
Abstract
Objective
This study investigated the relationship between potential prognostic parameters that may be associated with increased inflammation and survival in patients with malignant mesothelioma (MM).
Methods
This retrospective study assessed potential prognostic parameters measured at the time of MM diagnosis. Data on asbestos exposure, histopathological subtype of MM and laboratory parameters were collected.
Results
In 155 patients with MM (90 male), mean survival time was 13.9 months. In univariate analysis, age ≥60 years and neutrophil-to-lymphocyte ratio (NLR) ≥3 were associated with significantly shortened median survival times. In multivariate analysis, nonepithelial subtype, red cell distribution width (RDW) ≥20% and NLR ≥3 were associated with significantly shortened median survival times. Mortality rate was increased 2.77-, 1.67- and 1.52-fold in patients with RDW ≥20%, NLR ≥3 and nonepithelial subtype, respectively. Nonepithelial subtype, white blood cell count ≥11 200 µl and platelet-to-lymphocyte ratio ≥300 at baseline were associated with a heightened NLR value.
Conclusions
The NLR and RDW were significant predictive factors for MM prognosis.
Introduction
Malignant mesothelioma (MM) is a tumour with increasing incidence; 1 it is highly prevalent in the southeast region of Turkey because of environmental asbestos exposure.2–4 Although several treatment options have been used in patients with MM, the disease has a poor prognosis, with a mean survival time of only 12 months.5–7
The European Organisation for Research and Treatment of Cancer (EORTC) and the Cancer and Leukemia Group B have devised two prognostic scoring systems for use in patients with MM,8,9 which are based on several signs and symptoms of the disease. However, these scoring systems are not routinely used in MM prognosis because they are time consuming to perform. Therefore, in patients with MM, parameters that are useful, easy to measure and inexpensive to administer are needed for predicting prognosis.
Local and systemic inflammatory responses are known to increase in patients with solid tumours, and are associated with prognosis.10–12 Importantly, inflammation plays a critical role in the development of MM. 13 Moreover, during the MM disease process, patients show signs of increased inflammatory responses such as fever, sweats and weight loss.14,15 Thus, markers of inflammation may have value in establishing the prognosis of patients with MM.
Studies have identified the neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR) as measures of systemic inflammation; they are relatively inexpensive to perform and provide readily obtainable (and reproducible) markers that may be prognostic factors in patients with MM.16–19 However, studies have shown conflicting results with NLR. For example, in one cohort of 30 patients with MM, NLR ≥5 was associated with poor MM prognosis. 20 In contrast, in 44 patients with MM treated with surgical procedures, NLR ≥5 was not found to be associated with MM prognosis. 21
Other potentially prognostic inflammatory markers are red cell distribution width (RDW) and mean platelet volume (MPV). RDW is a measure of the variability in the size of circulating erythrocytes, 22 and is routinely reported with complete blood count. Studies have suggested that RDW is increased in patients with cardiovascular and pulmonary diseases, with inflammation playing a key role.23–25 MPV reflects platelet size, which is correlated with platelet function and activation: elevated MPV predicts high platelet activity and intensity of inflammation. 26 MPV values have been investigated in chronic inflammatory diseases, and increased values have been associated with conditions such as familial Mediterranean fever.27,28 To our knowledge, no previous study has investigated the relationships between RDW or MPV and prognosis, in patients with MM.
The aim of the present study was to investigate the relationship between potential prognostic indicators (including NLR, PLR, MPV, RDW and other variables) and survival, in patients with MM.
Methods
Study design
This was a retrospective study conducted between 1 September 2012 and 1 December 2012, using data obtained prior to treatment and held in patients’ files. Local ethical approval was obtained from the Dicle University Medical Faculty Ethics Committee for Noninterventional Studies.
Patients
Eligible patients had MM that was diagnosed between November 2003 and November 2012. MM was confirmed histopathologically. Pathological diagnosis was obtained on biopsies, in line with recent international guidelines. 29 Asbestos exposure type and time, location of MM, histopathological subtype of MM and basic laboratory parameters were obtained from patients’ files held at the Research Hospital at Dicle University. Patients (or their next of kin) provided written informed consent for the data to be published.
Potential prognostic parameters
Details on the following potential prognostic parameters, measured at the time of diagnosis, were obtained from patients’ files: age <60 or ≥60 years; 5 sex; histopathological subtype of MM (epithelial or nonepithelial); haemoglobin level <10 g/l or ≥10 g/l; 17 serum lactate dehydrogenase (LDH) level <500 U/l or ≥500 U/l;5,9 platelet count <420 × 103/µl or ≥420 × 103/µl; 5 white blood cell (WBC) count <11 200/µl or ≥11 200/µl. 5 LDH level was determined in serum using heparin and citrate and an autoanalszer, (Architect 1600c, Abbott Laboratories, Irving, TX, USA). LDH level was measured in tubes with K2 ethylenediaminetetra-acetic acid. Haemogram parameters (including WBC, haemoglobin, platelet count, neutrophil and lymphocyte counts) were measured using Cell-Dyn 3700 (Abbott Diagnostics, Lake Forest, IL, USA).
Assays were performed within 1 h of collection, after centrifugation of the paired specimens (1500
Assessment of the value of potential prognostic parameters
Univariate and multivariate analyses were used to investigate the relationship between MM prognosis and the following 11 potential factors: age; sex; histopathological subtype; platelet count; WBC count; serum LDH level; NLR; PLR; MPV; haemoglobin level; RDW.
Statistical analyses
The mean ± SD values were obtained for continuous variables and χ2-test was used to examine categorical variables. Duration of survival and median and mean event times, with 95% confidence intervals (CI), were estimated according to the Kaplan–Meier method. Median values were used in our definition of the cut-off limits. Duration of survival was defined as the period between time of diagnosis and time of death. If patients were still alive, survival was defined as the period between time of diagnosis and 1 November 2012.
Cox proportional hazards regression model, with stratification for the clinical trial, was used for both the univariate and multivariate analyses. The univariate analysis examined the prognostic importance of all the aforementioned factors and the model was used to examine the variables. A two-sided test was used, with a 0.05 level of significance. Comparisons of overall survival were made using two-tailed log-rank tests. Only variables with P-values <0.10 in the univariate analysis were included in the final model for the multivariate analysis.
In the Cox regression analysis, the backward conditional method was used. Significance was taken as P < 0.05. Statistical analyses were performed using SPSS®, version 15 (SPSS Inc., Chicago, IL, USA).
Results
Patients
Information on basic laboratory parameters was available for 198 patients with MM. Of these, 36 patients were excluded from the study due to lack of sufficient data, and a further seven patients were excluded due to the presence of active infection and other comorbidities (chronic obstructive pulmonary disease, lung cancer, interstitial lung disease, pneumoconiosis). This left a study group of 155 patients with MM, of whom 32 were alive at the time of the study; the mean follow-up period was 13.9 months. The types of data available for analysis varied considerably, depending on the information retained in individual patient records.
Patients had a mean ± SD age of 58.2 ± 11.9 years; 90 (58.1%) patients were male and 65 (42.0%) were female. There was limited information in the patient records on aspects such as comorbidities, treatment regimens and specific clinical findings. A total of 139 (89.7%) patients had pleural MM, 19 (12.3%) had peritoneal MM and one (0.6%) had pericardial MM; the numbers of peritoneal and pericardial MM were too low for statistical analysis. One hundred (64.5%) patients had epithelial subtype MM; six (3.9%) patients had sarcomatous subtype, six (3.9%) patients had mixed subtype and the subtype was unidentified in 43 (27.7%) patients. Environmental asbestos exposure was present in 100 (64.5%) patients and the mean exposure time in these patients was 31.2 years.
Neutrophil-to-lymphocyte ratio values were 0.50–10.50 (median 2.9). For other variables, PLR values were 59.40–576.27 (median 166.87), RDW values were 10.65–26.50 (median 16.0) and MPV values were 5.69–11.40 fl (median 7.81 fl).
The mean ± SD survival time was 13.9 ± 11.3 months.
Potential prognostic parameters
Univariate and multivariate analyses results for potential prognostic parameters in patients with malignant mesothelioma (MM).

Observed death n/total patient n;
Median survival (months).
CI, confidence interval; HR, hazard ratio; LDH, lactate dehydrogenase; MPV, mean platelet volume; NLR, neutrophil-to-lymphocyte ratio; NS, not significant; PLR, platelet-to-lymphocyte ratio; RDW, red cell distribution width; WBC, white blood cell.
Cox proportional hazards regression model.
Both the univariate and multivariate analyses revealed no associations between survival time and PLR ≥ 300, MPV ≥8 fl, LDH level ≥500 U/l, platelet count ≥420 × 103/µl, WBC count ≥11 200/µl or haemoglobin level ≥10 g/l.
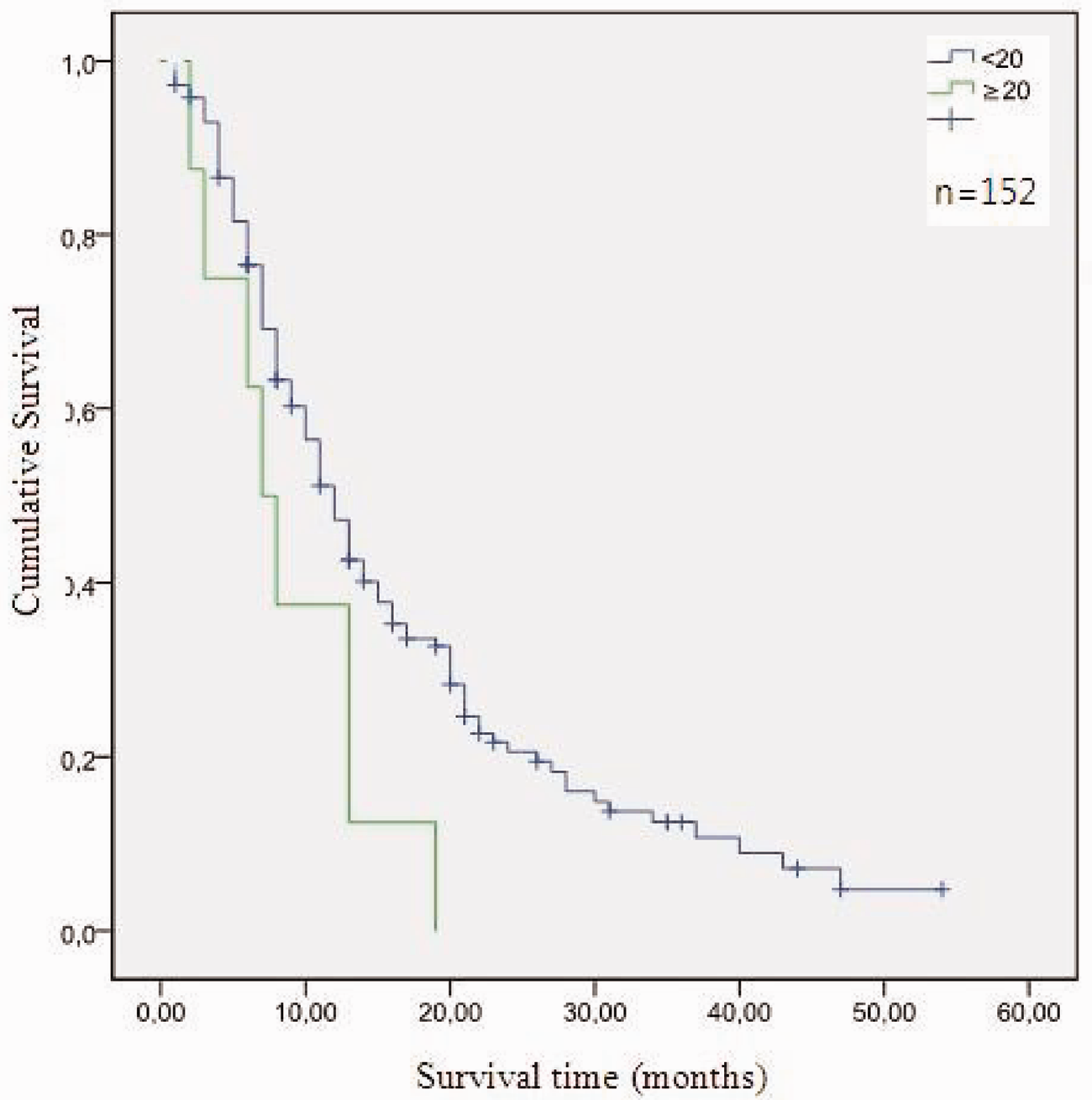
When the impact of other factors was excluded, RDW ≥20% was associated with an increased mortality rate of 2.77-fold in patients with MM, an NLR ≥3 with an increased mortality rate of 1.67-fold and a nonepithelial subtype with an increased mortality rate of 1.52-fold. Survival curves for patients according to histopathological subtype (epithelial or nonepithelial), RDW (<20% and ≥20%) and NLR (<3 and ≥3) are presented in Figures 1–3; the number of patients with data available for each analysis varied.
Kaplan–Meier survival curves according to histopathological subtype (epithelial and nonepithelial) in 155 patients with malignant mesothelioma (MM). When the impact of other factors was excluded, patients with a nonepithelial subtype (n = 55) had a significantly increased mortality rate of 1.52-fold versus patients with an epithelial subtype (n = 100) (P < 0.010; Cox proportional hazards regression model). The colour version of this figure is available at http://imr.sagepub.com. Kaplan–Meier survival curves according to red cell distribution width (RDW) (<20% and ≥20%) in 149 patients with malignant mesothelioma (MM). When the impact of other factors was excluded, patients with RDW ≥20% (n = 9) had a significantly increased mortality rate of 2.77-fold versus patients with RDW <20% (n = 143) (P < 0.010; Cox proportional hazards regression model). The colour version of this figure is available at http://imr.sagepub.com. Kaplan–Meier survival curves according to neutrophil-to-lymphocyte ratio (NLR) (<3 and ≥3) in 149 patients with malignant mesothelioma (MM). When the impact of other factors was excluded, patients with NLR ≥3 (n = 67) had a significantly increased mortality rate of 1.67-fold versus patients with NLR <3 (n = 82) (P < 0.010; Cox proportional hazards regression model). The colour version of this figure is available at http://imr.sagepub.com.

Association between baseline characteristics and prognostic parameters
Baseline characteristics of patients with malignant mesothelioma (MM) based on neutrophil-to-lymphocyte ratio (NLR n = 149).
LDH, lactate dehydrogenase; MPV, mean platelet volume; NLR, neutrophil-to-lymphocyte ratio; NS, nonsignificant; PLR, platelet-to-lymphocyte ratio; RDW, red cell distribution width; WBC, white blood cell.
χ2-test.
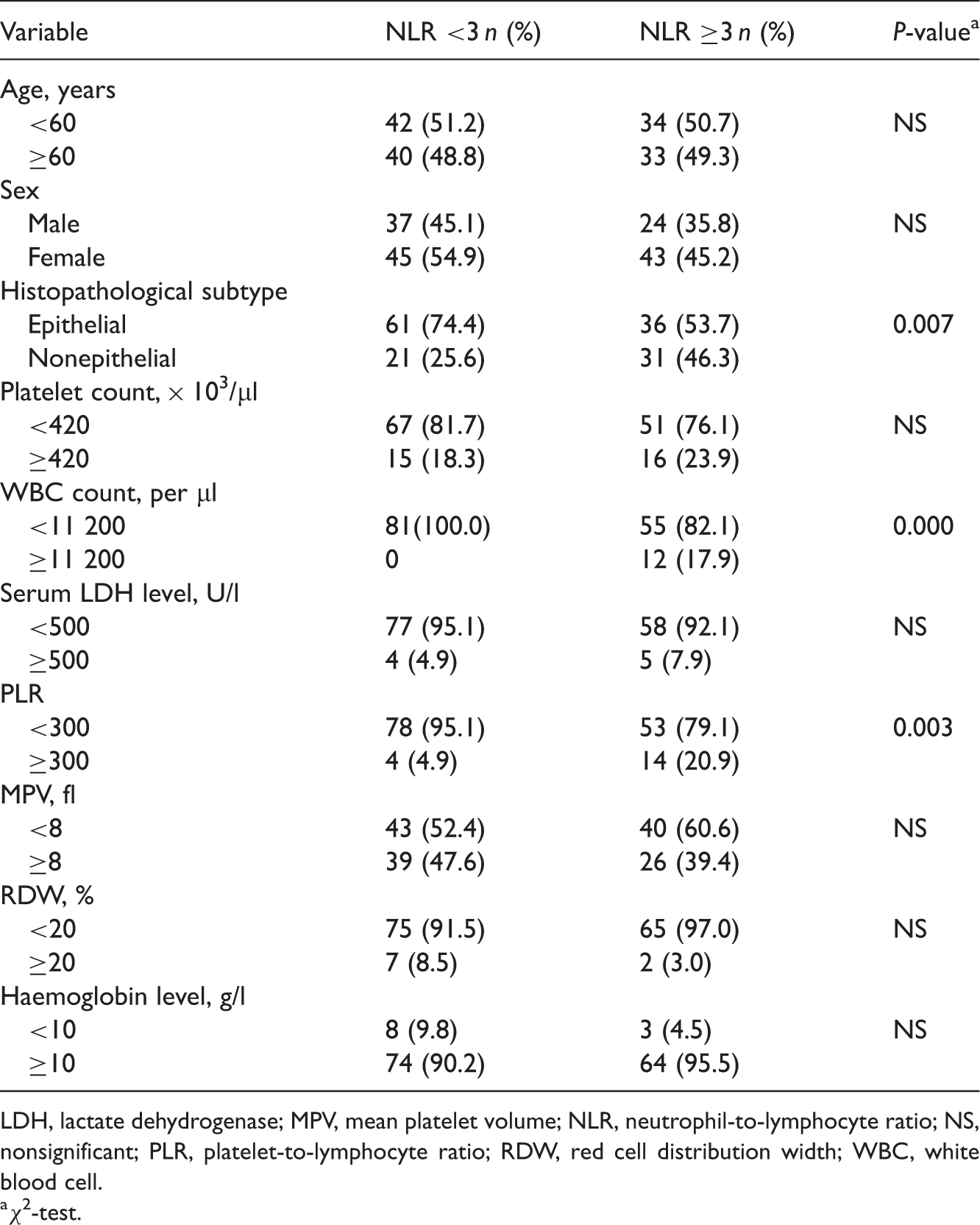
Baseline characteristics of patients with malignant mesothelioma (MM), based on red cell distribution width (RDW; n = 152).

LDH, lactate dehydrogenase; MPV, mean platelet volume; NLR, neutrophil-to-lymphocyte ratio; NS, nonsignificant; PLR, platelet-to-lymphocyte ratio; RDW, red cell distribution width; WBC, white blood cell.
χ2-test.
Discussion
The EORTC and the Cancer and Leukemia Group B analysed large numbers of patients with MM and identified the following poor prognostic factors:8,9 nonepithelioid histology; poor performance score; presence of chest pain; age >75 years; male sex; WBC count ≥8.3 × 109/l; platelet count >400 000/μl; LDH >500 U/l. In the present univariate analysis there was a significant association between age >60 years and poor prognosis for MM. The patient cohort in the present study was stratified at 60 years, given the low mean age of our study group (58 years) and the short survival duration; few of our patients reached 75 years of age, despite this being considered as the threshold for poor prognosis in the international recommendations.8,9
Inexpensive and easily detected prognostic parameters have not yet been developed for MM. Therefore, the present retrospective study investigated the relationship between potential prognostic indicators and survival in 155 patients with MM.
In countries where people are exposed to asbestos through industrial practices, rates of MM are generally higher in men than in women. This is because men are more likely to work for longer time periods in such industries and are therefore more likely to have higher lifetime asbestos exposure rates. However, in our region, asbestos exposure is mostly environmental and begins at birth; it affects both sexes almost equally, because it is processed with water and people are exposed via inhalation, in home environments. Some studies in our region have found male : female ratios of MM as close as 1.3–1.48.3,5 In our study, the ratio was 1.38.
In our region MM is probably detected at lower ages than those observed elsewhere as a consequence of the high rate of environmental exposure described above. In one study performed in our region, the mean age of patients was 56 years. 30 The mean age of MM patients in our study is also relatively low, probably as a result of the regional environmental asbestos exposure.
The mean survival time was 13.9 months. Of 11 potential prognostic factors assessed, the inflammatory markers NLR ≥3 and RDW ≥20% (in addition to the nonepithelial subtype), were effective indicators of MM prognosis in the multivariate analysis. Other markers (such as age, sex, LDH level, platelet count and WBC count) were not found to be prognostic indicators of MM.
Studies have reported that the rate of mortality increased 1.79–2.20-fold in patients with MM with NLR ≥3 versus <3, and that this difference was statistically significant.17,19 Unal et al. found that pretreatment NLR measurements provided important prognostic results in patients with nonsmall cell lung cancer. 31 In other studies, the rate of mortality in patients with MM was increased 2.00–2.70-fold with NLR ≥5 versus <5; this difference was also statistically significant.16,18 Cedrés et al. 20 found that NLR ≥5 was an independent prognostic factor in patients with MM. In the present study, the rate of mortality increased 1.67-fold in patients with MM who had an NLR of ≥3 compared with NLR <3; mean duration of survival was 10.5 months in those with an NLR ≥ 3 and 14.9 months in those with an NLR <3. The NLR may, therefore, be viewed as an inexpensive predictor of MM prognosis at the time of diagnosis, and we postulate that the NLR level could be a factor to use as part of the decision making process, when considering aggressive or palliative treatment regimens for patients with MM. It is reasonable to assume that patients with MM with more advanced disease at the time of diagnosis may have a more excessive systemic inflammatory response and, therefore, a higher NLR.
The histological subtype is well established in predicting prognosis in MM and many studies have found that the nonepithelial histological subtype is associated with a poor prognosis.9,16,17 The multivariate analysis in the present study also confirmed this finding: the mortality rate increased 1.52-fold in patients with a nonepithelial subtype of MM.
In complete blood count data, the RDW has been found to be increased in several inflammatory diseases.24,32,33 However, the association between a high RDW and overall prognosis in MM has not been widely investigated. In one investigation of patients with pulmonary embolism, RDW >15% was found to be a prognostic parameter in multivariate analysis, and RDW >15% increased the mortality rate 1.2-fold. 34 In another study of patients with community-acquired pneumonia, the 30-day mortality rate was significantly higher in those with a greater RDW. 35 In our study, mortality rates in patients with MM increased 2.77-fold in those with RDW ≥20% versus <20%, and the mean survival time was 8 months in those with RDW ≥20%, compared with 13.9 months in those with RDW <20%: a difference that was statistically significant. This result may be due to the association between RDW and increased inflammation, and to chronic inflammation playing a key role in the development of MM.
In our study, RDW ≥20% was associated with histopathological subtype and platelet count, whereas NLR ≥3 was associated with histopathological subtype, WBC count and PLR. These findings may be due to the associations between histopathological subtype, WBC count, platelet count and PLR, and poor prognosis of MM.8,9,18
A limitation of our study is its retrospective nature, which focused on pretreatment information obtained from patients’ files. Moreover, treatment regimens and their outcomes were unavailable, since patient management was conducted in other clinics, such as oncology clinics, or in thoracic surgery. Another limitation is that we only became aware of the guidelines outlined by the REMARK initiative 36 after we had undertaken the present study. As our study was retrospective, the patient data did not consistently include information on disease stage, comorbidities, performance status, chest pain, treatment regimens and other detailed results (which are recommended in the REMARK guidelines). Where possible, however, we had applied other recommendations of the REMARK initiative.
In conclusion, the pathological role of chronic inflammation in the development of MM is well established. 13 Based on our results, inflammatory-based biomarkers may be predictive of survival. NLR, as an index of systemic inflammation, may be independently associated with survival in patients with MM. Both the NLR and the RDW may be useful prognostic markers: they are easily obtainable and were significant predictive factors for MM prognosis. The inexpensive nature and reproducibility of the complete blood count, which includes both NLR and RDW, should encourage their use in the clinical management of patients with MM. Both parameters may help in making the decision between aggressive or palliative treatment regimens.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.