypothermia, including feedback-controlled endovascular catheters, surface cooling devices, cold saline (4℃), cooling blankets and ice bags. Cold saline infusion is the preferred method because it is convenient, and cost-effective, and has a good safety profile.4–7
As cold saline infusion lowers core temperature by decreasing the heat content of the body, 8 the refrigerated fluid should be kept as cool as possible until delivery. Room temperature, length of the infusion line and speed of infusion influence the temperature of saline at the infusion site. Insulation has been applied to minimise increases in saline temperature.9,10 We hypothesized that the infusion of cold saline using a rapid infusion system (RIS; as used in many emergency departments) might be effective for the induction of hypothermia and assist in maintaining low saline temperatures. In a laboratory setting, RIS was compared with full dripping without other equipment (control) and the use of a pressure bag.
Materials and methods
Experimental design
This study was conducted in a resuscitation room at the Department of Emergency Medicine, Chung-Ang University Hospital, Seoul, Republic of Korea, on 5 September 2013. Objects in the room that could radiate heat were removed or switched off, and the environmental temperature was maintained at 21.0 ± 1.0℃ during the experiment. Normal saline (0.9%, 1 l/bag; Safe-Flex, Cheiljedang Co., Seoul, Republic of Korea) was stored in the refrigerator (4℃) for ≥24 h before the experiment. After being removed from the refrigerator, the fluid bag was shaken, connected to an 80-cm intravenous (i.v.) infusion set (1 ml = 20 drops; HMS Co., Seoul, Republic of Korea) and hung on an i.v. pole. Thermoprobes (oesophageal stethoscope with temperature sensor; DeRoyal, Powell, TN, USA) were inserted into: (i) the proximal chamber of the infusion set; (ii) the distal rubber injection port of the i.v. line. Continuous temperature monitoring was performed by connecting the thermoprobes to a patient monitor (IntelliVue MP70; Philips, Boebilingen, Gemany). The height of the i.v. pole was identical to the height of the RIS (172 cm). The distal end of the infusion set was connected to a 16-G angio-catheter (Introcan Safety; B Braun, Melsungen, Germany) that was 65 cm above floor level. All experiments used identical infusion sets and equipment.
There were three experimental groups: control (full dripping without any pressure device); RIS (fluid placed in the chamber of a pressure infusor [Ranger; Arizant Healthcare, Eden Prairie, MN, USA] at 300 mmHg); pressure bag (conventional pressure bag with gauge, inflated to 300 mmHg at the start of infusion and whenever the pressure decreased to <100 mmHg). The experiment was performed 10 times in each group.
Measurements
The temperature of the fluid bag at the proximal chamber of the infusion set was noted prior to infusion. During infusion, the fluid temperature was recorded by both thermoprobes at 1-min intervals. Total infusion time was recorded. The increase in fluid temperature (cold energy loss; ℃ × min) was calculated as: (temperature of the proximal thermoprobe – temperature of the distal thermoprobe) × (total infusion time).
Statistical analyses
Data were presented as mean ± SD. Between-group differences were analysed using one-way analysis of variance. Statistical analyses were performed using SPSS® version 20.0 (SPSS Inc., Chicago, IL, USA) for Windows®. P-values <0.05 were considered statistically significant.
Results
Data regarding rates of infusion and saline temperatures in the three groups are shown in Table 1. There were no significant between-group differences in the initial fluid temperature at the proximal chamber. Infusion occurred significantly faster in the RIS group than in both other groups (P < 0.001 for each comparison; Table 1). After infusion, the mean saline temperature at the distal end of the i.v. line was significantly lower in the RIS group than in both other groups (P = 0.001 between RIS and control, P = 0.043 between RIS and pressure bag; P = 0.003 between control and pressure bag; Table 1) Cold energy loss was calculated as 30.95 ± 3.35℃ × min in the control group, 3.87 ± 4.20℃ × min in the RIS group, and 6.30 ± 0.87℃ × min in the pressure bag group. Cold energy loss was significantly lower in the RIS group than in both other groups (P < 0.001 for each comparison; Figure 1).
Comparison of temperature changes according to different infusion methods in a laboratory-based experiment to determine the effectiveness of a rapid infusion system in the induction of therapeutic hypothermia using cold saline. ‘Cold energy loss in the RIS group (b) was significantly lower than in the control (a) or pressure bag groups (c) (P < 0.001, each comparison). Duration of infusion and initial and final saline temperatures in a laboratory-based experiment to determine the effectiveness of a rapid infusion system in the induction of therapeutic hypothermia using cold saline. Data presented as mean ± SD. P < 0.001 versus both other groups; one-way analysis of variance. Control, full dripping with no pressurization. Experiment performed 10 times in each group.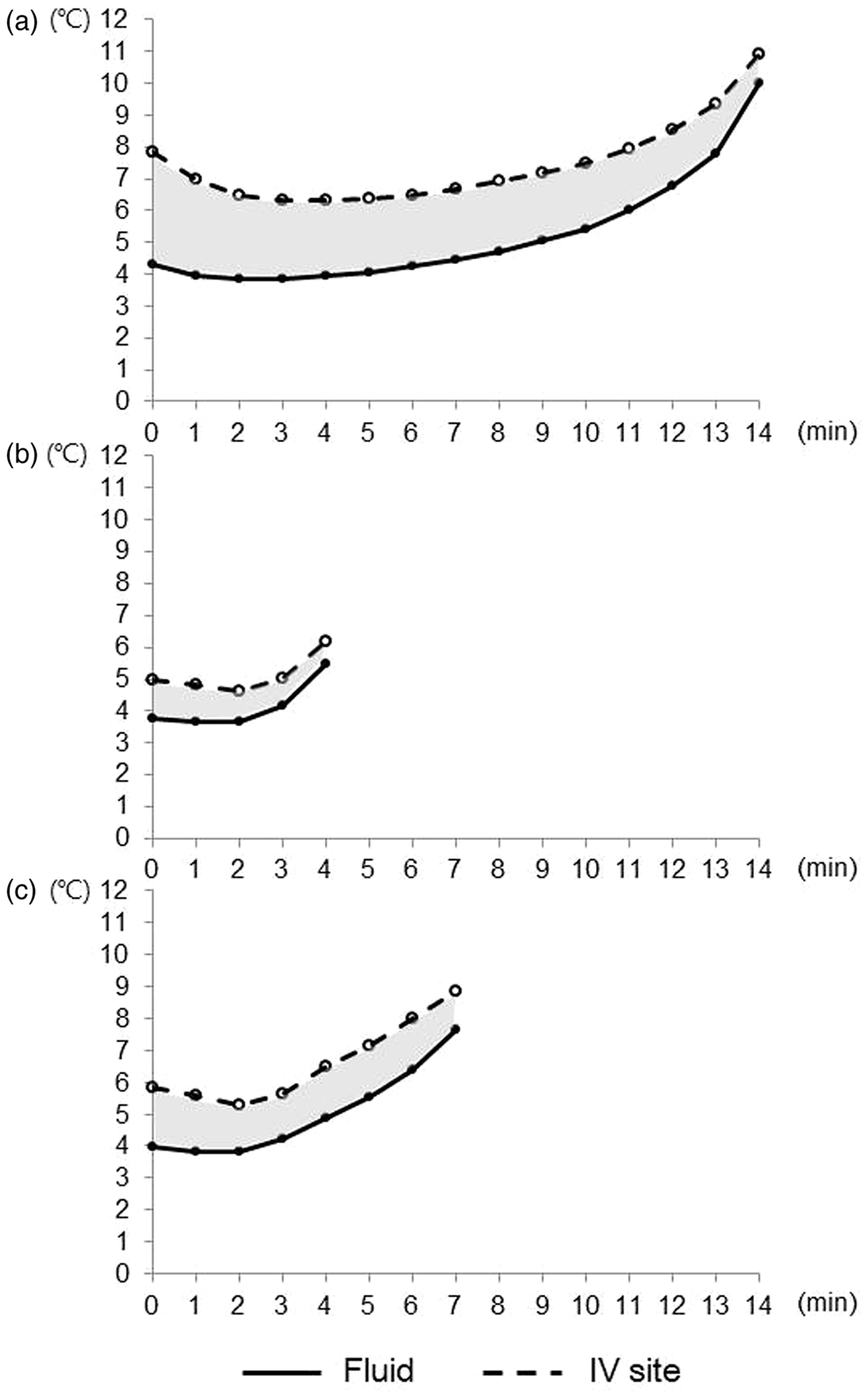

Discussion
The 2010 International Liaison Committee on Resuscitation guidelines for cardiopulmonary resuscitation recommend that comatose adult patients who experience an out-of-hospital cardiac arrest due to ventricular fibrillation should be cooled to 32–34℃ for 12–24 h following ROSC. 3 Induced hypothermia may also be considered for comatose adult patients on ROSC following in-hospital cardiac arrest of any initial rhythm or after an out-of-hospital cardiac arrest (OHCA) with an initial rhythm of pulseless electrical activity or asystole. 3 However, no definitive guidelines for the timing and method of therapeutic hypothermia induction are available.
Although some studies have indicated that early induction of therapeutic hypothermia has no beneficial effect on neurological outcome, clinical consensus is to reach the target temperature as early as possible after ROSC.11–14 Rapid infusion of cold saline is widely used to induce hypothermia because it is simple and cost-effective, and has a good safety profile. There are several techniques to improve the cooling effect of cold saline, including use of a pressure bag and insulating the cold saline bag and infusion set.9,10
Hypothermia is frequently induced in patients resuscitated from OHCA in the emergency department.4,15,16 To improve the effectiveness of cold saline in induction of hypothermia, the fluid should be maintained at a low temperature, the infusion should be rapid and the infusion line should be short. It is difficult to shorten the infusion line length in a clinical setting because infusion sets are available at standard lengths only. In addition, no guidelines are available for the rate of infusion; physicians commonly use an infusion rate of 30–50 ml/min.4,5,17–20
Rapid fluid infusion via a pressure bag is inconvenient because conventional pressure bags deflate spontaneously. Repeated manual inflation is required and the gauge on the pressure bag must be monitored carefully. Fluid delivery pressure cannot be easily maintained and the effectiveness of the cold saline is decreased. Compared with other methods, RIS allows for more rapid and consistent infusion, reducing the volume of saline required to induce hypothermia. Volume overload can occur when inducing therapeutic hypothermia using cold saline, thus increasing the risk of pulmonary oedema, although research has shown that rapid infusion of cold saline did not cause pulmonary oedema. 15 Lowering the core temperature is important for the induction of therapeutic hypothermia, and maintaining the infusion fluid at a lower temperature can reduce the volume required. The environment surrounding patients with cardiac arrest is typically chaotic and several devices may be connected to the patient. Consequently, cold saline infusion via RIS would be convenient, since this equipment is commonly available in emergency medical centres.
The present study has several limitations. First, it was performed in an emergency department but could not accurately mimic the complex environment during patient resuscitation. Secondly, although the RIS is used to stabilise patients with shock, it is not known whether it is appropriate to use RIS to infuse cold saline into patients after cardiac arrest. Additional prospective studies are required to assess the safety and use of RIS in the induction of therapeutic hypothermia by cold saline infusion.
In conclusion, it is important to minimise the temperature increase of saline during induction of therapeutic hypothermia. RIS allows for rapid infusion at a constant pressure, and can be easily applied in an emergency setting. This method maintains a low fluid temperature and is a convenient means of fluid infusion compared with full dripping or the use of a pressure bag.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research was supported by the Chung-Ang University Research Grants in 2013.