
Abstract
Objective
To investigate the role of interleukin 6 (IL6) and IL16 single nucleotide polymorphisms (SNPs) in coronary artery disease (CAD) risk in a Chinese population.
Methods
Patients with CAD and healthy control subjects were recruited. IL6 (rs1800795 and rs1800796) and IL16 (rs8034928, rs3848180, rs4577037, rs1131445, rs4778889 and rs11556218) genotyping was performed on the MassARRAY® platform (Sequenom®, San Diego, CA, USA).
Results
Frequencies of rs8034928 variant C allele and rs11556218 variant T allele were higher in patients with CAD (n = 326) than controls (n = 341). The rs8034928 C/C genotype (odds ratio [OR] 2.03; 95% confidence intervals [CI] 1.16, 3.62) and C allele (OR 1.97; 95%CI 1.15, 3.45) were associated with increased risk of CAD compared with wild type. Similarly, the rs11556218 T/T genotype (OR 2.44; 95%CI 1.15, 5.44) and T allele (OR 2.37; 95%CI 1.13, 5.24) were associated with increased CAD risk compared with wild type.
Conclusion
The SNPs rs8034928 and rs11556218 are associated with CAD risk in the Chinese population, and may be useful predictive markers for CAD susceptibility.
Introduction
Coronary artery disease (CAD) is a major health problem worldwide, and has a complex aetiology determined by factors including inflammation, sex, age, smoking, hypertension, diabetes and genetic susceptibility.1,2 The underlying pathological process of CAD is atherosclerosis, which is characterized by chronic inflammation, due primarily to the deposit of oxidized lipids on the inner layer of the arterial wall. 2 Studies have indicated that inflammation-related genes may be associated with CAD risk.3–7
Elevated concentrations of interleukin 6 (IL6) and its final product, C reactive protein, are associated with increased CAD risk. 2 Interleukin (IL) 16 is a proinflammatory and immunoregulatory cytokine with multiple functions in the genesis and maintenance of the inflammatory response. It is produced by diverse cell types including fibroblasts, monocytes, adipocytes and endothelial cells. 8 Genetic variants of IL16 are associated with the risk of several cancers and autoimmune diseases.9–11 Studies investigating the relationship between CAD risk and IL6 or IL16 single nucleotide polymorphisms (SNPs) are inconclusive, however. The IL6 SNPs 174 G > C (rs1800795) and 572 G > C (rs1800796), in addition to IL16 270 T > C (rs8034928), have been shown to be associated with CAD risk,12,13 but a meta-analysis revealed no association between IL6 174 G > C (rs1800795) and CAD risk, 14 and no relationship was found between CAD risk and IL6 or IL16 polymorphisms in three large sample studies.10,12,13 The aim of the present study was to investigate the relationships between SNPs of IL6 (rs1800795 and rs1800796) and IL16 (rs8034928, rs3848180, rs4577037, rs1131445, rs4778889 and rs11556218) and CAD risk, in a Chinese population.
Patients and methods
Study population
This case–control study recruited patients first diagnosed with CAD at the Department of Cardiology, Beijing Chaoyang Hospital, Beijing, China, between February 2008 and December 2011. Inclusion criteria were angiographic evidence of ≥70% stenosis of one major coronary artery, or ≥50% stenosis of the left main coronary artery. Exclusion criteria were: current heparin treatment; autoimmune disease; congenital heart disease; severe kidney or liver disease; malignancy.
Age-matched control subjects were recruited from individuals attending Beijing Chaoyang Hospital, Beijing, China, for routine health examination. Control subjects with known CAD or any other heart disease were excluded from the study.
All study participants completed a structured questionnaire during a face-to-face interview with medical staff, and 5 ml venous blood was collected in ethylenediamine tetra-acetic acid (EDTA) coated tubes and stored at −20℃ before use. Body mass index (BMI) was calculated as weight (kg)/height (m2). Total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) levels were determined in serum. Hypertension was defined as systolic blood pressure ≥140 mmHg and/or diastolic pressure ≥90 mmHg. Diabetes was defined as a fasting plasma glucose level of ≥7 mmol/l and/or a 2-h plasma glucose level of ≥11.1 mmol/l during oral glucose tolerance testing.
The study was approved by the Ethics Committee of Beijing Chaoyang Hospital of Capital Medical University, and all participants provided written informed consent.
Genotyping
Sequences of primers used for polymerase chain reaction single base extension amplification of interleukin 6 (IL6) and IL16 single nucleotide polymorphisms (SNPs).

Statistical analyses
Continuous variables were presented as mean ± SD and analysed using the independent-samples t-test. Categorical variables were presented as n (%) of subjects and analysed using the χ2-test. The Hardy–Weinberg equilibrium and between-group comparison of genotype distribution were analysed using the χ2-test. Odds ratios (OR) and their corresponding 95% confidence intervals (CI) were used to assess the effect of each SNP on CAD risk. Multivariate logistic regression analysis was performed to calculate the OR (95% CI) after adjusting for sex, smoking status, BMI, hypertension, diabetes, TC, TG, LDL-C and HDL-C. A P-value <0.05 was considered statistically significant. All statistical analyses were performed using SPSS® software, version 11.0 (SPSS Inc., Chicago, IL, USA) for Windows®.
Results
Demographic and clinical characteristics of patients with coronary artery disease (CAD) and healthy control subjects, included in a study investigating the role of interleukin 6 (IL6) and IL16 single nucleotide polymorphisms in CAD risk.
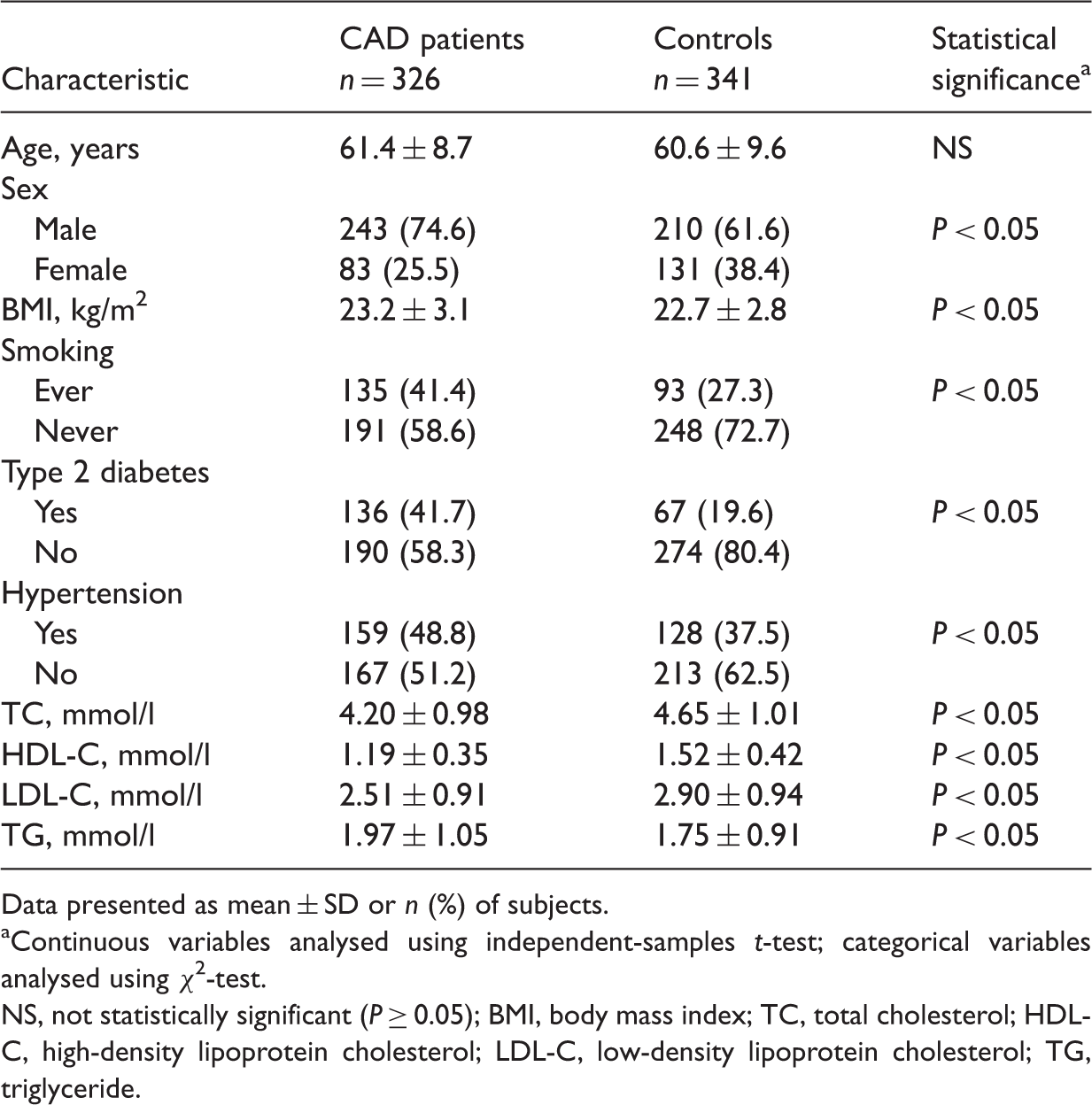
Data presented as mean ± SD or n (%) of subjects.
Continuous variables analysed using independent-samples t-test; categorical variables analysed using χ2-test.
NS, not statistically significant (P ≥ 0.05); BMI, body mass index; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, triglyceride.
Distribution of interleukin 6 (IL6) and IL16 single nucleotide polymorphisms in patients with coronary artery disease (CAD) and healthy control subjects.

Data presented as frequency or n (%) of subjects.
MAF (minor allele frequency), published at http://www.ncbi.nlm.nih.gov/snp/
χ2-test.
Wild type.
Heterozygous variant.
Homozygous variant.
NS, not statistically significant (P ≥ 0.05).
Multivariate logistic regression analysis of the effects of the interleukin 16 (IL16) single nucleotide polymorphisms rs8034928 and rs11556218 on coronary artery disease risk.

Adjusted for sex, body mass index, smoking status, diabetes, hypertension, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol and triglyceride.
Multivariate logistic regression analysis of the combined effect of the interleukin 16 (IL16) single nucleotide polymorphisms rs8034928 and rs11556218 on coronary artery disease risk.
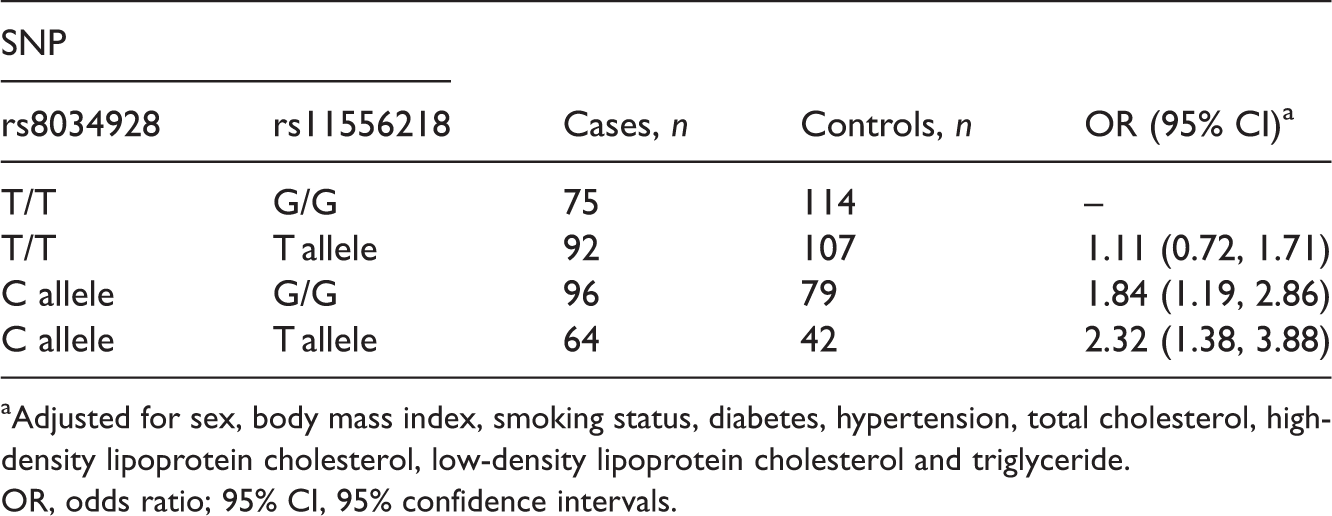
Adjusted for sex, body mass index, smoking status, diabetes, hypertension, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol and triglyceride.
OR, odds ratio; 95% CI, 95% confidence intervals.
Discussion
The IL16 SNPs rs8034928 and rs11556218 were associated with CAD risk in a Chinese Han population in the present study, but there was no relationship between IL6 rs1800795 and rs1800796, and IL16 rs3848180, rs4577037, rs1131445 or rs4778889 and CAD. These findings suggest that rs8034928 and rs11556218 may be useful genetic susceptibility markers for CAD, allowing for identification of high-risk individuals and the development of targeted therapies.
The IL16 gene contains 7 exons and 6 introns, covering approximately 12.8 kb of genomic DNA. 15 The SNPs rs11556218, rs8034928, rs3848180 and rs4577037 lie within the intron region, whereas rs1131445 and rs4778889 are located in the 3′ untranslated region. The rs11556218 SNP has been shown to be associated with allergic contact dermatitis, colorectal cancer, endometriosis, gastric cancer, systemic lupus erythematosus, nasopharyngeal carcinoma and renal cell carcinoma,10,11,16–20 in addition to CAD risk.12,21 In accordance with the present study findings, the rs11556218 TG/GG genotypes were previously associated with 1.77-fold increased risk of CAD compared with the TT genotype. 21
The rs4778889 polymorphism has been associated with Graves’ disease and asthma, 9 systemic lupus erythematosus, 11 and colorectal and gastric cancer. 10 There was no association between rs4778889 and CAD in the present study, however. This may be explained by differences in population background, the source of control subjects and sample size. Further studies are required to confirm the present findings.
A study including a large number of patients with CAD revealed significant between-group differences in rs8034928 allele frequencies, with the T/C and C/C genotypes associated with increased CAD risk. 8 These data are in accordance with the findings of the present study, where the T/C genotype was associated with a 2.14-fold increased risk of CAD, indicating that the IL16 rs8034928 T > C SNP has a role in the development of CAD.
The current study has several limitations. First, the study was conducted in a single hospital in China and the cohort may not be representative of China as a whole. Secondly, CAD is induced by multiple genes and environmental factors, none of which were considered in the present study.
In conclusion, the present study shows that rs8034928 and rs11556218 are associated with CAD risk in a Chinese population. The IL6 SNPs rs1800795 and rs1800796, and the IL16 SNPs rs3848180, rs4577037, rs1131445 and rs4778889, were not associated with CAD risk in this population. Further large-scale studies are required, to elucidate whether these IL6 and IL16 SNPs interact with environmental factors in the development of CAD.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.