
Abstract
Objective
To investigate tear-film break-up time and spatial distribution via noninvasive Keratograph 4 in patients with cataracts and dry eye syndrome (DES).
Methods
Noninvasive first break-up time (NIKf-BUT) and average break-up time (NIKav-BUT) were evaluated via Keratograph 4 in patients with age-related cataracts and DES. The location and size of tear break regions were recorded and the distribution of first break-up areas was summarized. Patients also underwent conventional break-up time assessments (TBUT test and Schirmer’s test).
Results
A total of 43 left and 43 right eyes were examined. There was no significant difference between TBUT and NIKav-BUT. NIKf-BUT was significantly shorter than TBUT. Both NIKf-BUT and NIKav-BUT correlated positively with TBUT. In both the left and right eye, the most common first break-up areas were the peripheral domain of the inferior precorneal surface and the central domain of the superior portion.
Conclusions
The Keratograph 4 appears to provide an effective noninvasive method for assessing tear film, enabling effective preoperative evaluation of tear film break-up regularity, informing the location of the incision and reducing the probability of postoperative DES.
Introduction
Dry eye syndrome (DES) is a multifactorial disease that stems from impairment of the ocular surface and tear ducts, leading to ocular discomfort and tear film instability. 1 The incidence of DES is increasing, 2 and has an adverse impact on a patient’s health-related quality-of-life, especially among elderly populations.3,4 Among patients with age-related cataracts, extraction surgery or phacoemulsification often induces DES, 5–7 while intraoperative incision and heat damage decrease corneal sensitivity.8,9 In addition, the routine pre- and postoperative use of eye drops containing antiseptic compounds or steroids can lead to tear film instability. 7 Since the majority of cataract patients are elderly, dry eye symptoms may exist preoperatively and worsen postoperatively. It is therefore vital to evaluate the condition of the ocular surface before surgery. 10 Eye drops, such as artificial tears (ARTs), are recommended before and after surgery to prevent the occurrence of DES and relieve its symptoms,6,11 but not all cataract patients need such intervention and there is no index to assess individual need. Methods for effective preoperative identification of patients with pre-existing DES or the potential for surgery-induced dry eye are required, and guidelines for the application of ARTs need to be established.
The conventional tear break-up time test (TBUT) was introduced in 1969 1 2 and has since been universally applied for dry eye diagnosis, and used as a standard in many international diagnostic criteria.13–15 The fluorescein used in conventional TBUT may induce reflex tearing and decrease tear stability,16–18 leading to the development of noninvasive methods that avoid the limitations of conventional TBUT.16–19 These include high-speed videotopography, 20 meniscometry 21 and the tearscope, 22 but these techniques require the subjective judgement of the examiner, and uniform criteria for noninvasive break-up time (NIBUT) remain to be established.
In addition to break-up time, noninvasive methods that assess tear film distribution, thickness and dynamic changes could potentially be used to assess tear film stability.23–28 Our previous research 29 described a technique to map tear film thickness using the Pentacam® (Oculus, Wetzlar, Germany). The Keratograph 4 (Oculus) noninvasively measures the first and mean break-up times without the need for fluorescein, presenting a colour-coded tear map that dynamically locates break-up zones, which could not be achieved previously. The aim of the present study was to identify the first break-up zones in patients with cataracts and DES. In addition, NIBUT (as assessed via Keratograph 4) was compared with conventional TBUT measurement.
Patients and methods
Study population
The study recruited patients with bilateral cataracts and typical DES symptoms (dryness, foreign-body sensation, aesthenopia, burning, stinging and photophobia), undergoing cataract surgery at the Department of Ophthalmology, Eye and ENT Hospital of Fudan University, Shanghai, China, between June 2011 and September 2011. All patients underwent slit-lamp microscopic examinations and ophthalmic examinations, including measurements of visual acuity and intraocular pressure. Exclusion criteria were: (i) non age-related cataracts (e.g. caused by drug use or trauma); (ii) pre-existing ocular disease (uveitis, glaucoma, ocular trauma, keratitis, etc.); (iii) history of ocular surgery; (iv) use of eye drops for DES or other ocular conditions; (v) ocular disorders that influence the eye surface, such as lid lesions, lacrimal dust obstruction, allergies, blepharitis and pterygia. Data regarding previous systemic diseases, and symptoms of dry mouth and arthralgia, were collected. The right eye of odd-numbered patients and the left eye of even-numbered patients were chosen for further examination.
The study adhered to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of the Eye and ENT Hospital of Fudan University (IRB number, KJ2011-21). Verbal informed consent was obtained from each participant after the nature and possible consequences of the study were explained to each patient.
DES diagnosis
Diagnosis of DES was performed according to Japanese dry eye diagnostic criteria, 30 requiring the presence of more than one subjective symptom (dryness, foreign-body sensation, burning sensation, photophobia, visual fatigue or blurred vision, red eye, etc.), and at least one of the following: (i) tear film instability (TBUT) ≤10 s; (ii) reduced tear production (Schirmer’s test 31 ) ≤5 mm/5 min; (iii) fluorescein staining score (van Bijsterveld standard 31 ) ≥1.
Tear film assessment
Tear film assessment with the Keratograph 4 was conducted ≥30 min before conventional examinations, in order to avoid any influence of fluorescein on tear film stability. Patients were seated at the Keratograph 4 in a darkened room with the eye focused on the central target, and a placido disc pattern comprising 22 illuminated rings was projected onto the corneal surface. The patient was asked to blink three or four times and then keep their eyes open for as long as possible. The instrument discontinued measurement at the next blink. Irregularities on the image indicated the instability or break-up of the tear film. At the same time, a video was recorded. After completion of each measurement, the instrument provided a representation of tear film break-up over time, including a tear map showing the location and size of the tear-break regions, as well as the first break-up time (NIKf-BUT) and average break-up time (NIKav-BUT; the mean of all tear film break-ups occurring over the entire cornea). A single eye of each patient was examined three times at 5-min intervals. NIBUT was determined, as described. 17
A representative Keratograph 4 noninvasive tear film measurement is shown in Figure 1. The tear film assessment software divides the 360° ocular surface into 24 bands (15° for each band; top right panel, Figure 1), then subdivides each band into eight small rectangles (with longitude numbers 1–8), each of which serves as a basic break-up unit. The colour of the unit in a certain location represents the BUT of this unit, which changes in colour from red to yellow to green as BUT increases. In the present study, the entire 360° precorneal surface was divided into six areas of 60° each, and each area was divided into two domains by longitude 4. The domain of each first break-up unit was recorded.
A representative Keratograph 4 (Oculus, Wetzlar, Germany) noninvasive tear film assessment of the left eye of a patient with age-related cataracts and dry eye syndrome. Left panel: a dynamic video recording captures the process of tear break-up, with the red-framed rectangular break-up unit. This static screenshot shows the time of first break-up (NIKf-BUT) as 2.2 s, and the location of the first break-up area (inferior nasally). Upper right panel: the total break-up areas during the time during which the eye was open. Lower right panel: NIKf-BUT, average break-up time (NIKav-BUT), and automatic dry eye classification. The colour version of this figure is available at: http://imr.sagepub.com.
Break-up time (TBUT) test and Schirmer’s test (without anaesthesia) were performed. For the TBUT test, a fluorescein-impregnated strip was placed in the patient’s lower conjunctival sac after wetting with nonpreserved saline solution. The patient was asked to blink three to five times then keep their eyes open. The time between the last blink and the appearance of the first dark dot was recorded as TBUT. Schirmer’s test was carried out by placing a bent strip beneath the temporal lid margin and closing the eyes. The strip was removed after 5 min and the maximum wet length was measured. A single eye of each patient was examined three times at 5-min intervals. All measurements were carried out by the same trained optometrist (H.F.Y. or Y.X.J.) in one room, with constant temperature and humidity.
Statistical analyses
Data were presented as mean ± SD or n (%). Differences between TBUT and NIK-BUT values were compared using two-sample Wilcoxon rank-sum (Mann–Whitney) U-test. Between-domain differences in first break-up location were analysed by Cochran–Mantel–Haenszel test. The correlation between TBUT and NIK-BUT was determined using nonparametric Spearman analysis. Data were analysed with Stata®/SE software, version 10.0 (StataCorp, College Station, TX, USA). P-values <0.05 were considered statistically significant.
Results
The study included 86 patients with age-related cataracts (46 male/40 female; mean age 68 ± 10 years; age range 48–90 years). A total of 86 eyes (43 right/43 left) were examined.
Tear break-up time as assessed by TBUT was significantly longer than NIKf-BUT (3.54 ± 0.22 s vs 2.21 ± 0.23 s; P < 0.001). There was no significant difference between TBUT and NIKav-BUT (3.54 ± 0.22 s vs 4.20 ± 0.38 s; P > 0.05). Both NIKf-BUT and NIKav-BUT were positively correlated with TBUT (ρ = 0.638, P < 0.001 and ρ = 0.528, P < 0.001, respectively).
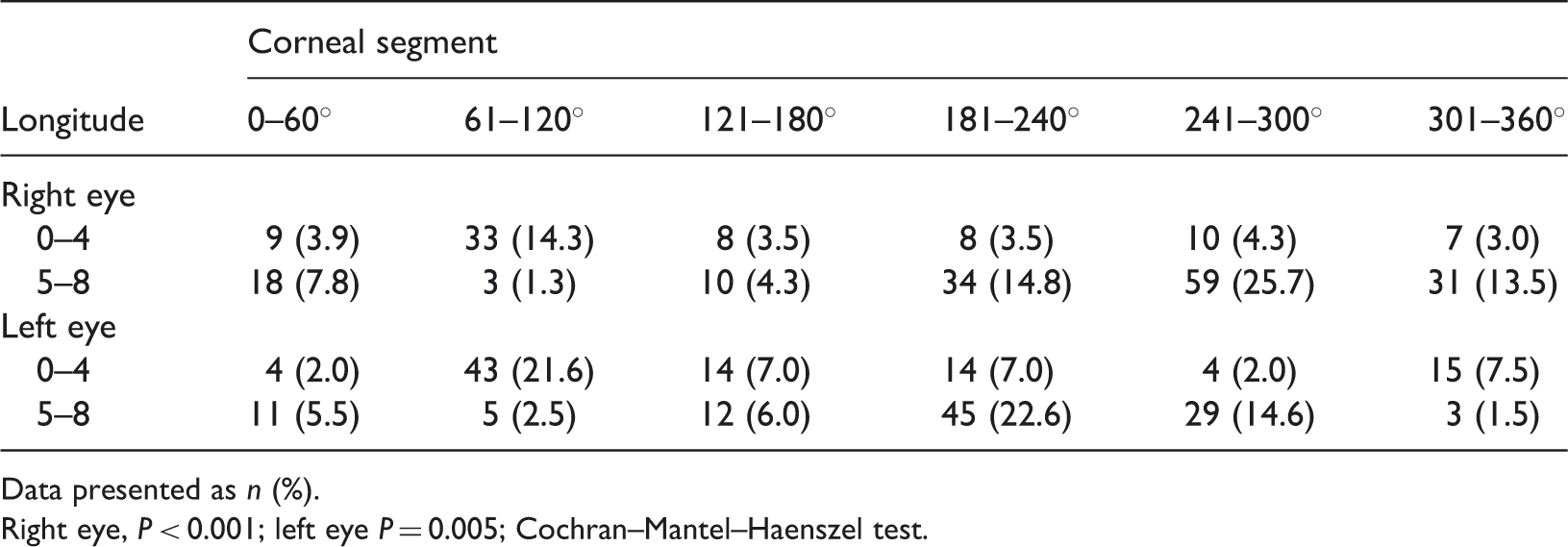
Figure 2 indicates the location of the first break-up areas in all 86 eyes (three readings each). When a first break-up unit was located in a given domain, it would be labelled once as a dot in this corresponding domain. The total number of dots in Figure 2 exceeds the total number of measurements because, in some eyes, several units broke simultaneously. The numbers of first break-up units for different domains are summarized in Table 1. There was a significant between-domain difference in both the right and left eyes (P < 0.001 and P = 0.0017, respectively). In both eyes, tear break-up tended to occur earlier in the peripheral domain of the inferior precorneal surface (181–360°) and the central domain of the superior portion (61–120°) than in any other region; in most areas, the total first break-up units were >10%.
Spatial distribution of first tear-film break-up in patients with age-related cataracts and dry eye syndrome (n = 43 left eyes and n = 43 right eyes). Each eye was examined three times; in some eyes, several tear units broke simultaneously. OD: right eyes; OS: left eyes. Location of first tear-film break-up in patients with age-related cataracts and dry eye syndrome (n = 43 left eyes and n = 43 right eyes, each eye examined three times). Data presented as n (%). Right eye, P < 0.001; left eye P = 0.005; Cochran–Mantel–Haenszel test.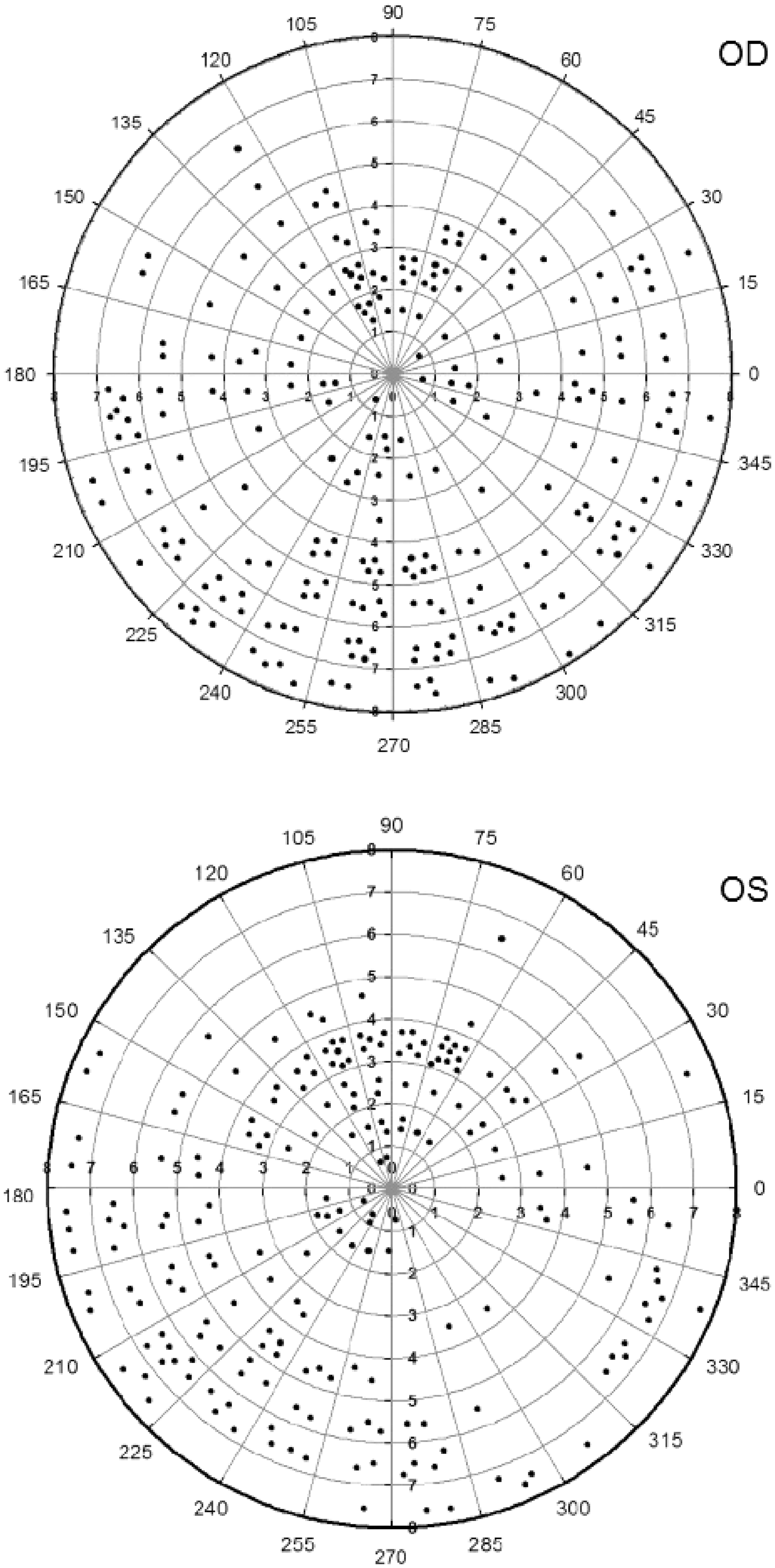
Discussion
There is a lack of consensus regarding noninvasive BUT measurement methodologies, with some studies indicating that NITBUT results in significantly higher values than TBUT,16,32,33 while a tearscope-based study found no significant difference. 22 Studies using the Keratograph 4 have resulted in shorter NIBUT than those determined using tearscope, however. 34 In this study, there was no significant difference between TBUT and NIKav-BUT, but TBUT and NIKf-BUT were significantly different, with the mean NIKf-BUT being 1.33 s shorter than the mean TBUT. This may be because the Keratograph 4 is capable of recording small and transient break-up areas that may not be visible to the eye.
Eye drops (such as ARTs) are often used both pre- and postoperatively in patients with cataracts, but there are no treatment guidelines available. Preoperative NIKf-BUT assessment via Keratograph 4 would allow identification of those patients at risk of developing postoperative dry eye who would benefit from ART treatment.
The precorneal surface is not evenly distributed and displays dynamic changes over time.35,36 Tear break-up has been shown to occur most frequently in the temporal and inferior areas37,38 and the inferior periphery of the cornea. 39 Thinner tear films have been reported to break-up earlier than thicker regions. 40 The tear film is known to thicken superiorly, to be uniformly distributed in the central region and to thin inferiorly.29,41 In the present study, the Keratograph 4 was used to record dynamic video throughout the interblink period (Figure 1, left panel), during which time increasing numbers of break-up units appeared. This dynamic process was represented in a single plot (Figure 1, upper right panel), which indicated the locations and break-up time of each break-up unit.
In the present study, the majority of first break-up areas occurred in the peripheral domain of the inferior precorneal surface (181–360°) and the central domain of the superior portion (61–120°); in most areas, the total first break-up units were >10%. This pattern may be explained by the following: (i) the effect of surface tension, which overpowers gravity after the blink; 42 (ii) the continuous secretion of tears from the upper lid; (iii) looseness of the eyelid in elderly patients, leading to evaporation in the lower domains. These findings differ from those of others, who determined that ocular surface height increased at the superior region over time.43,44 This may be due to the fact that the Keratograph 4 determines tear film breakage via thickness measurements, rather than height changes. In addition, the findings of our study may be different because the participants were cataract patients, in whom visual acuity and visual quality are relatively low because of their opacified lenses. Consequently, some patients may open their eyes more widely, thereby putting in additional effort to see clearly, and in turn this might change the tear-film distribution. We also acknowledge that the sample size in our study was not large and this may account for differences in the findings of the present study compared with other research. The findings of our research were simply descriptive observations. In our research, the diagnosis of dry eye was still made by establishing the tear-film break-up time, not by measuring the tear film break-up area. Our team plans to conduct additional research and obtain further evidence of the predictive and clinical value of Keratograph 4 examinations.
In conclusion, the determination of NIKf-BUT and NIKav-BUT via Keratograph 4 may be useful for predicting surgically induced dry eye and directing eye-drop intervention. This noninvasive methodology displays an intuitively colour-coded tear break-up map, enabling effective preoperative evaluation of tear film break-up regularity, informing the location of the incision, and reducing the probability of postoperative dry eye. Routine preoperative Keratograph 4 assessment of patients with cataracts may ultimately enhance visual quality.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the Project of the excellent academic leaders of Shanghai (No. 11XD1401200) and by the Project of the Nature Science Foundation of Shanghai (No. 11ZR1406100).