
Abstract
Objective
To determine the relationship between arterial distensibility and hypothyroidism by simultaneous assessment of coronary angiography and aortic distensibility, measured using 128-slice retrospective electrocardiogram-gated multiple row detector computed tomography (MDCT).
Methods
Untreated hypothyroid patients and age-matched euthyroid patients, who underwent 128-slice retrospective electrocardiogram-gated MDCT to evaluate the coronary arteries, were assessed. Intraluminal aortic areas in systolic and diastolic phases of the cardiac cycle were measured with multiphase reformation at predefined locations including the ascending aorta, proximal descending aorta and distal descending aorta in the widest axial plane.
Results
The study included 21 hypothyroid and 21 euthyroid patients. Patients with hypothyroidism exhibited decreased aortic distensibility between each location in the thoracic aorta (ascending aorta, proximal descending aorta and distal descending aorta) compared with euthryoid patients.
Conclusions
Hypothyroidism was associated with preclinical vascular alteration, characterized by impaired aortic distensibility at each location of the thoracic aorta, which has been shown to be related to increased cardiovascular risk. Monitoring of aortic distensibility is relevant for evaluating coronary artery disease progression and treatment choices.
Keywords
Introduction
Hypothyroidism is thought to be a strong risk factor for developing atherosclerosis, and can lead to coronary artery disease and aortic atherosclerosis.1,2 The interaction between atherosclerosis and hypothyroidism, however, remains unclear. 3 In patients with hypertension, it has been shown that despite the presence of intact vasculature, arterial function may be abnormal. 4 Aortic distensibility, which relates to the degree of contraction and expansion of the aorta, is a property of the vascular wall itself: it is affected by several factors and is related to hypothyroidism.3,5
Simultaneous evaluation of the coronary angiogram and aortic elasticity is important to estimate the risk of developing coronary artery disease, 4 with aortic distensibility emerging as a useful predictor of coronary artery disease risk. 6 The thoracic aorta is easily accessible by 128-slice multiple row detector computed tomography (MDCT) during coronary angiograms, and MDCT has been shown to provide an objective calculation of aortic distensibility. 7 Increased carotid arterial stiffness has been reported in hypothyroid patients.3,8 However, there is little information regarding aortic distensibility measured using MDCT and its clinical significance in hypothyroidism.
Aortic distensibility can be objectively measured using MDCT or magnetic resonance imaging at any point along the thoracic aorta, and changes in distensibility in both the ascending and descending aorta have been shown in patients with atherosclerosis.9,10 Aortic distensibility has also been shown to be inversely proportional to severity and presence of coronary artery disease.11,12 With improved temporal and spatial resolution, 128-slice MDCT with retrospective electrocardiogram-gating allows accurate visualization of small- and large-calibre vasculature and their contractility throughout the cardiac cycle.13,14 Data relating to MDCT-measured aortic distensibility and coronary artery disease using single imaging modality are lacking. The aim of the present study was to compare aortic distensibility between hypothyroidism and euthyroidism using single-source MDCT as a high spatial resolution and objective imaging technique.
Patients and methods
Study population
This retrospective case–control study included female patients with untreated primary hypothyroidism and negative coronary angiograms, and euthyroid female patients, matched for age and body mass index (BMI), with negative coronary angiograms, who presented at the Department of Radiology, Uludag University, Bursa, Turkey, between May 2010 and May 2011. Patients were enrolled sequentially into the study. Patients with atherosclerosis, diabetes mellitus, hypertension, severe obesity (BMI > 35 kg/m2), renal failure, cerebrovascular disease, malignancy, severe lung disease, the metabolic syndrome, allergies, or who smoked, were receiving hormone replacement therapy or were male, were excluded from the study. The study protocol was approved by Uludag University School of Medicine Ethics Committee (reference no. 2011-10/2) and written informed consent was obtained from all participants. The study complied with the Declaration of Helsinki.
Biochemistry
Blood samples were drawn from antecubital veins immediately prior to performing MDCT following an overnight fast. Samples were allowed to clot for 30 min at room temperature, then centrifuged at 2683
Multiple row detector computed tomography imaging
MDCT was performed using a coronary artery imaging protocol on a 128-slice MDCT (SOMATOM® Definition AS+; Siemens Healthcare, Forchheim, Germany). Patients received 0.6 mg nitroglycerin sublingually and 5–20 mg metoprolol intravenously (i.v.) if the resting heart rate was >60 beats/min and if no contraindications were present. Breath-hold images were acquired at inspiration (rotation time, 330 ms; collimation, 32 × 0.6 mm) using 120 kV, 200 mA and retrospective electrocardiogram-tube modulation. To optimize coronary artery contrast enhancement, a test bolus of nonionic contrast media was used comprising 1.1 ml/kg iopromide i.v. (Ultravist 370 g/ml, Bayer Schering Pharma, Berlin, Germany). Reconstructions were produced using a retrospective electrocardiogram-gated MDCT technique, allowing a temporal resolution of 75 ms. Four coronary arteries were assessed per patient. Plaque detection within one or more coronary artery and characterization by MDCT was performed as previously described. 15 MDCT angiography images were reconstructed with filtered back projection: slice thickness, 0.6 mm; increment, 0.3 mm. The same raw data were transferred to an offline workstation, and images were reconstructed with the same slice thickness and increment.
Aortic distensibility
For aortic distensibility measurements, the multiphase reformation dataset was reconstructed at a 10% R–R interval (10 phases of the cardiac cycle) with 1.5 mm slice thickness and 1.5 mm increments of the axial images. For coronary plaque evaluation, a mean of three axial datasets per subject were reconstructed with a 512 × 512 pixel image matrix: slice thickness, 0.65 mm; increment, 0.4 mm. Aortic distensibility was calculated as previously described:
9
Representative images of retrospective electrocardiogram-gated 128-slice multiple row detector computed tomography of aortic distensibility. (a) oblique sagittal image with associated cross-sectional areas of (b) systolic and (c) diastolic phase aortic diameters. Scale bars, 25 mm. AA, ascending aorta; PDA, proximal descending aorta; DDA, distal descending aorta.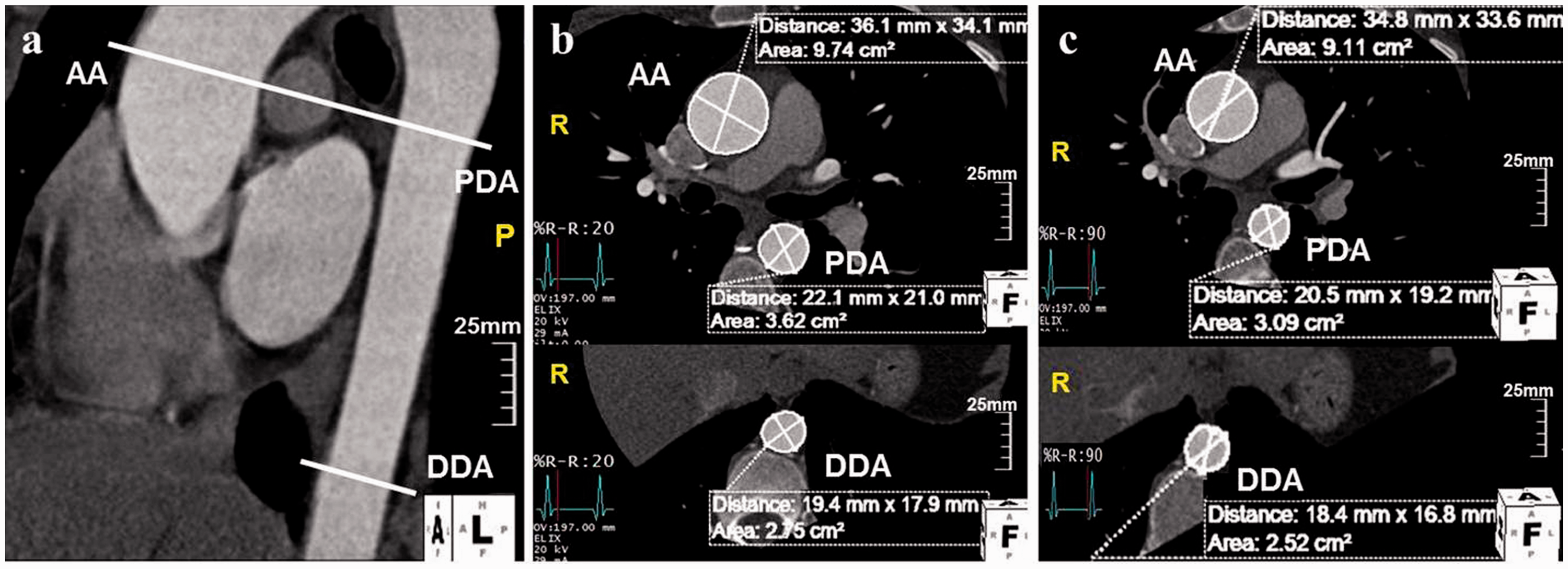
Two radiologists (A.D. and G.G.) performed the measurements on a dedicated offline workstation (QMass CT® version 7.1; Medis Medical Imaging Systems, Leiden, the Netherlands). The inter-observer reproducibility was determined by measurements of data from 10 randomly selected studies using the intraclass correlation coefficient (ICC).
Statistical analyses
Descriptive statistics are presented as mean ± SD for continuous variables and as frequency and percentages for nominal variables. Student’s t-test was used to compare normally distributed covariates. All analyses were performed using the SPSS® software package, version 18.0 (SPSS Inc., Chicago, IL, USA) for Windows®. A two-tailed P-value <0.05 was considered to indicate statistical significance.
Results
Characteristics of women with untreated primary hypothyroidism and negative coronary angiograms, and euthyroid women matched for age and body mass index, with negative coronary angiograms (control group) who underwent 128-slice multiple row detector computed tomography.

Data presented as mean ± SD.
NS, no statistically significant between-group differences (P ≥ 0.05); Student's t-test.
HDL, high-density lipoprotein; LDL, low-density lipoprotein; T3, triiodothyronine; T4, thyroxine; SBP, systolic blood pressure; DBP, diastolic blood pressure; ΔP, pulse pressure; AA, ascending aorta; PDA, proximal descending aorta; DDA, distal descending aorta.
The inter-observer ICC and intra-observer ICC for aortic distensibility measurements were 0.92 and 0.96, respectively. The distensibility of the ascending aorta, proximal descending aorta and distal descending aorta detected by retrospective electrocardiogram-gated MDCT was significantly decreased in patients with hypothyroidism compared with euthyroid controls (all P = 0.001, Table 1).
Discussion
Using retrospective electrocardiogram-gated MDCT, the present study revealed that hypothyroidism was associated with preclinical vascular alteration, supporting the findings of previous studies, in which hypothyroidism has been shown to be related to atherosclerosis and increased cardiovascular risk.2–6 Monitoring of aortic distensibility has been shown to be relevant for evaluating coronary artery disease progression and treatment choices.7–9
Previous investigations regarding hypothyroidism and atherosclerosis have yielded contradictory results. Some studies have shown increased risk of atherosclerosis, 3 while others found no effect on atherosclerosis in cases of hypothyroidism compared with patients with normal thyroid function. 19 Studies using echocardiography have suggested that patients with hypothyroidism have decreased central arterial distensibility.20,21 In addition, hypothyroidism has been associated with preclinical atherosclerosis, characterized by increased stiffness of the common carotid artery,3,8 and aortic distensibility in patients with hypothyroidism has been shown to be improved by thyroid hormone replacement treatment. 22
Altered arterial elasticity might be explained by altered lipid metabolism including serum cholesterol and LDL elevation in hypothyroid patients compared with euthyroid subjects.19,23,24 During recombinant TSH management, TSH has been shown to affect the arterial wall by impairing vasodilation. 3 Data in the present study also demonstrated a positive relationship between aortic distensibility and total cholesterol, LDL, T3, T4 and TSH levels.
The presence of hypothyroidism is a significant contributor to increased vascular stiffness and thus reduced aortic distensibility.1,2 The presence and extent of hypothyroidism has also shown to be a strong predictor of vascular morbidity and mortality.20,25 The effect of hypothyroidism on the vasculature has been proposed to occur at the early stage of atherosclerosis, where increased production and irreversible cross-linking of collagen fibres, and reduced levels of elastin contribute to impaired aortic distensibility.8,26
Hypothyroidism takes time to develop, and the driving force for the progression of atherosclerosis is thought to be associated with increased oxidative stress. 27 The present study showed a relationship between hypothyroidism and reduced aortic distensibility. The strength of the present study relies on the use of single imaging modality (contrast-enhanced electrocardiogram-gated MDCT) to demonstrate that aortic distensibility was reduced at the ascending aorta, proximal descending aorta and distal descending aorta.
The presence of hypothyroidism has been shown to be independently associated with reduced aortic distensibility in a population free of known coronary artery disease. 28 Disease in one vasculature may be indicative of disease in other vasculature. 9 Regardless of atherosclerosis location, the presence of atherosclerosis is associated with reduced aortic distensibility, and indicates higher cardiovascular event rates. 29 The strength of the present study came from the simultaneous finding of distensibility in the ascending aorta, proximal descending aorta and distal descending aorta as an early and objective marker of atherosclerosis, and evaluation of the coronary artery, using a single imaging modality. The ascending aorta, proximal descending aorta and distal descending aorta distensibility was found to be reduced by the presence of hypothyroidism, which implies an interaction between the biophysics of different vasculature.
The presence of hypothyroidism has been shown to have a strong independent association with decreased aortic distensibility 30 and is associated with worse cardiovascular outcomes compared with patients without hypothyroidism.25,29 This may have clinical implications and suggests that vascular disease with increased aortic distensibility is a symptom of hypothyroidism. It warrants more intensive medical therapy for vascular disease risks in patients with hypothryoidsm.22,31
The present study was limited by a number of factors. The study comprised a hospital-based cohort, with a limited number of cases. Acute-phase reactants and anti-thyroid antibodies were not measured, and the effect of hormone replacement treatment on aortic distensibility in hypothyroidism was not investigated.
In conclusion, the present study demonstrated that a more rigid, less distensible aorta is associated with atherosclerosis in hypothyroidism compared with euthyroidism. In addition, aortic distensibility was found to be related to increased cholesterol, LDL, T3, T4 and TSH levels. Hypothyroidism might be related to preclinical atherosclerosis, shown by decreased aortic distensibility. Due to the clinical importance of vascular alteration, the present study suggests that 128-slice electrocardiogram-gated MDCT systems are a useful imaging modality for simultaneously evaluating aortic distensibility in terms of cardiovascular risk. Further studies are needed to evaluate the effect of hormone replacement therapy on these pathophysiological and biophysical changes of the aorta in hypothyroidism.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflict of interests.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Acknowledgements
We gratefully acknowledge Ercan Tuncel, Gursel Savci and Naile B. Topal (Uludag University, Bursa, Turkey) for their editorial contributions.