
Abstract
Background
Percutaneous kyphoplasty is a popular technique in the treatment of osteoporotic vertebral fractures, but intracardiac cement embolism can be a life-threatening complication.
Conclusions
The present case highlights that surgical removal may be the first-choice treatment for symptomatic intracardiac cement embolism.
Keywords
Introduction
Percutaneous kyphoplasty and vertebroplasty are minimally invasive surgical techniques that are widely used to treat osteoporotic vertebral compression fractures and spinal metastases.1,2 However, percutaneous kyphoplasty is associated with multiple complications due to leakage of polymethylmethacrylate (PMMA) cement into the perivertebral venous system. The rate of venous cement embolism complications reportedly ranges from 2.1% to 26.0%.3,4 The cement first enters the heart chambers and may further migrate into the pulmonary arteries, which can cause life-threatening complications. We herein report a case of post-kyphoplasty intracardiac and pulmonary cement embolisms that caused cardiac perforation and pericardial tamponade, resulting in severe cardiopulmonary complications.
Case report
A woman in her early 80s was hospitalized because of persistent severe back pain. One month earlier, she had experienced an accidental fall. The patient was 155 cm tall, weighed 62 kg, and had a body mass index of 25.8 kg/m2. She had a history of hypertension. Radiography and magnetic resonance imaging confirmed a compression fracture of the L4 and L5 vertebral bodies. The T-value measured by dual-energy X-ray absorptiometry was −3.3, which indicated osteoporosis of the lumbar spine. Percutaneous kyphoplasty was performed via a unilateral transpedicular approach with a 13-gauge needle under local anesthesia. Using fluoroscopic guidance, the prepared cement was injected into the L4 and L5 vertebral bodies, and the injected cement volume reached approximately 4.0 mL for each vertebra. No extravasation of bone cement was observed on either anteroposterior or lateral fluoroscopy. The patient’s back pain was soon relieved, and she was discharged from the hospital 3 days after surgery.
Two months later, the patient developed dyspnea and chest tightness. No signs of myocardial ischemia were found on an electrocardiogram, and a heart murmur was auscultated during the physical examination. Laboratory tests showed remarkably elevated D-dimer and myocardial enzyme concentrations. Transthoracic echocardiography showed a foreign body with calcium density in the right atrium (Figure 1). Therefore, we suspected that the patient had developed an intracardiac embolism. Chest computed tomography confirmed the existence of foreign bodies in the right atrium with perforation of the atrial wall, causing pericardial tamponade. Several high-density materials in the left pulmonary artery and right lower lobe pulmonary artery were also observed (Figure 2).
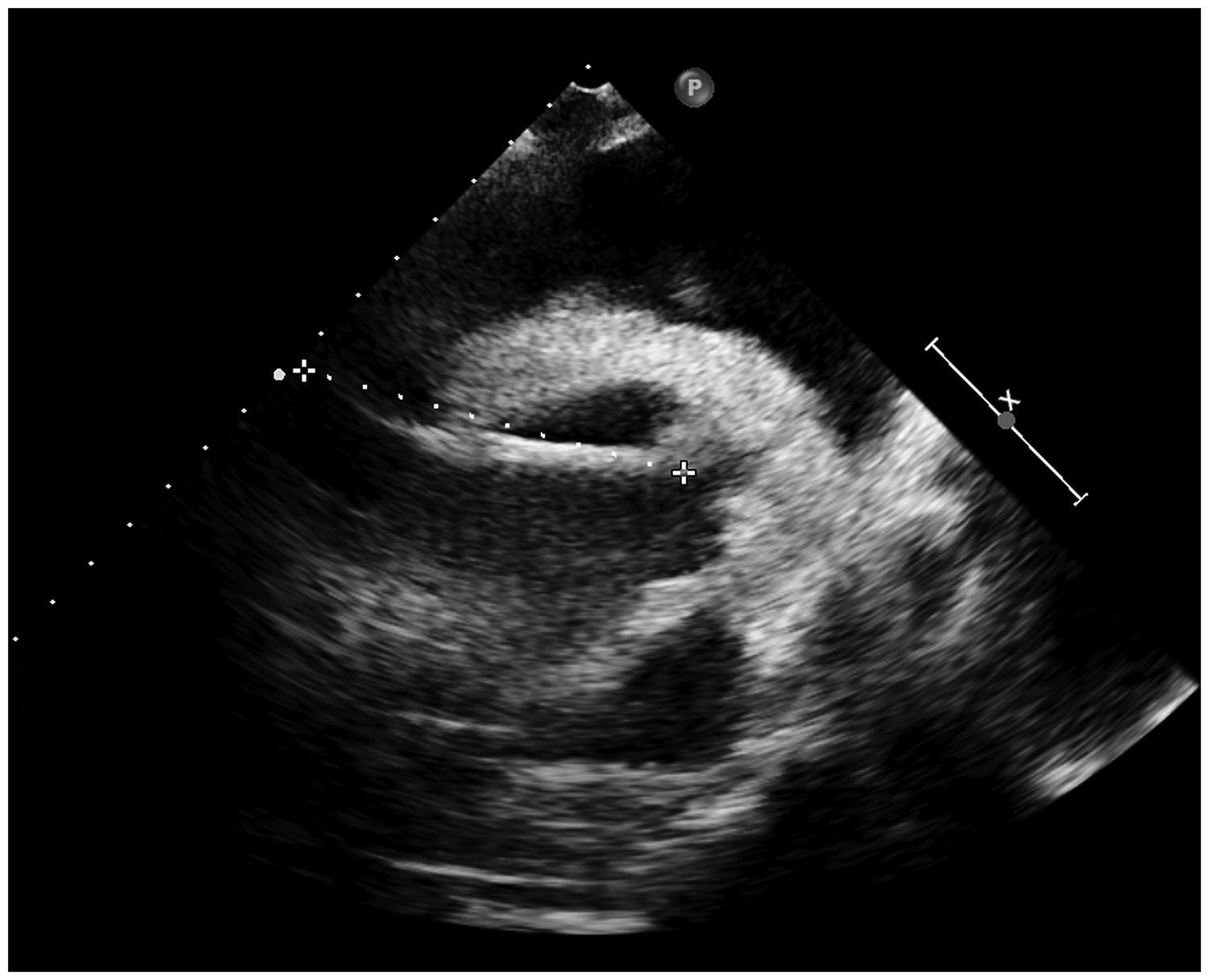
Echocardiographic finding of a linear foreign body in the right atrium (dotted line; length = 73 mm).

Images of intracardiac and pulmonary cement embolism. (a) Computed tomography showed high-density foreign bodies in the right atrium (red arrow) resulting in pericardial tamponade (blue arrow) and (b, c) Cement embolisms were present in the left pulmonary artery and right lower lobe pulmonary artery (red arrow).
After obtaining the patient’s consent for treatment, she was promptly treated with low-molecular-weight heparin and oxygen. Urgent pericardial drainage was performed with aspiration of 300 mL of bloody fluid. The patient’s blood oxygen saturation decreased to 83%, and she was treated with respiratory support. Cardiology specialists were consulted immediately, and the treatment options were discussed. We decided to perform open surgery to remove the cement emboli from the right atrium and pulmonary artery. However, the patient refused surgical removal. Five days after admission, the patient developed atrial fibrillation and pneumonia that was unresponsive to antibiotic therapy. She died of cardiac and respiratory failure 7 days after admission. The reporting of this study conforms to the CARE guidelines. 5
Discussion
Kyphoplasty is a technique that involves the injection of PMMA bone cement into the compressed vertebral body to mechanically stabilize the fracture. Reported complications of kyphoplasty include infection, adjacent level fracture, central canal stenosis, and pulmonary embolism. 6 Among the various complications, cement leakage is relatively common. It may cause local complications such as central canal stenosis and systemic complications including pulmonary embolism and intracardiac embolism. The rate of venous cement embolism as a complication of kyphoplasty is reportedly as high as 65%. 7 The bone cement enters the right heart chambers and may further migrate into the pulmonary arteries. PMMA is a foreign object and cannot be absorbed by the human body. Because of its irregular shape and porous surface, PMMA is considered potentially thrombogenic. 8 In most patients, the cement pieces are small and scattered, and the embolisms can be clinically insignificant. In some patients, however, the embolisms may change the hemodynamic status and lead to fatal consequences. 9
Intracardiac embolism of bone cement secondary to vertebroplasty and kyphoplasty is a potentially serious complication. The reported incidence of intracardiac embolism is 3.9%. 10 The most common symptoms of intracardiac embolism are chest pain and dyspnea. The onset of symptoms may be days, months, or even years after surgery. Most bone cement is located in the right atrium and right ventricle. However, several reports have described penetration of the heart wall by the cement, resulting in cardiac perforation,9,11,12 whereas involvement of the tricuspid valve can result in tricuspid regurgitation.13 –16 In the present case, we presumed that the PMMA had stayed in the right atrium after the procedure. As the heart continued to beat, the PMMA eventually penetrated the right atrial wall and caused pericardial tamponade.
In terms of treatment, most reported cases of symptomatic intracardiac embolism were treated with open surgery (Table 1), especially in patients with tricuspid valve injury and cardiac perforation. Percutaneous retrieval is an alternative minimally invasive procedure to remove the cement, but potential complications such as further thrombus fragmentation and distal embolization need to be fully recognized. 17
Literature review of intracardiac embolism due to kyphoplasty or vertebroplasty.
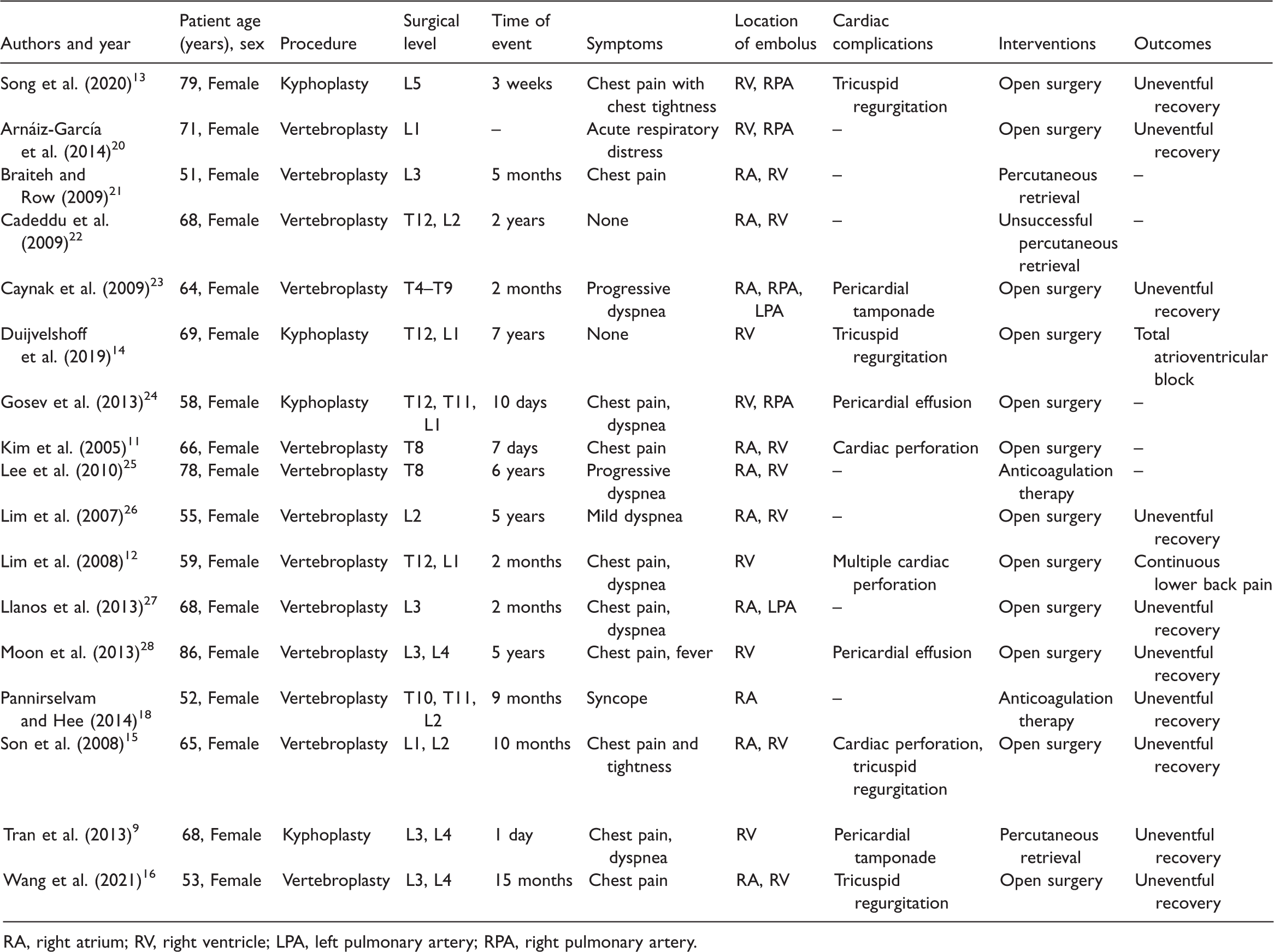
RA, right atrium; RV, right ventricle; LPA, left pulmonary artery; RPA, right pulmonary artery.
Few reports have addressed conservative treatment for intracardiac embolism of bone cement. Pannirselvam and Hee 18 described a patient who presented with syncope after vertebroplasty. Echocardiography showed a 2.8-cm foreign body in the right atrium. The patient was treated with anticoagulation therapy and had no further symptoms, including syncope; thus, there was no need for additional interventions. Liang et al. 19 suggested that cardiopulmonary embolism should be managed by conservative treatment under close monitoring. In patients who develop mild clinical manifestations with a stable hemodynamic status, conservative treatment including anticoagulation, continuous low-flow oxygen inhalation, and antibiotics can be an option.
There are no clear criteria for how severe an intracardiac cement embolism must be before surgery is required. Hatzantonis et al. 17 suggested that surgical removal should be considered for patients with symptomatic intracardiac embolism. The decision about whether to attempt percutaneous retrieval or open surgery should be based on careful consideration of a number of clinical issues, including the precise location and size of the embolism and the presence of any cardiac complications.
Conclusion
Intracardiac cement embolism following percutaneous kyphoplasty is a rare but life-threatening complication. Surgical removal may be the first-choice treatment for symptomatic intracardiac embolism.
Footnotes
Author contributions
Huang Chunneng drafted and edited the manuscript.
Declaration of conflicting interests
The author declares that there is no conflict of interest.
Ethical statement
All patient details have been de-identified. Verbal consent for publication was obtained from the patient’s son, and the consent for publication was approved by the Institutional Review Board of Hangzhou First People’s Hospital.
Data availability statement
This is a case report of one patient. To protect the patient’s privacy and respect her confidentiality, none of the raw data are available in any public repository. The original reports, laboratory studies, imaging studies, and clinical records are retained as per normal procedure within the medical records of our hospital.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Science and Technology Project of Zhejiang Province (grant number: 2019RC238).